All published articles of this journal are available on ScienceDirect.

HIV RNA and HCV RNA Levels, and Mortality: The Japan Cohort Study of HIV Patients Infected through Blood Products
Authors Info & Affiliations
Abstract
Background:
Most hemophiliacs living with HIV are co-infected with HCV. In their clinical practice, the long-term effects of anti-HIV and anti-HCV therapies have not been sufficiently investigated.
Objective:
This study aimed to evaluate changes in HIV RNA and HCV RNA levels and the prognosis in hemophiliacs living with HIV over 24 years in Japan.
Methods:
We used cohort study data of 578 hemophiliacs living with HIV. We analyzed trends in HIV RNA levels between the fiscal years 1997 and 2008 (first follow-up), and trends in HIV RNA and HCV RNA levels between the fiscal years 2009 and 2020 (second follow-up). Mortality rates by HIV RNA and HCV RNA levels were calculated from 11,207 observed person-years and 194 deaths.
Results:
The percentage of HIV RNA levels <400 copies/mL rose in the first period of follow-up, and the percentage of HCV RNA-negative rose in the second period of follow-up. The participants with HIV RNA levels <400 copies/mL had a significantly lower mortality rate than the others, with a ratio of 0.46 in the first period. HCV antibody-positive participants who were HCV RNA-negative had a significantly lower mortality rate than those who were HCV RNA-positive, with a ratio of 0.47 in the second period.
Conclusion:
After the introduction of combination anti-HIV therapy over 24 years in hemophiliacs living with HIV, HIV RNA levels decreased in the first half of this period, resulting in decreased mortality. Additionally, HCV RNA levels decreased in the second half of this study period, resulting in even further decreased mortality.
1. INTRODUCTION
Combination anti-human immunodeficiency virus (HIV) therapies that were started in the late 1990s reduced HIV RNA levels greatly improved the prognosis in HIV-positive individuals in many countries [1-4]. Anti-hepatitis C virus (HCV) treatment has made great progress approximately since 2010. This progress has led to the expansion of HCV RNA-negative conversion in individuals living with HCV [5-7]. Anti-HIV and anti-HCV therapies have changed and advanced over the years.
In the mid-1980s, many hemophiliacs became infected with HIV through contaminated blood products [8, 9]. Most hemophiliacs living with HIV were co-infected with HCV. For many years, hemophiliacs living with HIV co-infected with HCV were taking anti-HIV therapies and anti-HCV therapies. These therapies were probably appropriate at the time. The long-term effects of anti-HIV therapies and anti-HCV therapies in such actual clinical settings have not been sufficiently investigated [9, 10].
In Japan, 1,432 cases have been reported to be infected with HIV through blood products [11]. A research program for these HIV-positive individuals has been carried out since the fiscal year 1993 with the support of the Ministry of Health, Labour and Welfare [12, 13]. The Japan Cohort Study of HIV Patients Infected through Blood Products, which was based on this program, was started at the same time [14].
The present study aimed to evaluate changes in HIV RNA and HCV RNA levels and the prognosis in hemophiliacs living with HIV in a real-world setting in Japan. This study covered 24 years after the introduction of combination anti-HIV therapy in the fiscal year 1997. We used data from the Japan Cohort Study of HIV Patients Infected through Blood Products.
2. MATERIALS AND METHODS
2.1. The Japan Cohort Study of HIV Patients Infected through Blood Products
A research program for people with HIV infection from contaminated blood coagulation factor products started in the fiscal year 1993 in Japan. This program is intended to help prevent these people from developing HIV-infected symptoms in daily living by providing health management expenses [12, 13]. In this program, participants were requested to submit reports filled out by their treatment physician. Some items in the report are quarterly, including HIV RNA levels, the CD4 cell count, and anti-HIV therapy, while others are annual, including HCV RNA levels and a history of anti-HCV therapy. When participants in this program develop acquired immunodeficiency syndrome (AIDS), they are transferred to another program for the relief of side effects of blood products and are followed until death. As of 1st April 1997, many people infected with HIV from blood products were participating in this program (approximately 80%) [12, 14]. Follow-up of participants until death by the end of the fiscal year 2020 was complete. The Japan Cohort Study of HIV Patients Infected through Blood Products, which was based on this program, was started at the same time. Details of the cohort study are described elsewhere [12-14].
2.2. Data Analysis
The data from the cohort study mentioned above were collected, including sex, age, CD4 cell count, HIV RNA levels, anti-HIV therapy, HCV antibody and HCV RNA levels, anti-HCV therapy, and the date of death [12, 14]. No personal identifiers, such as the name or address, were included. We created a subset cohort from that data for our analysis. The cohort consisted of 578 male hemophiliac patients on 1 April 1997, who had been infected with HIV by blood products in the 1980s [4, 12]. The follow-up was 24 years between the fiscal years 1997 and 2020 based on the above-mentioned program. The follow-up was divided into two periods of 12 years, comprising fiscal years 1997–2008 (first period of follow-up) and fiscal years 2009–2020 (second period of follow-up) owing to the availability of HCV RNA data.
We analyzed the characteristics of the participants. These characteristics included age, CD4 cell count, and anti-HIV therapy at baseline in the first period of follow-up. These characteristics also included the variables in the first period of follow-up plus HCV antibody and a history of anti-HCV therapy at baseline and at the end of the second period of follow-up. Anti-HIV therapy was classified into six categories as follows: no regimen, regimens including two nucleoside reverse transcriptase inhibitors (NRTIs), regimens including two NRTIs and one or two protease inhibitors (two NRTIs + PI[s]), regimens including two NRTIs and one non-nucleoside reverse transcriptase inhibitor (two NRTIs + NNRTI), regimens including two NRTIs and one integrase strand transfer inhibitor (two NRTIs + INSTI), and other regimens. Anti-HCV therapy included interferon therapy, direct-acting anti-HCV drug therapy, and their combination therapy.
We analyzed trends in HIV RNA levels in the first and second periods of follow-up, and trends in HCV RNA levels in the second period of follow-up. HIV RNA levels by quarter were categorized as < 400 copies/mL (detection limit in the 1997 HIV RNA test) and ≥ 400 copies/mL in the first period of follow-up and < 50 copies/mL (detection limit in the 2009 HIV RNA test) and ≥ 50 copies/mL in the second period of follow-up. HCV RNA levels in HCV antibody-positive participants by the fiscal year were categorized as positive and negative. We assumed that an HCV RNA-negative status would continue thereafter.
Mortality rates by HIV RNA and HCV RNA levels were calculated from observed person-years and deaths in each of the first and second periods of follow-up. HIV RNA and HCV RNA levels at death were assumed to be those of the previous year. A binomial test was used to compare mortality rates, assuming that the number of deaths followed a Poisson distribution. All analyses were performed using the SAS statistical package, version 9.4 (SAS, Institute, Cary, NC, USA).
3. RESULTS
Table 1 shows the characteristics of the participants in the first and second periods of follow-up. The participants comprised 578 men with a mean age of 29.4 years at baseline in the first period of follow-up. The number of participants was reduced by 127 deaths to 451 at the end of the first period of follow-up. The number of participants was reduced by 67 deaths from 451 at baseline to 384 at the end of the second period of follow-up. The mean CD4 cell count increased from 344.6 cells/μL at baseline in the first period of follow-up to 465.3 cells/μL at baseline to 530.7 cells/μL at the end of the second period of follow-up.
Table 1.
| Characteristics of Participants | First Period of Follow-up | Second Period of Follow-up | |||||||
|---|---|---|---|---|---|---|---|---|---|
| At Baseline | At Baseline | At the end of the Follow-up | |||||||
| Age (years), n, mean, and standard deviation | 578 | 29.4 | 9.6 | 451 | 39.6 | 8.1 | 384 | 50.7 | 7.4 |
| CD4 cell count (cells/μL), n, mean, and standard deviation | 502 | 344.6 | 199.7 | 389 | 465.3 | 236.9 | 277 | 530.7 | 252.6 |
| Anti-HIV regimen use, n, %#1 | |||||||||
| No regimen | 138 | 26.6 | - | 62 | 14.9 | - | 7 | 2.1 | - |
| Two NRTIs | 206 | 39.8 | - | 20 | 4.8 | - | 1 | 0.3 | - |
| Two NRTIs + PI(s) | 89 | 17.2 | - | 180 | 43.3 | - | 13 | 3.9 | - |
| Two NRTIs + NNRTI | 0 | 0.0 | - | 81 | 19.5 | - | 21 | 6.3 | - |
| Two NRTIs + INSTI | 0 | 0.0 | - | 16 | 3.8 | - | 215 | 64.8 | - |
| Other regimens | 85 | 16.4 | - | 57 | 13.7 | - | 75 | 22.6 | - |
| Unknown | 60 | - | - | 35 | - | - | 52 | - | - |
| HCV antibody, n, %#1 | |||||||||
| Positive | - | - | - | 421 | 96.6 | - | 359 | 96.8 | - |
| Negative | - | - | - | 15 | 3.4 | - | 12 | 3.2 | - |
| Unknown | 578 | - | - | 15 | - | - | 13 | - | - |
| History of anti-HCV treatment, n, %#2 | |||||||||
| Yes | - | - | - | 223 | 57.3 | - | 261 | 79.3 | - |
| No | - | - | - | 166 | 42.7 | - | 68 | 20.7 | - |
| Unknown | 578 | - | - | 32 | - | - | 30 | - | - |
Two NRTIs + PI(s): regimens including two NRTIs and one or two protease inhibitors.
Two NRTIs + NNRTI: regimens including two NRTIs and one non-nucleoside reverse transcriptase inhibitor.
Two NRTIs + INSTI: regimens including two NRTIs and one integrase strand transfer inhibitor.
#1 Unknown data were excluded from percentage calculations.
#2 Data used were only HCV antibody-positive. Unknown data were excluded from percentage calculations.
The proportion of using no regimen of anti-HIV treatment decreased from 26.6% to 2.1% in the first and second periods of follow-up. In the first period of follow-up, the proportion of using Two NRTIs decreased from 39.8% to 4.8%. However, the proportion of using two NRTIs + PI(s) increased from 17.2% to 43.3%, and the proportion of using two NRTIs + NNRTI increased from 0.0% to 19.5% in the first period of follow-up. In the second period of follow-up, the proportion of using two NRTIs + PI(s) and two NRTIs + NNRTI decreased, while the proportion of using two NRTIs + INSTI increased from 3.8% to 64.8%. A total of 96.6% of participants were HCV antibody-positive at baseline in the second period of follow-up. The proportion of HCV antibody-positive participants with a history of anti-HCV therapy increased from 57.3% to 79.3% in the second period of follow-up.
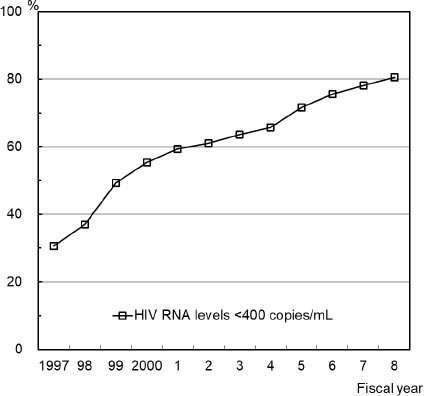
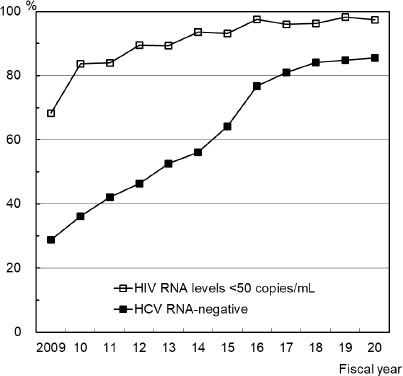
Fig. (1) shows the percentage of participants with HIV RNA levels <400 copies/mL in the first period of follow-up. This percentage steadily rose from 30.7% to 80.6% in the first period of follow-up. Fig. (2) shows the percentage of participants with HIV RNA levels <50 copies/mL and the percentage of HCV RNA-negative participants who were HCV antibody-positive in the second period of follow-up. The percentage of participants with HIV RNA levels <50 copies/mL was >80% in 2010, >95% in 2016, and high over the second period of follow-up. The percentage of HCV RNA-negative participants who were HCV antibody-positive steadily rose from 28.7% to 85.5% in the second period of follow-up.
| - | Person-years | No. of Deaths |
Mortality Rate (per 100 Person-years) |
Ratio of Mortality Rates | P-value |
|---|---|---|---|---|---|
| First period of follow-up | |||||
| Total | 6237.9 | 127 | 2.04 | - | - |
| - | - | - | - | - | - |
| HIV RNA levels <400 copies/mL | 2811.2 | 35 | 1.25 | 0.46 | <0.001 |
| HIV RNA levels ≥400 copies/mL | 2364.9 | 64 | 2.71 | 1.00 | - |
| - | - | - | - | - | - |
| Second period of follow-up | |||||
| Total | 4968.9 | 67 | 1.35 | - | - |
| - | - | - | - | - | - |
| HIV RNA levels <50 copies/mL | 3801.6 | 49 | 1.29 | 0.57 | 0.118 |
| HIV RNA levels ≥50 copies/mL | 398.6 | 9 | 2.26 | 1.00 | - |
| - | - | - | - | - | - |
| HCV RNA-negative of HCV antibody-positive | 2972.3 | 28 | 0.94 | 0.47 | 0.002 |
| HCV RNA-positive of HCV antibody-positive | 1684.9 | 34 | 2.02 | 1.00 | - |
Table 2 shows the person-years, number of deaths, and mortality rate by HIV RNA and HCV RNA levels in the first and second periods of follow-up. There were 127 deaths of 6,237.9 person-years and 67 deaths of 4,968.9 person-years in the first and second periods of follow-up, respectively. The mortality rate per 100 person-years significantly decreased from 2.04 in the first period of follow-up to 1.35 in the second period of follow-up (p < 0.001). The participants with HIV RNA levels < 400 copies/mL had a significantly lower mortality rate than those with HIV RNA levels ≥ 400 copies/mL, with a ratio of 0.46 in the first period of follow-up (p < 0.001). Those with HIV RNA levels < 50 copies/mL had a lower mortality rate than those with HIV RNA levels ≥ 50 copies/mL, with a ratio of 0.57 in the second period of follow-up, but this was not significant. HCV antibody-positive participants who were HCV RNA-negative had a significantly lower mortality rate than those who were HCV RNA-positive, with a ratio of 0.47 in the second period of follow-up (p=0.002).
4. DISCUSSION
This study showed that, during the 12 years since the introduction of combination anti-HIV therapy in 1997, there was a rapid decline in HIV RNA levels and an association between HIV RNA levels and the prognosis in hemophiliacs living with HIV. These results are likely to be due to the well-known effects of combination anti-HIV therapy [1-4]. During the next 12-year period between the fiscal years 2009 and 2020, we observed a decrease in two NRTIs + PI(s) use and two NRTIs + NNRTI use, an increase in two NRTIs + INSTI use, and a sustained low HIV RNA level. These findings are likely to be due to subsequent advances in anti-HIV therapy and its appropriate application to hemophiliacs living with HIV in Japan [14, 15]. A prognostic difference in HIV RNA levels during this period was observed as found during the preceding 12-year period, but this difference was not significant. This phenomenon may be due to fewer observed person-years of high HIV RNA levels owing to the maintenance of low HIV RNA levels.
In this study, we observed a sharp increase in the HCV RNA-negative rate among HCV antibody-positive participants during the 12-year period between fiscal years 2009 and 2020. During this period, there were important advances in anti-HCV therapy. Combination therapy with interferon and direct-acting anti-HCV drugs was introduced in 2011, and direct-acting anti-HCV drug therapy without interferon was introduced in 2014 [16]. Strong effects of these therapies on HCV RNA-negative conversion have been reported [6, 7]. The development of such anti-HCV therapy and its rapid application to hemophiliacs living with HIV and HCV may have affected the increase in HCV RNA-negative conversion.
We found an association between HCV RNA levels and the prognosis in the second period of follow-up and a significantly improved prognosis between the first and second periods of follow-up. This finding suggested that HCV RNA-negative conversion led to an improved prognosis in hemophiliacs living with both HIV and HCV [10, 17]. Additionally, this finding indicated that HCV RNA-negative conversion greatly contributed to the improvement of the prognosis for all hemophiliacs living with HIV during this period.
This study has some limitations. We used data from the Japan Cohort Study of HIV Patients Infected through Blood Products, which was based on a research project with the support of the Ministry of Health, Labour and Welfare of Japan [12, 13]. The data used in the present study were limited to those collected in this research project. Data such as HCV RNA and HIV RNA levels were reported by the participants’ physicians and included some missing values owing to non-reporting. Data on anti-HIV therapy at the time of reporting may have been fairly accurate because most reporting physicians were probably responsible for the participants’ HIV treatment at that time. However, because some of the physicians might not have been responsible for the HCV treatment of the participants, the data on a history of anti-HCV therapy may not always have been accurate. Therefore, this possible inaccuracy may have led to an underestimation of the proportion of those with a history of anti-HCV therapy [12, 14]. HIV RNA testing methods changed during this period [4, 18]. The classification of HIV RNA level data used was based on the detection limits of HIV RNA tests at baseline in 1997 and in 2009 for each of the first and second periods of follow-up, respectively [14]. Trends in HCV RNA were observed only in the second period of follow-up owing to the availability of the data. There was great progress in anti-HCV therapy during this period. Detailed data on anti-HCV treatment regimens in the first and second follow-up periods were not available. Our assumption that an HCV RNA-negative status would continue thereafter must be valid because of almost no new HCV infections with blood products [19]. We showed mortality rates during the first and second periods of follow-up but did not show mortality rates by year because of low precision owing to the small number of deaths. Data on HIV RNA and HCV RNA levels at death were not available. Therefore, those from the year before death were used in our analysis. To analyze the association of HIV RNA and HCV RNA with mortality, the person-year method was used to estimate mortality rates by HIV RNA and HCV RNA levels. The application of more sophisticated survival analysis methods may be appropriate.
Because follow-up of our participants until death was complete, survival or death data were accurate, and mortality rates could be calculated correctly for all participants who were followed up. However, mortality rates by HIV RNA and HCV RNA were calculated from fewer observed person-years because of missing data for HIV RNA and HCV RNA levels (Table 2). Cause-specific mortality rates could not be calculated because no cause-of-death data were available [12, 13]. An analysis of the cause of death will be an important issue in future research [20].
CONCLUSION
Twenty-four years after the introduction of combination anti-HIV therapy for hemophiliacs living with HIV, HIV RNA levels decreased in the first half of this period, resulting in a decreased mortality rate. Furthermore, HCV RNA levels decreased in the second half of this period, resulting in an even lower mortality rate.
AUTHORS’ CONTRIBUTION
All authors have made significant contributions to the manuscript. MK, MM, and S Hashimoto conceived the idea, wrote the proposal, analyzed the data, and drafted the manuscript. HY, KA, HG and SO interpreted the analysis. TS, S Higasa, MO, and GO reviewed and edited the manuscript. All authors contributed to a critical review of the draft and approved the final manuscript.
LIST OF ABBREVIATIONS
| RNA | = Ribonucleic Acid |
| HIV | = Human Immunodeficiency Virus |
| HCV | = Hepatitis C Virus |
| NRTIs | = Nucleoside/nucleotide Reverse Transcriptase Inhibitors |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved in July 2022 by the Ethical Review Board for Clinical Studies of National Hospital Organization Osaka National Hospital, Osaka, Japan (No. 15026).
HUMAN AND ANIMAL RIGHTS
No animals were used for studies that are the basis of this research. All the humans used were in accordance with the Helsinki Declaration of 1975.
CONSENT FOR PUBLICATION
This study was based on the Japan Cohort Study of HIV Patients Infected through Blood Products. Anonymity and confidentiality as well as data protection were guaranteed.
STANDARDS OF REPORTING
The STROBE guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available on request from the corresponding author, [MK]. The data are not publicly available due to their containing information that could compromise the privacy of research participants.
FUNDING
This study was supported by the Yu-ai Welfare Foundation (Public Interest Incorporated Foundation) in Japan.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

