All published articles of this journal are available on ScienceDirect.

Anxiety and Depression Disorder among Adult People Living with HIV/AIDS on Follow-up at Dessie Public Health Facilities Antiretroviral Therapy Clinics, Northeast Ethiopia: A Multicenter Cross-sectional Study
Abstract
Background:
Anxiety and depression are the most prevalent mental disorders among people living with HIV/AIDS compared to people without HIV/AIDS. In addition, mental health problems are associated with an increase in morbidity and mortality in people living with HIV/AIDS due to adverse effects, adherence to antiretroviral therapy, quality of life, and all health-related parameters. There is no additional study on multiple sites as an integrated way to address the proposed issue.
Objective:
This study aimed to assess the prevalence of anxiety and depression disorders and their associated factors among adult HIV-/AIDS patients on follow-up at antiretroviral therapy clinics in the Dessie town public health facility, Northeast Ethiopia.
Methods:
A multicenter institutional-based descriptive cross-sectional study design was used. Data were collected through face-to-face interviews using a structured questionnaire. Anxiety and depression disorders were assessed by using the Hospital Anxiety and Depression Scale (HADS). EPI-Data software version 7.2 for data entry and SPSS version 23 for statistical analysis were used. Statistical significance was declared at a p-value of <0.05 and an adjusted odds ratio (AOR) with a 95% confidence interval (CI) in the final model.
Results:
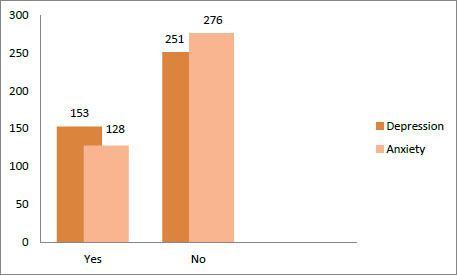
In this study, 404 adult HIV/-AIDS patients presenting for a follow-up at antiretroviral therapy clinics at Dessie town public health facilities participated; the prevalence of anxiety and depression disorders was found to be 31.7% (CI: 27%, 36.6%) and 38% (CI: 33.7%, 42.7%), respectively. Being female (AOR=3.5 95% CI: 1.86 –6.65), viral loads ≥ 1000 copies/ml (AOR =2.2, 95% CI: 1.2-3.95), and CD4 cells <200 cells/mm3 were associated with depressive disorder and HAART containing efavirenz (2.3 95% CI: 1-4.58), consumption of coffee and tea (AOR =2.5, 95% CI; 1.45 -4.37) and female gender (AOR= 3.5 95% CI; 1.9-6.6), which were found to be predictors for anxiety disorders.
Conclusion and Recommendations:
The magnitude of depression in people living with HIV/AIDS on follow-up with antiretroviral therapy was found to be higher than the pooled estimated prevalence found in Ethiopia. Being female, viral load ≥ 1000 copies/ml, and CD4 cells <200 cells/mm3 were associated with the occurrence of depressive disorders, and a HAART regimen containing efavirenz, taking coffee and tea, and female sex were found to be predictors for anxiety disorder.
1. BACKGROUND
HIV/AIDS is one of the most devastating public health problems. Globally, an estimated 36.7 million people are living with HIV/AIDS (PLWHA) [1], of which Africa contributes the highest burden of HIV infection in the world, with an estimated prevalence of 25,000,000 people in June 2016. In sub-Saharan Africa, 1.2 million people have been reported to die from this chronic and devastating disease [2]. According to the National Demographic and Health Survey (EDHS) report, 722,248 people were living with HIV and 170,000 people died from AIDS in the year 2017. Mental health problems account for 13% of the global burden of the disease as these are highly intertwined with infectious diseases, such as HIV/AIDS [1]. Millions of people with the human infectious virus (HIV) suffer from depression symptoms each year [3], which are defined as depressed mood, loss of interest or pleasure, decreased energy, feelings of guilt or low self-worth, disturbed sleep or appetite, and poor concentration [4]. Several studies show that approximately 38-55% of HIV-positive patients live in Sub-Saharan Africa, which has been associated with depressive symptoms [5-8]. In Ethiopia, the pooled estimated prevalence of depression in PLWHIV was found to be 36.65% [9], which results from the psychological impact of having a fatal disease or stems from the effects of psychosocial stressors associated with illness, such as stigma and discrimination, from actual neurological changes in the physical and chemical structures of the central nervous system that occur as a result of HIV, opportunistic infections, and related ART treatments [4]. On the other hand, anxiety is the other more prevalent mental disorder among HIV-infected individuals on ART treatment and is defined as a vague, subjective, nonspecific feeling of uneasiness, apprehension, tension (excessive nervousness), fear, a sense of impending doom, irrational avoidance of objects or situations, and anxiety attack [10]. Global systematic review reports on common mental health disorders in adults living with HIV/AIDS show that the prevalence of generalized anxiety disorder ranges from 25–33%. Anxiety among those who have recently been diagnosed with HIV is more prevalent as a result of social stigma related to their diagnosis [11], limited social support, recurrence of physical symptoms of HIV disease, encountering HIV-related stigma, and exposure to trauma or abuse [12]. As researchers have suggested, low income, unemployment, alcohol use, poor ART medication adherence, HIV/AIDS stage, perceived stigma, social support, being widowed, being female, and low educational status are risk factors associated with depression and anxiety among the HIV-infected population [13, 14].
2. METHODS
2.1. Study Setting
The study was conducted in Dessie town, which is located in the northeast 451 km from Addis Abeba (the capital city of Ethiopia) and 480 km from the Amhara regional state town (Bahirdar). According to the 2007 census, Dessie town, including Dessie woreda, has a total population of 151,174, of whom 72,932 are men and 78,242 women; 120,095 or 79.44% are urban inhabitants living in the town of Dessie, and the rest of the population is living in rural Kebeles around Dessie. In Dessie town, there are three private hospitals, six government health facilities, Dessie Compressive and Specialized Hospital, Buanboa Wuha Health Centre, segno Gebaye Health Centre, and Dessie Health Centre, which are public health facilities that provide ART services for different zones, such as the Oromia Special Zone, South Wollo, North Wollo, and partial parts of North Showa. In each health facility, there are eight ART refill OPDS, four ART pharmacies, four data clerk offices, and four VCT rooms. At the moment, there are a total of 9580 adult people living with HIV at Dessie Public health facilities antiretroviral therapy clinics, Amhara regional state, Ethiopia Ministry of Health, Ethiopia, and enrolled in ART follow-up clinic (Fig. 1).
2.2. Sample Size Determination and Sampling Procedure
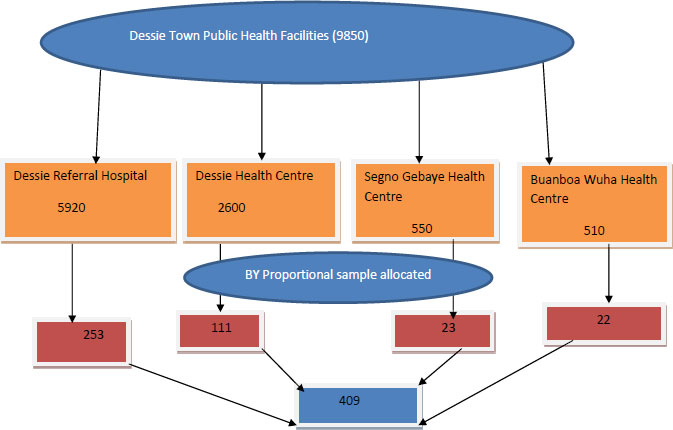
The sample size was determined by using a single population proportion formula considering the following assumptions: confidence level at 95% with a standard normal curve value of 1.96 (Zα/2 = ±1.96), a margin of error (d = 0.05), and the proportion of depression among HIV/AIDS clients attending the ART clinic in Alaret Hospital, Addis Ababa, Ethiopia (41.2%) [13]. By adding 9% of the nonresponse rate, the final sample size was 409.
After proportional allocation to each health facility, a systematic random sampling technique was employed to select the study participants. On average, 101, 43, 9, and 8 adult PLWHA visited the Dessie referral hospital, Dessie health center, Segno Gebaye health center, and Bunboa Wuha health center ART clinics per day, respectively. The data were collected for two months, and the total number of patients attending the ART clinics within two months was 4444, 1892, 946, and 352 based on the above order. The sampling interval (K-value) for each health center was determined as follows:
 for Dessie referral hospital,
for Dessie referral hospital,
 for Segno Gebaye health center,
for Segno Gebaye health center,
 for Dessie health center, and
for Dessie health center, and
 for Bunba Wuha health center were used to select each study participant.
for Bunba Wuha health center were used to select each study participant.
Based on the order in which the patients attended the follow-up, by using systematic random sampling, the study participants were selected every 11, 5, 2, and ~ 1 person pattern after determining the starting unit by the lottery method. To avoid recycling the data, special marks were used in the chart and supported by verbal confirmation of whether the patients visited in the previous four weeks (Figs. 2 and 3).
2.3. Data Collection Tools and Procedure
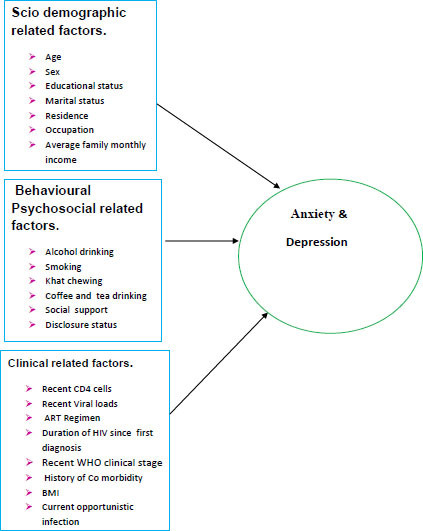
A semistructured interviewer-administered questionnaire with chart review was used to collect the data. The questionnaires included sociodemographic-related factors, clinically related factors, behavioral- and psychosocial-related factors, depression, and anxiety measurement questions. To assess depression and anxiety disorders, the Hospital Anxiety and Depression Scale (HADS) was used; it was originally developed by Zigmond and Snaith, and its validity and reliability among Ethiopian HIV-positive subjects were confirmed with Cronbach’s alpha (0.87) [15]. To measure anxiety disorder, the Hospital Anxiety Scale was used. It involves 7 Likert scale anxiety questions with 0 = not at all, 1 = occasionally, 2 = a lot of, and 3 = most of the time components ranging from 0-3 with minimum 0 and maximum 21 scores and classified as 0-8 having no anxiety disorder and >8 having an anxiety disorder; depression was measured using the same scale containing 7 Likert questions ranging from 0-3 points with a score of minimum 0 and maximum 21, with 0-8 indicating having no depression disorder, whereas score >8 indicating having a depression disorder [16].
2.4. Data Processing and Analysis
Data were coded and entered into Epi-info version 7.2.1 and then exported to SPSS version 23 for statistical analysis. Both descriptive and analytical statistical procedures were utilized. Descriptive statistics, such as percentage, mean, median, standard deviation, and interquartile range (IQR) were used depending on the nature of the data for the presentation of sociodemographic data, clinical data, and prevalence of anxiety and depression. Tables were also used for data presentation. After all, the variables fulfilled the Chi-square assumption and diagnostic collinearity, and then, binary logistic regression was used to identify factors associated with anxiety and depression disorder among HIV-infected adult patients. All explanatory variables were entered into the multivariable logistic regression model to control the possible effect of confounders by using the backward stepwise regression method. Finally, the variables that had an independent association with depression and anxiety were declared based on 95% CI and a p-value of <0.05. Model fitness was checked by using the Hosmer and Lemeshow goodness-of-fit test, which provided a value of 0.75.
| Variable | Category | Frequency (n) | Percent (%) |
| Sex | Male | 149 | 36.9 |
| Female | 255 | 63.1 | |
| Age group | 18-35 years | 202 | 50 |
| >35 years | 202 | 50 | |
| Marital status | Single | 105 | 26 |
| Married | 175 | 43.3 | |
| Divorce | 76 | 18.8 | |
| Widowed | 48 | 11.9 | - |
| Religion | Muslim | 234 | 57.92 |
| Orthodox | 165 | 40.84 | |
| Other | 5 | 1.24 | |
| Education | Un able to write and read |
111 | 27.5 |
| Primary school | 142 | 35.12 | |
| Secondary school | 92 | 22.8 | |
| College and above | 59 | 14.6 | |
| Residence | Urban | 342 | 84.7 |
| Rural | 62 | 15.3 | |
| Occupation | Daily labour | 104 | 25.3 |
| House wife | 82 | 20.3 | |
| Student | 62 | 15.3 | |
| Merchant | 56 | 13.9 | |
| Civil servant Farmer |
55 34 |
13.1 8.4 |
|
| Other | 13 | 3.2 | |
| Monthly income | ≤ 1000 birr | 254 | 62.9 |
| > 1000 birr | 150 | 37.1 |
| Variable | Category | Number (n) | Percent (%) |
| Duration HIV infection | >5 years | 257 | 63.6 |
| ≤ 5 years | 147 | 36.4 | |
| BMI | 18.5-25kg/m2 | 247 | 61.1 |
| <18 kg/m2 | 49 | 12.1 | |
| > 25 kg/m2 | 108 | 26.7 | |
| Current treatment WHO staging | Stage I | 380 | 94.1 |
| Stage II | 19 | 4.7 | |
| Stage III | 5 | 1.2 | |
| Recent CD4 cell count | 350 cell/mm3 | 248 | 61.4 |
| 200-350cell/mm3 | 76 | 18.8 | |
| < 200cell/mm3 | 80 | 19.8 | |
| Recent viral load | ≤1000copy/ml | 299 | 74 |
| >1000 copy/ml | 101 | 25 | |
| Other | 4 | 1 | |
| Current ART regimen | Efavirezbased ART regimen | 276 | 67.3 |
| Nevirapine -based ART regimen | 94 | 23.8 | |
| Lobenavier /Atazenavier based ART |
36 | 8.9 | |
| ART adherence | Good | 269 | 66.6 |
| Fair | 70 | 17.3 | |
| Poor | 65 | 16.1 | |
| History of comorbidity | Yes | 58 | 14.4 |
| No | 346 | 85.6 | |
| Current opportunistic infection | Yes | 25 | 6.2 |
| No | 379 | 93.8 |
3. RESULTS
A total of 404 participants were enrolled in this study, which yielded a 99% response rate. The mean age of the participants was 36.75 years. Nearly two-third (n=255, 63.1%) of the participants were female. Regarding their marital status, 175 (43.3%) were married, 76 (18.8%) were divorced, and 48 (11.9%) were widowed. Concerning the participants’ religion, 234 (57.9%) were Muslim and 165 (40.5%) were Orthodox. Concerning their educational status, more than one-fourth of the participants (142, 35.1%) were attending primary school, and 111 (27.5%) were unable to read and write. Regarding their residency, more than two-third of the participants, i.e., 342 (84.4%), were urban dwellers, 104 (25.7%) were daily laborers, and nearly two-third of the participants, i.e., 254 (62.9%), had a monthly income less than or equal to 1000 Birr per month (Table 1).
3.1. Clinical Characteristics of the Study Participants
Among the study participants, 257 (63.6%) had been infected with HIV for more than five years since their first diagnosis. Regarding their WHO treatment staging, the majority of the participants (380, 94.1%) were at stage one. Concerning their immunity, more than half percent of the participants, i.e., 248 (61.4), had CD4 cells greater than 350 cells/mm3, and more than two-third, 299 (74%), had viral loads less than or equal to 1000 copies/ml. Regarding their ART drugs, the majority of the participants 272 (67.3%) were taking an efavirenz-based HAART regimen, followed by 96 (23.8%), who were on the nevirapine-based regimen, while two-third of the participants, 269 (66.6%), currently had good ART drug adherence. Regarding the patients’ health status, 58 (14.4%) had comorbidities, such as kidney and liver disease, and 25 (6.2%) were currently diagnosed as having an opportunistic infection (Table 2).
3.2. Behavioral and Psychosocial Characteristics of the Study Participants
Among the study participants, 250 (61.9%) were currently living alone, half of the participants (206, 51%) were currently taking tea and coffee, and nearly 7% of the participants were taking alcohol in the last month before the data collection period; 55 (13.6%) of the participants had a history of khat chewing, and 46 (11.4%) were currently chewing khat. With respect to smoking status, 22 (5.4%) and 16 (4%) participants were in the past and currently smoking cigarettes, respectively.
3.3. Prevalence of Anxiety and Depression Disorder
3.3.1. Factors Associated with Depression Disorder
All variables were computed in bivariable and multivariable binary logistic regression analyses to test the presence of an association with anxiety and depression disorder. Regarding sociodemographic factors, females were 3.5 times more likely to develop depression disorder than their male counterparts (AOR=3.5 95% CI; 1.86 –6.65). With regards to the clinical-related factors, this study identified that adult people living with HIV with a viral load ≥ 1000 copies/ml were nearly 2.2 times more likely to develop depression than clients who had viral loads less than 1000 copies/ml (AOR =2.2, 95% CI; 1.2 -3.95). Similarly, an adult HIV-infected individual with CD4 cells <200 cells/mm3 was 3.67 times more likely to develop depression than a patient with CD4 cells greater than 350 cells/mm3 and 200-350 cells/mm3 (AOR =3.67, 95% CI; 1.85 -7.2.4).
3.3.2. Factors Associated with Anxiety Disorder
In the multivariable logistic regression analysis, the females were 3.5 times more likely to develop an anxiety disorder compared to their counterparts (AOR=3.5 95% CI; 1.9 – 6.6). Similarly, those on HAART regimen containing efavirenz were 2.3 times more likely to develop an anxiety disorder compared to those on non-efavirenz-containing HAART regimen and another ART regimen (AOR =2.3, 95% CI; 1.4 -4.58), and those taking coffee and tea were 2.5 times more likely to develop an anxiety disorder compared to those who have not taken coffee and tea (AOR =2.5, 95% CI; 1.4 -4.3) (Tables 3 and 4).
| Variable | Category | Frequency | Percent (%) |
| Social support | Yes No |
250 154 |
61.9 38.1 |
| Khat chewed status | Never chewed | 303 | 75 |
| Former chewed | 55 | 13.6 | |
| Current chewed | 46 | 11.4 | |
| Alcohol drink status | Yes | 28 | 6.9 |
| No | 376 | 93.1 | |
| Smoking status | Never Smoked | 366 | 90.6 |
| Former smoked | 22 | 5.4 | |
| Current smoked | 16 | 4 |
| Variables | Depression Disorder | Anxiety Disorder | Depression Disorder | Anxiety Disorder | ||||
| Sex | Yes | No | Yes | No | COR(95%CI) | AOR(95%CI) | COR (95%CI) | AOR (95%CI) |
| Male | 32 | 117 | 29 | 120 | 1 | - | 1 | - |
| Female | 121 | 134 | 99 | 156 | 3.3(2.08,5.24) | 3.5(1.86,6.65) * | 2.6 (1.63,4) | 3.5 (1.9,6.6)* |
| Age | - | - | - | - | - | - | - | - |
| ≤35 years | 59 | 143 | 54 | 148 | 1 | - | 1 | - |
| >35 years | 94 | 108 | 74 | 128 | 2.14(1.4,3.2) | - | 1.6(1.03,2.4) | - |
| Marital Status | - | - | - | - | - | - | - | - |
| Married | 59 | 116 | 38 | 67 | 1 | - | 1 | - |
| Unmarried | 40 | 65 | 50 | 125 | 1.2 (0.7,2) | - | 1.4 (0.8,2.4) | - |
| Divorce | 32 | 44 | 23 | 53 | 1.4 (0.8,2.5) | - | 1 (0.6,2) | - |
| Widow | 22 | 26 | 17 | 31 | 1.7(0.9,3.2) | - | 1.4 (0.7,2.7) | - |
| Education | - | - | - | - | - | - | - | - |
| Lower education level | 112 | 112 | 89 | 164 | 1 | - | 1 | - |
| Higher education level | 110 | 41 | 39 | 112 | .47(0.3,0.7) | - | .6 (0.4,1) | - |
| Residence | - | - | - | - | - | - | - | - |
| Rural | 20 | 42 | 14 | 48 | 1 | - | 1 | - |
| Urban | 133 | 209 | 114 | 228 | 1.33(0.75,2.3) | - | 1.7 (0.9,3.2) | - |
| Employment | - | - | - | - | - | - | - | - |
| Had no job | 25 | 50 | 22 | 53 | .78(.463,1.33) | - | .87 (.50,1.51) | - |
| Had job | 128 | 201 | 106 | 223 | 1 | - | 1 | - |
| Family average monthly income | - | - | - | - | Depression Disorder |
Anxiety Disorder |
||
| COR(95%CI) | AOR(95%CI) | COR(95%CI) | AOR(95%CI) | |||||
| >1000 birr | 59 | 91 | 49 | 101 | 1 | - | 1 | - |
| ≤1000 birr | 94 | 160 | 79 | 175 | 0.90(.6,1.37) | - | .93(.6-1.43) | - |
| BMI | - | - | - | - | - | - | - | - |
| 18.5-25 | 74 | 172 | 55 | 191 | 1 | 1 | 1 | - |
| <18.5 | 13 | 36 | 13 | 36 | .8(.4,1.7) | 1.9(.83,4.4) | 1.3(.62,2.5) | 1.9(.8,4) |
| >25 | 66 | 43 | 60 | 49 | 3.6(2.2,5) | 1.5(0.66,5.44) | 4.3(2.6,6.9) | 2(0.86,6.6) |
| Taking coffee and tea | - | - | - | - | - | - | - | - |
| No | 60 | 138 | 45 | 153 | 1 | - | 1 | - |
| Yes | 93 | 113 | 83 | 123 | 1.9(1.28,2.8) | 1.9(0.2,3.3) | 2.3(1.5,3.4) | 2.5(1.45,4.37) |
| Smoking Status | - | - | - | - | - | - | - | - |
| Never smoked | 124 | 242 | 100 | 266 | 1 | - | 1 | - |
| Current smoked | 13 | 3 | 12 | 4 | 8.5(2.4,30) | - | 8(2.5,25) | 1.2(0.5,32) |
| Past smoked | 16 | 6 | 16 | 6 | 5(2,13.6) | - | 7(2.7,18.6) | 4(0.6,37.6) |
| Khat chewing | - | - | - | - | - | - | - | - |
| Never chewed | 93 | 210 | 75 | 228 | 1 | - | 1 | - |
| Currently chewed | 31 | 15 | 29 | 17 | 2.5(1.4,4.5) | 2.3(0.1,4.7 ) | 2.4(1.3,4.2) | 2(0.5,4.4) |
| Past chewed | 29 | 26 | 24 | 31 | 4.7(2.4,9) | 2.5(0.2,5.7) | 5.1(2.7,10) | 3.86(0.7,8.67) |
| Alcohol drinking status | - | - | - | - | - | - | - | - |
| No | 141 | 235 | 115 | 261 | 1 | - | 1 | - |
| Yes | 12 | 16 | 13 | 15 | 1.3(.6,2.7) | - | 2(.9,4.2) | - |
| Current ART regimen | - | - | - | - | - | - | - | - |
|
Nevirapine
contain |
29 | 67 | 22 | 74 | 1 | - | 1 | - |
| Efaverize contain regimen | 108 | 164 | 93 | 179 | 1.5(0.9,2.5) | - | 1.7(1,3) | 2.3( 1,4.58) * |
| Other regimen | 16 | 20 | 13 | 23 | 1.8(.4,4) | - | 1.9(.8,4.3) | - |
| ART drug adherence | - | - | - | - | - | - | - | - |
| Good | 108 | 231 | 92 | 247 | 1 | - | 1 | - |
| Poor | 45 | 20 | 36 | 29 | 4.8 (2.7,8.5) | 3.7(0.8,7.7) | 3(1.9,5.7) | - |
| Duration of HIV infection | - | - | - | - | - | - | - | - |
| ≤ 5 | 43 | 104 | 33 | 114 | 1 | - | 1 | - |
| > 5 years | 110 | 147 | 95 | 162 | 1.8(1.2,2.8) | - | 2(1.3,3) | - |
| Viral loads | - | - | - | - | - | - | - | - |
| <1000 copies/ml | 88 | 221 | 73 | 226 | 1 | - | 1 | - |
| ≥1000 copies/ml | 65 | 36 | 55 | 46 | 4,3(2.7,7) | 2.3(1.3,4.2) * | 3.7(2.3,6) | 2(0.2,4) |
| CD4 cells | - | - | - | - | - | - | - | - |
| >350 cells/m3 | 80 | 168 | 58 | 190 | 1 | - | 1 | - |
| 200-350 cells/mm3 | 24 | 52 | 25 | 51 | .96(.6,1.7) | - | 1.6(.8,2.8) | - |
| <200 cells/mm3 | 49 | 29 | 45 | 35 | 3.3 (2,5.6) | 2.1(1.1,4) * | 4.4(2.5,7) | 3.67(0.86,7.2) |
| WHO stage | - | - | - | - | - | - | - | - |
| Stage I | 142 | 237 | 121 | 259 | 1 | - | 1 | - |
| Stage II&III | 10 | 14 | 7 | 17 | 1.2(.5,2.7) | - | .9(.4,2) | - |
| Opportunistic infection | - | - | - | - | - | - | - | - |
| No | 139 | 240 | 115 | 264 | 1 | - | 1 | - |
| Yes | 14 | 11 | 13 | 12 | 2.2(.97,4.7) | - | 2.5(2.1,5.6) | - |
| Discloser status | - | - | - | - | - | - | - | - |
| Yes | 127 | 235 | 109 | 253 | 1 | - | 1 | - |
| No | 26 | 16 | 19 | 23 | 3(1.6,5.8) | - | 1.9(1,3.7) | - |
| Live alone | - | - | - | - | - | - | - | - |
| No | 48 | 202 | 34 | 216 | 1 | 1 | - | |
| Yes | 105 | 49 | 94 | 60 | 9(5.7,14 | - | 10(6,16) | - |
| Comorbidity disease | - | - | - | - | - | - | - | - |
| No | 123 | 223 | 105 | 241 | 1 | - | 1 | - |
| Yes | 30 | 28 | 23 | 35 | 1.4(1.1,3.4) | - | 1.5(.85,2.7) | - |
4. DISCUSSION
The prevalence of depression in the present study was found to be 38%. Regarding the prevalence, the current study’s result is in line with other studies carried out in two areas of Ethiopia, in which the prevalence estimates were reported to be 41.2% and 32% [13, 14]. On the other hand, the present study’s findings were found to be lower than those of studies performed in Gondar, Ethiopia, China, and southern India, in which the prevalence was reported to be 60%, 66.3%, and 90%, respectively [17-19]. In the current study, the prevalence of depression was higher than that in studies conducted in Harer, Ethiopia, Uganda, Nigeria, Brazil, and Melbourne. The variation may be due to the use of different sample sizes and measurement tools in Ethiopia (5.8%, DASS tool, 107 participants), Uganda (8.1%, MINI-Plus, 618 participants), Nigeria (24.6%, DSM-IV, 130 participants), Brazil (5.8%, HADS, 406 participants), and Melbourne (21.7%, Inventory to Diagnose Depression Disorder, 322 participants) [17, 20-23]. Regarding associated factors, females were 3.5 times more likely to develop depression disorder than their male counterparts (AOR=3.5 95% CI; 1.86 –6.65). A positive association between female gender and depression disorder in HIV/AIDS has previously been reported in Africa [21]. Females typically have a two to three times higher rate of depressive disorders than men. Female victims are more exposed to traumatic experiences, such as sexual, physical, and emotional abuse, both in childhood and adulthood [24]. From the clinical-related factors, this study identified that adult people living with HIV with a viral load ≥ 1000 copies/ml were nearly 2.2 times more likely to develop depression than those who had viral loads less than 1000 copies/ml (AOR =2.2, 95% CI; 1.2 -3.95). This finding was supported by a study performed at Mount Sinai Hospital, New York city [25]. With respect to human immunodeficiency virus infection, individuals with a high viral load were more likely to have higher anxiety or depression scores on the HADS, because those with a high viral load were significantly more depressed than patients with better control of their HIV infection. This study indicated that HIV-infected individuals with CD4 cells < 200 cells/mm3 were 3.67 more likely to develop depression than HIV-infected individuals with CD4 cells 350 cells/mm3 and 200-350 cells/mm3 (AOR =3.67, 95% CI; 1.85 -7.2.4). This finding was also supported by the study conducted at Mount Sinai Hospital, New York city [25].
In the current study, the prevalence of anxiety was found to be 31.7% (CI 27%, 36.6%). This result is in line with other studies carried out in two areas of Ethiopia and New York city [13, 14, 25], in which the prevalence was reported to be 32.4%, 34.4%, and 34.4%, respectively. On the other hand, the current study's finding has been found to be lower than the studies done in Albania [26], in which the prevalence was reported to be 82.3%. In Albania, only 79 HIV-infected individuals participated by using extra web material that was used to measure anxiety disorder; these findings have been found to be higher than the studies done in Brazil with12.6% [22], at Debretabor hospital, Ethiopia, with 22.2% [27], and Nigeria with 25.6% [17], respectively. The above prevalence variations might be due to the difference in sample size and the use of different measurement tools used to assess anxiety disorder. In Ethiopia and Brazil, BAI greater than or equal to 22 has been used with 436 and 346 study participants, respectively. In Nigeria, the Generalized Anxiety Disorder (GAD-7) scale has been used with a cut-off of ≥ 5 for 350 study participants.
In this study, females were 3.5 times more likely to develop anxiety disorders than their male counterparts, and this result was supported by studies conducted in Ethiopia [27], Brazil [22], and China [18]. Females exposed to acute life experiences, low social interaction, and less social support from friends and families might be at increased risk of anxiety disorders. Similarly, those on a HAART regimen containing efavirenz were 2.3 times more likely to develop an anxiety disorder compared to those using non-efavirenz-containing and other HAART regimens (AOR =2.3, 95% CI; 1.4 -4.58). This finding has been supported by another study [28].
Finally, from behavioral and psychosocially related factors, HIV-infected individuals who took coffee and tea were 2.5 times more likely to have anxiety symptoms compared to people who had not taken coffee and tea (AOR =2.5, 95% CI; 1.4 -4.3). This finding has been supported by a previous study [29]. Caffeine has anxiogenic effects in both experimental and realistic situations, which may be due to increased levels of lactate in the brain. Another study found the neuropsychiatric effects of caffeine to be mediated largely by the blockade of adenosine A1 and adenosine 2A receptors in the central nervous system, which has a direct linkage with the dopaminergic system, specifically with the adenosine A2 receptor [30], which stimulates inhibitory GABA adrenergic neurons in pathways. The blockade of adenosine receptors also reverses the inhibition of adrenaline release in the sympathetic nervous system, which results in sympathetic stimulation.
LIMITATIONS
In the current study, substances, such as alcohol, cigarettes, khat, and coffee/tea were not measured quantitatively. Moreover, this study is cross-sectional, thereby providing weak evidence for evaluating the cause-and-effect relationship.
CONCLUSION
The findings of this study have shown the magnitude of depression in people living with HIV/AIDS to be higher than the pooled estimated prevalence found in Ethiopia on follow-up at Dessie town public health facility antiretroviral therapy clinics. Therefore, healthcare providers working in the ART care service centers should pay strong attention to female patients, and those with viral loads ≥ 1000 copies/ml and CD4 cells <200 cells/mm3, for assessing depression disorder, and also to patients taking the HAART regimen containing efavirenz, coffee and tea, to assess anxiety disorders in these individuals and provide mental health care services as early as possible in order to improve mental health among people living with HIV/AIDS.
LIST OF ABBREVIATIONS
| ART | = Antiretroviral Therapy |
| BMI | = Body Mass Index |
| CD4 | = Cluster of Differentiation |
| CNS | = Central Nervous System |
| EFV | = Efavirenz |
| HADS | = Hospital Anxiety-Depression Scale |
| PLWHA | = People living with HIV and AIDS |
| USA | = United States of America |
| WHO | = World Health Organization |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the Research Ethical Review Committee of the School of Nursing, College of Medicine and Health Sciences on behalf of the University of Gondar Review Board. Then, an official letter was submitted to the Dessie town public health facilities administrative. Data collection was performed after obtaining permission.
HUMAN AND ANIMAL RIGHTS
Participation was completely voluntary, and an informed written consent was obtained from all study subjects after in-depth clarification about the objective of the study. All information obtained throughout the study was kept confidential.
CONSENT FOR PUBLICATION
The study does not include images or videos relating to an individual. However, concerning the data collected and used in this study, while obtaining consent from each participant, information related to publishing the study findings was addressed, and participants agreed to it.
STANDARDS OF REPORTING
COREQ guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
The datasets used and/or analysed during the current study are available from the corresponding author [F.S.D] upon reasonable request.
FUNDING
This research did not receive any grants from any funding agency in the public, commercial, or not-for-profit sectors.
ACKNOWLEDGEMENTS
The author would like to express gratitude to the University of Gondar College of Medicine and Health Sciences Research and Ethical Review Committee for the approval of the ethical clearance, and would like to thank data collectors and supervisors for their commitment and the study participants for their valuable information.

