All published articles of this journal are available on ScienceDirect.

High Incidence and Predictors of Loss to Follow-up among Children and Adolescents on Life Long Antiretroviral Therapy in the Conflict-affected Northwest and Southwest Regions of Cameroon: A Retrospective Cohort Study
Authors Info & Affiliations
Abstract
Background:
Retention in care and transition to adulthood are critical for children and adolescents living with HIV on Antiretroviral Therapy (ART) in HIV treatment programs in Sub Sahara, Africa.
Objective:
This study aimed to determine the incidence and predictors of loss-to-follow-up (LTFU) in the context of the ongoing crisis caused by an armed conflict in the Northwest and Southwest Regions of Cameroon, where staff in HIV treatment programs faced unique challenges of retention of children/adolescents.
Methods:
We employed a multi-stage mixed method design in which we conducted a retrospective cohort study to determine incidence and risk factors for LTFU through data abstraction from medical records of children and adolescents from five (5) ART treatment centers, followed by seventeen (17) key informant interviews conducted with healthcare workers to gain further insights into the reasons for LTFU among children and adolescents enrolled between January 2018 to December 2021. Kaplan–Meier plots were used to determine the probability of LTFU as a function of time. The Cox regression model was used to measure predictors of LTFU. Endpoint-recorded interviews were transcribed, translated, and analyzed using Atlas-ti Version 9.
Results:
A total of 1,030 children and adolescents (p-y) were enrolled for follow-up. 138 (13.4%) were LTFU, with an overall incidence rate of 33.0 LTFU per 1000 person years. Survival probability decreased for younger children and older adolescents. Receiving care in a rural health facility (AHR:2.14 (1.23-3.76), non-biological caregivers (AHR: 2.44; 95% CI: 1.59-3.74), short duration on ART, being on a sub-optimal regimen (AHR: 17.83; 95% CI: 11.00-29.00) and long distances to health facility (AHR:2.05; 95% CI: 1.10-3.20) were significant predictors of LTFU. Multiple Caregivers (94.1%), long distances/cost of transportation (88.2%), socio-political crises (75.5%), peer pressure, refusal, dating and marriage among adolescents (70.5%), stigma (64.7%), competitive life activities (58.8%), lack of timely disclosure (53%), poverty/lack of partner/family support (48.2%), lack of understanding on the disease process (47.0%), alternative forms of health care (29.4%), and shortage of ARVs (13.8%) were reasons for poor retention from the interviews.
Conclusion:
The overall incidence rate of LTFU was 33.0 per 1000 person years for children and adolescents initiated on lifelong ART over a period of four (4) years in the conflict-affected areas. The study portrays the need for innovative, multifaceted strategies to mitigate the predictors of this high-risk LTFU in displaced populations in the context of a sociopolitical crisis.
1. INTRODUCTION
The Acquired Immunodeficiency Syndrome (AIDS) pandemic remains the most serious of infectious diseases in public health [1]. Cameroon is a country located in Sub-Saharan Africa (SSA) with a population of about 23.34 million [2], with an estimated 491,834 people living with HIV in 2021 [3]. In Cameroon, HIV prevalence for the population ages 0-14 and 15-49 are 0.2% and 3.4%, respectively [4]. The epidemiological burden of HIV in Cameroon is decreasing (from 4.3% in 2011 to 3.4% in 2018) [5]. At a country level, this progress is largely due to efforts in implementing the Prevention of Mother-To-Child Transmission (PMTCT) option B+ since 2014, the “Test and Treat” strategy since 2016, HIV early infant diagnosis since 2007 and increasing viral load coverage. However, mortality and LTFU in HIV programs are ongoing challenges to the scaling up of HIV management in children and adolescents, the rates and determinants of which vary by health facility [6], Retention in care is particularly challenging in pediatric HIV treatment programs in SSA where the proportion of children LTFU has been estimated to be around 9–14% during the first year of treatment and up to 28% during the second year of treatment [7]. Despite notable achievements, challenges remain throughout the treatment cascade, particularly in retaining patients in long-term care and maintaining viral suppression [7]. Opportunities to retain children within the cascade are missed at each step, and the risk of mortality is especially high in the first 90 days following ART initiation [7]. Studies in SSA describe high rates of LTFU once children have entered care [8-10]. Sociopolitical instability can further hamper or affect disease prevention and control programs as well as the accessibility to health facilities. Political instability may take the acute forms of armed conflict, violent regime change, or politically motivated assassinations [10]. Achieving high retention rates is central to the UNAIDS “95-95-95” targets, especially since 95% of HIV-infected people will receive sustained ART and 95% will have viral load suppression. In this study, we used routine sociodemographic and clinical data to describe LTFU and identify risk factors for LTFU among children and adolescents receiving ART in some selected treatment centers in the NW and SW regions of Cameroon. The Northwest and Southwest Regions continue to have a large number of unstable populations, including PLHIV caregivers, mainly due to the exactions of the armed conflict [6]. Previous studies have shown that the absence or cessation of ARV treatment can lead to a deterioration in clinical condition, a drop in immunity and an increase in viral load in patients who are LTFU [7, 8]. This contributes to an increase in morbidity and mortality related to HIV infection and to the development of resistance to antiretroviral drugs (ARVs) [7, 8]. Thus, our study was aimed at identifying the incidence and context-specific predictors of LTFU among children and adolescents through the assessment of their records and the perceptions of healthcare workers (key informants) from the treatment centers for more insights on the possible reasons for LTFU in children and adolescents, for possible mitigation and overall retention in care in this priority population.
2. MATERIALS AND METHODS
2.1. Study Design and Setting
This was a retrospective cohort study that employed both qualitative and quantitative methods of data collection. Study sites constituted five ART treatment centers (three in the NW and two in the SW) regions in Cameroon, serving a large population. These treatment centers were each selected from five different health districts in the two regions of Cameroon, and thus clustering or group effect was minimized. The two regions have been in an armed conflict since 2017, and clashes continue from time to time to this day. The health facilities provided comprehensive healthcare services, including HIV prevention and treatment and were purposefully selected to include urban, semi-urban and rural populations. The records of children and adolescents who were LTFU and those who resumed ART after documented LTFU between January 2018 and December 2021 were assessed.
2.2. Study Participants/Duration
The study was carried out in five HIV treatment centers, each hosting a pediatric unit with children and adolescents enrolled in HIV care. Records of all children and adolescents who were on treatment or LTFU between January 2018 and December 2021 were reviewed. Children and adolescents 0-19 years with complete information in their records were included, while those with incomplete information in their records on LTFU as the major outcome of interest were excluded from the study. The study also recruited healthcare providers working in the HIV/AIDS pediatric clinics for the qualitative portion. Both quantitative and qualitative studies were conducted from November 2021 to March 2022.
2.3. Sample Size Determination and Sampling Procedures
We retrospectively analyzed medical records (n = 1,030) from a cohort of all children 0–9 years (355) and adolescents 10–19 years (675) living with HIV and on ART between January 2018 and December 2021, from the five healthcare facilities, who were followed for treatment outcomes. Treatment centers which were all faith-based institutions were purposively selected to include urban, semi-urban and rural populations. Furthermore, purposive sampling was used to select key informants in the various pediatric units for the in-depth interviews.
2.4. Data Collection
2.4.1. Quantitative Data Collection
A data extraction checklist was used to obtain information from the records of children and adolescents from the files, ART registers and electronic database in the five health facilities. The checklist was developed to capture socio-demographic, clinical, and treatment-related variables. The predictor variables assessed were baseline socio-demographic factors (sex, age, educational status, residence, main daily caregiver, occupation of caregiver, the mother still alive, the father still alive, presence of phone number, HIV status of caregiver, marital status, distance from health facility) and base-line clinical and treatment-related factors (baseline CD4 count, past opportunistic infections, recent weight, type of regimen at the start of ART, regimen at LTFU, regimen switch if any, duration on ART, isoniazid preventive therapy, WHO clinical stage at treatment initiation, most recent viral load, and history of TB infection). Data were collected by trained research assistants who triangulated from individual files, ART registers, and the electronic database.
2.4.2. Qualitative Data Collection
Qualitative data was collected through in-depth interviews with key informants (KIs) who were facility healthcare workers. Interviews were conducted by one of the authors using in-depth interview guides and transcripts cross-validated by another author. Seventeen KIs interviews were held with health care workers who were assigned the duty to cover follow-up of the children and adolescents who were LTFU at least once during the cohort period. Audio recordings from Key Informants Interviews (KIIs) were taken by the research team during the interactions, with informed consent from the respondents. The interviews were held at quiet locations at the health facilities and by phone with strict respect for confidentiality. On average, an interview took about 30–45 minutes. Questions were asked, beginning from general to very specific questions. KIs were further probed with questions based on the main reasons for ART attrition in children and adolescents enrolled in the health facilities.
2.5. Main Outcomes and Secondary Outcomes
The main outcome of interest was the first LTFU defined as not seen or reached for >90 days and not known to have been transferred out of the clinic to another or died during the study period. Secondary outcomes were documented, transferred out and died. We examined these outcomes among all children and adolescents in the cohort.
2.6. Data Processing and Analysis
Quantitative data was inputted into an Excel sheet, cleaned, and exported into SPSS vs. 26 for analysis. Data analysis was also done using the R software. A descriptive analysis of socio-demographic and baseline clinical characteristics was done using counts and percentages for all categorical variables. The person-years of observation (pyo) were also calculated and used to determine the incidence of LTFU, mortality and transferred-out rates per 1000 pyo. Kaplan–Meier curve was used to estimate median survival time. The Cox regression analysis was done to assess the factors associated with time on ART to LTFU among children and adolescents. History of ART adherence was classified into good, fair, and poor according to the number of daily doses missed for children on once-daily doses and twice-daily doses and the percentage summerised. For children on once-daily doses, adherence was classified as Good (≥95% or 1 pill missed per month), Fair (90–95% or 2-3 pills missed per month), or Poor (less than 90% or > 3 pills missed per month). For children on twice daily doses, adherence was classified as Good (≥95% or 2 pills missed per month), Fair (90–95% or 3-6 pills missed per month), or Poor (less than 90% or 3-6 pills missed per month).
After qualitative data collection, all interviews were verbatim transcribed for analysis using thematic areas. The transcribed data was reviewed and cross-validated by another team member. Then, coding and interpretation were done by CWA, followed by validation by EMK for reliability and validity. The coding was done using social-ecological guidelines [11, 12] to assess individual and external parameters of LTFU. Data analyses were conducted using an inductive method of content analysis based on emerging themes (personal, family, community, and health system parameters). The main grouped themes used were: perceptions and experiences of healthcare providers on the causes of attrition rates in children and adolescents and understanding of the importance of ART adherence.
3. RESULTS
3.1. Socio-demographic Characteristics of Children and Adolescents on ART
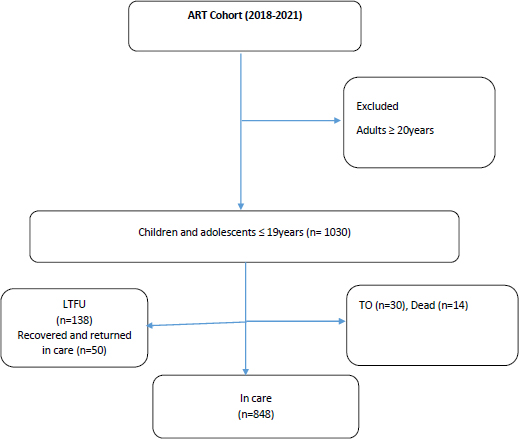
The cohort was observed for 1,030 children/adolescents, with 138 (13.4%) of them LTFU. Out of the 138 participants LTFU, fifty (50) were recovered and reengaged in care. At the end of follow-up, 848 (82.3%) HIV-infected children and adolescents were in care (Fig. 1). More than half (55.5%) of the participants were females. The median age of the children and adolescents was 12 ± 4.82 years. More adolescents (10-19 years) (61.0%) were present in the cohort compared to children 0-9 years (39.0%), with most of the participants, 342(33.0%), being older adolescents of age group 15-19 years. Close to half of the study participants had a primary level of education, 559 (49%). More than half, 604 (59%) of the children and adolescents lived with their parents as their main caregivers, with 377 (37%) of these caregivers having a secondary level of education. About a third of the caregivers, 365 (35%), were farmers (Table 1).
| Characteristic | Frequency | Percentage |
|---|---|---|
| Gender | - | - |
| Male | 464 | 45.0 |
| Female | 566 | 55.0 |
| Age category | - | - |
| 0-4 | 96 | 9.3 |
| 5-9 | 259 | 25.1 |
| 10-14 | 333 | 32.3 |
| 15-19 | 342 | 33.2 |
| Level of Education | - | - |
| Primary | 559 | 54.3 |
| Secondary | 272 | 26.4 |
| Tertiary | 32 | 3.1 |
| No Formal Education | 74 | 37.2 |
| Not of school age | 47 | 4.6 |
| Missing values | 46 | 4.5 |
| Health Facility | - | - |
| HF 1 | 275 | 26.7 |
| HF 2 | 270 | 26.2 |
| HF 3 | 49 | 4.8 |
| HF 4 | 103 | 10.0 |
| HF 5 | 333 | 32.3 |
| Residence | - | - |
| Urban | 407 | 39.5 |
| Rural | 396 | 38.4 |
| Semi-urban | 227 | 22.0 |
| Main Daily Caregiver | - | - |
| Parents | 604 | 58.6 |
| Relatives | 209 | 20.3 |
| Grandparents | 70 | 6.8 |
| Siblings | 38 | 3.7 |
| Missing Values | 109 | 10.6 |
| Caregiver’s Level of Education | - | - |
| No formal education | 39 | 3.8 |
| Primary | 351 | 34.1 |
| Secondary | 377 | 36.6 |
| Tertiary | 81 | 7.9 |
| Missing Values | 182 | 17.7 |
| Caregiver’s occupation | - | - |
| Farmer | 365 | 35.4 |
| Business | 206 | 20.0 |
| Hairdresser | 65 | 6.3 |
| Tailor | 61 | 5.9 |
| Unemployed | 34 | 3.3 |
| Others | 30 | 2.9 |
| Driver | 25 | 2.4 |
| Teaching | 25 | 2.4 |
| HCW | 21 | 2.0 |
| Builder | 24 | 2.3 |
| Missing Values | 174 | 16.9 |
| Distance to HF | - | - |
| <20km | 740 | 71.8 |
| 20-50km | 197 | 19.1 |
| >50km | 81 | 7.9 |
| Missing Values | 12 | 1.2 |
| Characteristic | Frequency | Percentage |
|---|---|---|
| WHO stage | - | - |
| Stage I | 357 | 34.7 |
| Stage II | 221 | 21.5 |
| Stage III | 237 | 23.0 |
| Stage IV | 92 | 8.9 |
| Missing Values | 123 | 11.9 |
| CD4 count(cells/ml) | - | - |
| <200 | 62 | 6.0 |
| 200-499 | 114 | 11.1 |
| ≥500 | 304 | 29.5 |
| Unknown | 550 | 53.4 |
| ART regimen | - | - |
| ABC+3TC+DTG | 146 | 14.2 |
| AZT+3TC+NVP | 62 | 6.0 |
| ABC+3TC+LPV/r | 135 | 13.1 |
| ABC+3TC+EFV | 33 | 3.2 |
| TDF+3TC+DTG | 497 | 48.3 |
| TDF+3TC+EFV | 48 | 4.7 |
| Others | 109 | 10.6 |
| History of ART adherence | - | - |
| Good | 686 | 66.6 |
| Fair | 194 | 18.8 |
| Poor | 120 | 11.7 |
| Missing Values | 30 | 2.9 |
| HIV status of caregiver | - | - |
| Positive | 586 | 56.9 |
| Negative | 128 | 12.4 |
| Unknown | 316 | 30.7 |
3.2. Baseline Clinical Characteristics of HIV-positive Children and Adolescents on ART
About a third (34.7%) of the children and adolescents in the cohort had WHO clinical stage I, 357 (34.7%). A total of 304(29.5%) had a baseline CD4 count greater than or equal to 500 cells/ml. Close to half of the adolescents (497 [48.3%]) were on a Dolutegravir-based regimen. Many of the study participants, 686 (66.6%), recorded a good history of adherence to ART as seen in records and as reported by healthcare workers. More than half of the caregivers, 586 (56.9%), were aware of their own HIV status as positive (Table 2).
3.3. Proportion of Children and Adolescents LTFU
A total of 138 HIV-positive children and adolescents were LTFU. Of the 138, 79(57.2%) were children 0-9 years, while 59 (42.8%) were adolescents 10-19 (Older adolescents (15-19years) and constituted 33 (24%) of those LTFU. A total of 50 (36.2%) children and adolescents recovered and reengaged in care.
3.4. Incidence of Loss to Follow-Up of Children and Adolescents Aggregated by Gender, Age group and Treatment Centerss from January 1, 2018, to December 31, 2021
The overall incidence of LTFU in children and adolescents was 33 LTFU per 1000 children/adolescent years, while the incidence of death was 3 deaths per 1000 children/adolescent years, and those transferred out (TO) was 7 per 1000 children/adolescent years. Over this period, 138(13.4) were LTFU, 14(1.4%) patients died, and overall attrition was 152 (14.8%). LTFU occurred more in females 76 (7.4%) than in males, while the proportion was more in children 5–9 years old, 44 (4.3%) than in any other age group. Based on the health facility, the proportion was more at health facility 1, 53 (5.1%) in a rural setting than in any other health facility (Table 3).
3.5. Time until Loss to Follow-Up Among ART Attending Children and Adolescents on ART from January 1, 2018, to December 31, 2021
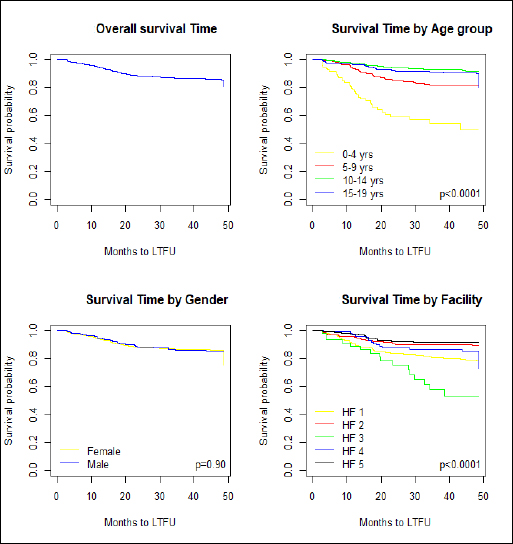
In this study, all children and adolescents on treatment between Jan 2018 and Sept 2021 were enrolled and followed until December 2021 for the occurrence of the event of interest (LTFU). Children and adolescents who exited or completed the study without the occurrence of the event of interest were censored. The minimum and maximum follow-up period was three months and forty-eight months, respectively (Fig. 2). The overall cumulative survival probability at the end of the 10th month was 0.96 (95% CI: 0.95- 0.97), while it was 0.89 (95% CI: 0.88-0.92) and 0.87 (95% CI: 0.85- 0.89) at the 20th and 30th follow-up month, respectively. In addition, the cumulative survival probability at the 40th and 48th follow-up months was 0.86 (95% CI: 0.84-0.88) and 0.86 (95% CI: 0.83, 0.88), respectively (Fig. 1). The survival probability significantly decreased for children 0-4 years, followed by children in the 5-9 years category and older adolescents 15-19 years. There was no statistically significant difference in survival probability for females and males. The survival probability significantly decreased for HF1 and HF3 treatment centers.
| Variable | n (%) | LTFU (%) | Died (%) | TO (%) |
|---|---|---|---|---|
| Total | 1030(100) | 138(13.4) | 14(1.4) | 30(2.9) |
| Gender | - | - | - | - |
| Female | 566(55) | 76(7.4) | 7(0.7) | 16(1.6) |
| Male | 464(45) | 62(6.0) | 7(0.7) | 14(1.4) |
| Age group | - | - | - | - |
| 0 - 4 | 96(9) | 35(3.4) | 4(0.4) | 0 |
| 5 - 9 | 259(25) | 44(4.3) | 2(0.2) | 7(0.7) |
| 10 - 14 | 333(32) | 26(2.5) | 3(0.3) | 7(0.7) |
| 15 - 19 | 342(33) | 33(3.2) | 5(0.5) | 16(1.6) |
| Health facility | - | - | - | |
| HF1 | 275(27) | 53(5.1) | 4(0.4) | 17(1.7) |
| HF2 | 270(26) | 27(2.6) | 1(0.1) | 5(0.5) |
| HF3 | 49(5) | 16(1.6) | 0 | 2(0.2) |
| HF4 | 103(10) | 15(1.5) | 0 | 1(0.1) |
| HF5 | 333(32) | 27(2.6) | 9(0.9) | 5(0.5) |
3.6. Predictors of Loss to Follow-up among Children and Adolescents
In our study, the following significant variables in univariate analysis were included in the Cox proportional hazard multivariable model: residence, type of caregiver, having a registered phone number for follow-up calls, type of ART regimen, the experience of regimen change, history of ART adherence, duration on ART, and the approximate distance between home and health facility. A P-value of less than 0.05 as a cutoff point was considered statistically significant. Children and adolescents in care at the HF1 treatment center had a two times higher risk of loss to follow-up (AHR: 2.14; 95% CI:1.23-3.76) than their counterparts at HF5. Similarly, children and adolescents receiving care at the HF2 in a rural setting had a two times higher risk of loss to follow-up (AHR: 2.51; 95% CI: 1.40-4.53) compared with their counterparts at the HF5. In addition, children and adolescents in care at HF4 had a two times higher risk of loss to follow-up (AHR: 2.02; 95% CI: 0.98-4.17) than their counterparts at HF5. The risk of LTFU in children of 5-9 years (AHR: 0.55; 95% CI: 0.31-0.98) and adolescents of 10-14 (AHR: 0.25; 95% CI: 0.13-0.49), 15-19 (AHR: 0.34; 95% CI: 0.18-0.64) was lower compared with children of 0-4 years. The risk of LTFU among ART-attending children and adolescents who had non-biological caregivers was two times higher as compared with their counterparts who had primary biological caregivers (AHR: 2.44; 95% CI: 1.59-3.74). The risk of LTFU in children and adolescents on sub-optimal regimens (AHR: 17.83; 95% CI: 11.00-29.00) and other (AHR: 6.83; 95% CI: 3.85-12.14) regimens was very high compared with those on the optimal regimen. Children and adolescents with a history of good adherence had a lower risk of LTFU (AHR: 0.52; 95% CI: 0.35-0.77) than their counterparts with poor or fair adherence. The risk of LTFU in children and adolescents with a prolonged duration on ART, i.e., 13-24 months (AHR: 0.38; 95% CI: 0.19-0.74) and 25+ months (AHR: 0.20; 95% CI: 0.11-0.33) was lower compared with those with ≤12 months duration on ART. ART-attending children and adolescents who had more than fifty kilometers distance between their homes and the health facility had a two times higher risk of loss to follow-up as compared with their counterparts who had less than twenty kilometers distance from home to the health facility (AHR: 2.05; 95% CI: 1.10-3.20) (Table 4).
| Variable | Event | Censored | CHR(95%CI) | AHR(95%CI) | P-value |
|---|---|---|---|---|---|
| Gender | |||||
| Male | 62 | 402 | 1.00 | 1.00 | |
| Female | 76 | 490 | 1.02 (0.70-1.38) | 1.03 (0.70-1.51) | 0.8751 |
| Health Facility | |||||
| HF 5 | 27 | 306 | 1.00 | 1.00 | |
| HF 1 | 53 | 222 | 2.74 (1.73-4.36) | 2.14 (1.23-3.76) | 0.0081* |
| HF 2 | 27 | 243 | 1.58 (0.92-2.69) | 2.51 (1.40-4.53) | 0.0022* |
| HF 3 | 16 | 33 | 7.57 (4.10-14.13) | 1.38 (0.71-2.69) | 0.3466 |
| HF 4 | 15 | 88 | 1.71 (0.91-3.21) | 2.02 (0.98-4.17) | 0.0567* |
| Age Category | |||||
| 0-4 | 35 | 61 | 1.00 | 1.00 | |
| 5-9 | 44 | 215 | 0.40 (0.25-0.62) | 0.55 (0.31-0.98) | 0.0412* |
| 10-14 | 26 | 307 | 0.17 (0.10-0.29) | 0.25 (0.13-0.49) | <0.0001* |
| 15-19 | 33 | 309 | 0.22 (0.14-0.36) | 0.34 (0.18-0.64) | 0.0008* |
| Residence | |||||
| Urban | 37 | 370 | 1.00 | 1.00 | |
| Rural | 77 | 319 | 2.24 (1.52-3.32) | 1.37 (0.87-2.17) | 0.1793 |
| Semi-urban | 24 | 203 | 1.15 (0.69-1.93) | 1.46 (0.84-2.55) | 0.1886 |
| Main Daily Caregiver | |||||
| Biological | 76 | 560 | 1.00 | 1.00 | |
| Non-biological | 33 | 186 | 1.55 (1.10-2.17) | 2.44 (1.59-3.74) | <0.0001* |
| Cell Phone | |||||
| Yes | 122 | 868 | 1.00 | 1.00 | |
| No | 16 | 24 | 3.84 (2.28-6.48) | 1.40 (0.78-2.49) | 0.2598 |
| Type of ART Regimen | |||||
| Optimal | 29 | 749 | 1.00 | 1.00 | |
| Sub optimal | 83 | 59 | 26.35 (17.18-40.39) | 17.83 (11.00-29.00) | <0.0001* |
| Others | 26 | 84 | 7.32 (4.31-12.44) | 6.83 (3.85-12.14) | <0.0001* |
| Experience of Regimen Change | |||||
| No | 106 | 794 | 1.00 | 1.00 | |
| Yes | 28 | 98 | 1.80 (1.19-2.73) | 1.01 (0.61-1.63) | 0.8846 |
| History of ART Adherence | |||||
| Poor/Fair | 73 | 241 | 1.00 | 1.00 | |
| Good | 62 | 624 | 0.35 (0.25-0.48) | 0.52 (0.35-0.77) | 0.0008* |
| Duration on ART in Months | |||||
| ≤12 months | 28 | 48 | 1.00 | 1.00 | |
| 13 - 24 months | 25 | 67 | 0.52 (0.30-0.89) | 0.38 (0.19-0.74) | 0.0042* |
| 25+ months | 85 | 777 | 0.17 (0.12-0.26) | 0.20 (0.11-0.33) | <0.0001* |
| Approximate distance to health facility | |||||
| <20km | 74 | 666 | 1.00 | 1.00 | |
| 20-50km | 32 | 165 | 1.64 (1.10-2.48) | 1.20 (0.74-1.99) | 0.4798 |
| >50km | 32 | 49 | 4.99 (3.30-7.57) | 2.05 (1.10-3.20) | 0.0285* |
3.7. Reasons for Poor Retention in Children and Adolescents
3.7.1. Multiple Caregivers
Findings from the integrated content analysis showed that nearly all (94.1%) of the key informants at the pediatric treatment centers reported poor retention in children and adolescents associated with multiple caregivers. According to the key informant, children constantly switch from one caregiver to another, and sometimes the transition is done without prior notification at the ART clinic, which makes it difficult for them to trace even when they visit the communities. Extracts from some key informants are given below:
“the main pressing cause of loss to follow up among children here is the rampant change of caregivers. He/she is no longer with the grandmother, and is now with the aunt, the aunt is no longer taking good care of the child and is now with one uncle who may not even be aware of the child’s condition, and this shifting from one place to another subsequently leads to LTFU….” (Health facility 1 Male-KI3).
“Many of the children in care do not live with their biological parents as most of them are orphans, they are so unstable, and they keep changing from one caregiver to another, which causes poor retention in so many of them…”. (Health facility 3 Female-KI2).
3.7.2. Long Distances/Cost of Transportation
This study also showed that some clients had to travel a long distance from home to the health facility with their children or adolescents for clinical appointments or ARV refills. This was evident in many of the responses from the KIs (88.2%) from the frequency of the integrated content analysis. According to the responses, most parents and guardians complained of living in very far-off places. Sometimes they did not even have money at all or sufficient amounts to travel to and from the HF and as such they had to miss clinic appointments, as reported by some KIs:
“…. most of our clients come from very far-off communities, and these children need to come to the facility very often; they are not like adults, and they need to be followed up, but distance is a serious issue affecting retention in this age category. For example, a child or adolescent lives in Baiye-Pania, Mbonge, Baikoke and sometimes transport is about 15000frs - 20000frs and their caregivers cannot afford that often, and this has affected retention in them a lot….” (Health facility 2 Female-KI1).
“Many of the children and adolescents here, their caregivers are peasant farmers who live in nearby villages, sometimes they even pay 3000frs to come to the health facility, they are unable and what the clinic reimburse is not really sufficient to cover very high transport costs or half of that amount, and this has affected them coming to the clinic here……..(Health facility 3 Male-KI1).
3.7.3. Sociopolitical Crises/Displacement
Integrated content analysis showed that 75.5% of the responses as the reasons for loss to follow-up in children and adolescents were linked with sociopolitical crises in the Northwest and Southwest regions of Cameroon and displacements for educational purposes as a result of school lockdown. According to the key informants, there have been frequent confrontations between the military and the separatists and most of the time; there is constant blockage of roads. This has caused difficulty for these caregivers as sometimes they cannot access the health facility with their children to continue their care. Still, in the context of this crises, KIs say several schools have been shut down, and many of these children and adolescents have been displaced for schooling purposes without any notification at the clinic. In some localities, KIs say these children and adolescents have been displaced for safety into bushes and cannot be traced again. Some adolescents do not have identification cards and cannot come to the health facilities. Below are examples of quotes from some KIs:
…sometimes, when there are serious gunshots, many of them start running into the bushes, you will follow the location plan they gave, and when you get there, they are in the bushes, you cannot trace them again, and with time, they are LTFU. Last time our community team went for outreach with files and ARVs to serve them, but they came back because they could not trace these children or the adolescents because they were in the bushes…. (Health facility 2 Female-KI3).
“…. many of the children and adolescents whom we cannot trace back to care have been displaced due to the crises for schooling purposes since schools have been shut down in this area. You even visit the community, they will tell you they no longer live here, and they are schooling at so and so place. Some adolescents do not have ID cards, and for fear of the military, they do not come to the health facility……………… (Health facility 4 Male-KI3).
3.7.4. Peer Pressure, Refusal, Dating and Marriage among Adolescents
Nearly 3/4 (70.5%) of the KIs from the in-depth interviews said peer pressure, desire to start dating or entering into marriage or co-habiting without letting the other partner know their sero-statuses were reasons for missed appointments among adolescents. KIs also indicated that peer pressure among adolescents has led to smoking, promiscuity, drinking, gambling, reckless living and stubbornness toward parents and guardians, which has caused some of them to drop out of care. Below are examples of such quotes from KIs:
“…. many of the adolescents here, out of peer pressure, have started dating, others drink and smoke, and when we reach out to them to remind them of their rendezvous, they will tell us that they will not come because they are dating and do not want to be seen in the hospital. Some go into cohabiting and marriage without their parent’s concern. Sometimes you even visit their homes, and their parents will tell you they have not seen this one in two weeks, they have not seen this other one for one week, and subsequently, they cannot be traced anymore. This peer pressure and promiscuous lifestyle among adolescents is the highest problem that has caused poor retention for us here…” (Health Facility 5 Female-KI2).
………. we have a 16-year-old adolescent who came back here with a whole bag of medications, telling us she will not take her medications again and asking why she is taking medications when she is not sick…..even though she was already disclosed she keeps refusing to take, as she said if her mother did not die that means she too will not die and will not take again……(Health facility 4 Female-KI5).
3.7.5. Stigma
Findings from in-depth interviews showed that 64.7% of the respondents cited stigma among adolescents and some caregivers as the reason for poor retention in children and adolescents, especially among adolescents. According to the respondents, when most adolescents become aware of their status, and age transition, they start feeling shy to come to the treatment center as they do not want to be seen. For some children, their parents still feel stigmatized and do not want their child to be seen at the treatment center frequently, so they tend to shy away from treatment, as seen below:
“…. stigma is also a serious issue here that has affected retention, especially in our adolescents. For example, we have two of our adolescents who will always come into the clinic through this path (nurse pointing to the opposite direction of the main entrance into the treatment center). They do not come like this (still pointing); they use this downer section, which shows that it is a problem they are still feeling stigmatized. I tried talking with them, but even when they come, they feel uncomfortable sitting on the cue here in front of the center, and most often they miss several appointments” (Health facility 2 female-KI2).
“.. some children and adolescents live in homes with relatives or relative’s homes with multiple children, they feel shy taking the medication, and this has led to poor retention. Also, some caregivers do not want their children to be seen in the hospital or known in the community for taking ARVs which has affected retention as well…. (Health facility 1 female-KI4).
3.7.6. Competitive Life Activities
Results from the integrated content analysis showed that 58.8% of the respondents indicated loss to follow-up among children and adolescents associated with caregivers and adolescents themselves being involved in other activities, such as job, business, learning a trade or schooling linked with poor retention in children, as most often they say they do not have time to bring the child to the ART clinic for some time because they were engaged in one activity or another as seen below:
“…with the advent of the crises, Saturday has officially become a school day, and most adolescents attend schools and do not come to the clinic, especially during examination periods. Some caregivers value their businesses more than the health of the child; they are the only breadwinners and tend to put food on the table for their children, so they prefer to go about their business and not bring the child even for months…..”……(Health facility 4 female-KI4)
“…..many of the adolescents are engaged in other activities that they are doing like schooling, apprenticeship, businesses and most of the time, they find it difficult to come to the health facility. So you find them missing their rendezvous, and subsequently, they are LTFU. For example, some of them are apprentices, and you will hear them say, ‘I have gone to work in Bamenda.’ They have gone to work in Bafoussam, but when it is time for medication, it is not possible for them to come. They will say they are coming, and they do not end up coming for long periods, even without salvage…….(Health facility 3 Male-KI1).
3.7.7. Lack of Timely Disclosure
According to healthcare providers (53%), some caregivers do not disclose their status to their children and adolescents at the appropriate time, and because they do not understand why they are taking these ARVs, they default. According to them, why should they be taking medications when they are feeling well? Below are examples of such quotes:
“…. we still have some adolescents who are 15, 16 years and they do not know why they are on medications, and their caregivers are not willing to disclose to them on time. They are like, I am very healthy, but why am I taking medications? Some come here to collect medications because they are afraid of their parents, and when they go back home, they do not take them. When you ask them to bring their drugs so that you can do a pill count, you will see some of them bring a whole pack back to you, and when their parents are not around, they do not come to the health facility at all…….” (Health facility 4 male-KI4).
“……disclosure is not done at the appropriate time, and some children and adolescents keep asking why they are taking the medication. They only take when their parents are around. If the parents are not around, especially the adolescents, they do not continue treatment and will become ill since they do not know why they are taking it….” (Health facility 2 female-KI2).
3.7.8. Poverty/Lack of Partner/Family Support
Integrated content analysis from KIs (41.2%) indicated that poverty and lack of family support, especially for relatives as caregivers and single parents, were linked with poor retention in children and adolescents on ART. According to their responses, caregivers and adolescents come to the health facility complaining of no money to buy the appropriate diet or food supplements needed for the child. Sometimes the caregivers or adolescents are the ones taking care of the entire family, and with poverty and shortages of food, it is difficult to continue in care. Lack of family support, both psychological and financial, was associated with dropout in care. Below are examples of such quotes:
“…. some caregivers say that their families and spouses do not give them the right support to keep bringing these children to the health facility. For example, the mother of a child came here and was complaining that the child’s father doesn’t care about them and, most often, he is not around and sometimes, when she is sick, she pleads with the husband to bring the child to the hospital which he doesn’t………….”(Health facility 1 femaile-K1
“……some caregivers come here complaining of not having enough money to take care of the children, especially in cases where the relative has her own biological child and the orphaned child to take care of. We have many cases like that who are just peasant farmers who depend on their farms to take care of these children, which is not sufficient to extend for the nutritional needs or maintain this other child in care which has negatively affected retention in them...”(Health facility 5 femaile-K3).
3.7.9. Lack of Understanding of the Disease Process and Treatment
Close to half of the healthcare workers (47.0%) reported a poor understanding of the HIV disease process/treatment as the reason for poor retention in care for some children and adolescents. Some KIs said many caregivers, especially those living with children who are orphans, do not really understand the concept of HIV, disease progression, nor the importance of adherence to treatment as some believe the treatment has a short duration. This poor understanding causes poor retention in these children, as seen in the in-depth interview below:
“……some caregivers feel that since this HIV is in children, with time, it will get better or go away completely. For example, I was talking with a child’s aunt this morning, and she was asking me when this sickness will go away in her niece? So many of them are not informed or are ignorant about the disease and the importance of adherence in children. We do our best to educate them on this, but you will educate one caregiver now and in the next couple of months, that child has another caregiver who will not know about the disease process nor take the child’s adherence seriously, and this affects the child’s retention in care. So when they do not understand the care and treatment that much, it also affects their retention and good adherence…...” (Health facility 3 female-KI2).
“………some of them start bringing their children for treatment, and after a while, especially when their children or adolescents themselves feel better, they stop taking the treatment. This is ignorant as they will tell you their children are fine now and do not need to continue with their medications….” (Health facility 2 Female-KI1)
3.7.10. Alternative Forms of Healthcare
Some KIs (29.4%) reported the loss to follow-up among children and adolescents associated with seeking alternative forms of healthcare, such as religious and traditional healers. Due to these alternatives, they stopped coming to the health facility. Some caregivers believe that since their children have been prayed for, they are healed and need no ARVs. According to key informants, some caregivers and adolescents visit traditional healers who are told that HIV has a spiritual origin and, therefore, must be treated spiritually. As a result, they default from treatment, as seen from the in-depth interviews below:
“…….we have parents who do not bring their children to the hospital again because they believe they have been healed through prayers. For example, we tried reaching this father because he was no longer bringing his daughter to the treatment center for 2 years now, but he told us that his daughter was no longer taking the treatment because she had been healed. We have also had cases in which some parents take herbs and also take their children to these herbal practitioners who claim they can treat the disease………….”(Health facility 1 femaile-K1).
“…some people come here after they have gone to one traditionalist for healing as they are told that the disease is caused by spirits and needs to be targeted spiritually and some of them do not bring their children and only come back later when their condition has worsened…………..”(Health facility 5 femaile-K1).
3.7.11. Shortage of ARVs
Four respondents (13.8%) reported a shortage of ARVs and inefficacy of the ARVs the children were taking as the main reason the caregivers stopped coming to the health facility with their children and had to go elsewhere where their children could be helped.
This point was further strengthened by some pediatric healthcare staff in the treatment centers:
“stock availability has been an issue here from July till now. There is stock out of lopirito (lopinavir/ritonavir), which is one of the main drugs for children. We had to start rationing, and at one moment, it was just TLD, and we were giving for two weeks for children and adolescents who live closer and sometimes for a maximum of one month for those who live far, which is not easy on them considering the crises situation here, constant roadblocks and their distance. We have to ration so that children do not stay without medications until we outsource or get a regional supply….(Health facility 4 female-KI5).”
4. DISCUSSION
This study assessed the incidence, survival time, predictors of loss to follow-up from ART services and reasons for poor retention among children and adolescents in some ART treatment centers in Cameroon from the perspective of their service providers.
4.1. Incidence of Loss to Follow-up
The true cumulative incidence was 33 per 1000 child/adolescent years of LTFU over the study period, and the periodic prevalence was 13%. The incidence obtained from this study was not different from that obtained in Kenya [13], with 32.9 per 1000 child years of LTFU and a period prevalence of 12.6%. This magnitude of LTFU of 12.6% agreed with findings from previous studies conducted in sub-Saharan Africa cite (ref). About 21% of patients in HIV programmers were LTFU in Africa [1]. LTFU differed radically across populations because authors used different definitions. For instance, a Ugandan study reported 50.1% of children were LTFU [2], while a South African study reported an LTFU rate of 50.2% [3]. Different definitions of LTFU carry the inherent risk of misclassification of active patients as LTFU. Some studies cite the absence of 1 week from a scheduled appointment [4], and the absence of 2 weeks after an appointment date [5], while others use 6 weeks of missed appointment [6]. We employed the WHO [14-17] definition of LTFU as more than 90 days of absence from the missed clinical or drug pick-up appointment without any follow-up visit [7, 8], a definition also used by MINISANTE Cameroon. In Cameroon, previous studies have focused on HIV programs in conflict-free zones. Our study is among the very first looking at LTFU in the context of socio-political crises. In a study conducted in western Kenya, 14.2% of children were LTFU, and for children already initiated on ART, 14.1% dropped out of care [9]. This was, however, slightly greater than the 13% obtained from our study. It has been reported that 10-14% of children on ART get lost to follow-up in HIV care programs in Africa [9].
The cumulative survival probability at the end of the 10th month was 0.96 (95% CI: 0.95- 0.97), while it was 0.89 (95% CI: 0.88-0.92) and 0.87 (95% CI: 0.85- 0.89) at the 20th and 30th follow-up month, respectively. Our findings were similar to that obtained in Ethiopia, where the cumulative survival probability at the end of the 10th, 20th, 40th, and 60th follow-up month was 0.89 (95% CI:0.87,0.91), 0.82 (95% CI:0.79,0.85), 0.78 (95% CI:0.75,0.81), and 0.74 (95% CI:0.70,0.77), respectively.
4.2. Factors Predictive of Loss to Follow-up
Children and adolescents receiving care at HF1 and HF2, all located in rural and semi-rural settings, were more likely to be loss to follow-up compared to those in an urban setting (HF5). Our finding was similar to a systematic study reported from Asia-Pacific, Central, East, West, and Southern Africa, the Caribbean and Central and South America [14] where rural settings (as 1.21, 95% CI 1.13 to 1.29) risk LTFU. Another study showed no significant difference in the outcome of children in rural and urban settings [15].
Infants and young children were more likely to be LTFU compared to other age group categories. Our findings were similar to that obtained in South Africa [16]. A study in Zimbabwe [17] showed that those starting ART as young adolescents (10–14 years) had a 1.5 times higher rate of LTFU after moving into the 15–19 age group; adolescents starting ART aged 15–19 had an increased rate of LTFU compared to adolescents of the same age established on ART at an earlier age; and moving from adolescence into young adulthood increased the risk of LTFU by nearly twofold. Our findings were contrary to that obtained in India [18], where age ≥15 years (adjusted SHR (aSHR) 2.44; 95% CI:1.18 – 5.02) was a risk factor for LTFU.
Children and adolescents with non-biological caregivers had a greater risk of LTFU than those with biological parents as the main caregiver. Similar findings were obtained in Kenya [13]. Our findings were, however, contrary to that obtained in Ethiopia [19], where Children cared for by biological parents were nearly 2.8 at high risk of loss to follow-up as compared to children cared for by non-biological parents.
Children and adolescents on sub-optimal and other ART regimens had a greater risk of loss to follow-up compared with those on the optimal regimens. As of 2018, ART coverage among children was only 28% [5]. A systematic study in sub-Saharan Africa showed that more than half of all children on ART were still receiving suboptimal formulations. The use of suboptimal formulations negatively affects treatment adherence and viral suppression and ultimately increases HIV-related morbidity and mortality [5]. Sub-optimal and other ART combinations in children may result in lower efficacy, drug resistance, and subsequent poor retention.
The risk of loss to follow-up among ART-attending patients who did not have a primary caregiver was two times higher compared with their counterparts who had a primary caregiver (AHR: 2.59; 95% CI: 1.84, 3.66). This study’s finding was similar to the studies conducted in South Africa [16] and Ethiopia [20]. This might be due to family support, which means families may have the greater emotional support to offer than clinic staff. The child's primary caregiver was the parent (mostly mothers) in 59% of the cases, followed by relatives (aunties and uncles) 22%, and grandmother in 7% of cases. This means that a substantial number of the children and adolescents were under the care of grandmothers, relatives, and siblings who often have poor socioeconomic and low educational status contributing to loss to follow-up. No biological parents with poor socioeconomic status as main daily caregivers was identified as one of the challenges in the provision of HIV care in resource-limited settings [10].
Good history of adherence to ART for children and adolescents was a lower risk of LTFU compared with the history of poor or fair adherence on ART. Similar findings were found in Ethiopia [20], where children who had fair/poor adherence to ARV drugs were two and a half times more at risk of being LTFU than children who had good adherence. Our findings were contrary to that obtained in South Africa [21], where adherence was not a risk factor for loss to follow-up. Disruption in HIV care because of missed appointments can undermine clinical outcomes, including assessment of adverse events, ongoing provision of prophylactic medications, clinical and neurodevelopment assessment, and early identification of treatment failure results from LTFU.
Children and adolescents on ART above thirteen months had a lower risk of loss to follow-up compared with their counterparts on ART less than or equal to twelve months. Similar findings were obtained in South Africa [21], where most children and adolescents got lost within the first year of initiation to ART. Counseling on the importance of ART adherence should be done for caregivers whose children have been enrolled in ART within 1 year or less to prevent loss to follow-up.
Long distances had a higher risk of LTFU than children and adolescents with short distances of less than fifty kilometers. Our study was similar to that obtained in Zambia [22], where the long distance to health facilities was a risk factor for poor retention in patients on ART.
4.3. Reasons for Poor Retention as Derived from the Qualitative Study
Many healthcare providers complained of multiple caregivers for children and adolescents as the cause of LTFU in them. This was consistent with a study in Zambia [22], where the change of caregiver was a reason for LTFU in children on ART. Some studies have recorded inconsistent parental care [20] as a reason for LTFU. At the extreme, parental death had many implications on treatment outcomes [12, 21] in children, including LTFU in care if the children were on ART. The effects are widespread, including multiple separations of couples, movements to new households, educational challenges, and an increased risk for internalizing disorders and post-traumatic stress [4, 2]. Most often, due to this constant switching of caregivers, children find themselves in the hands of caregivers who are unaware that the children are on treatment. There is a need for health facilities to educate caregivers on the proper transitioning of children and for treatment centers to constantly update the demographic information for children and adolescents in case they have relocated to ensure continuity in care.
A serious socio-political crisis started in November 2016 in the Northwest and Southwest Regions of Cameroon, with over 4,000 people killed, 500,000 internally displaced and at least 40,000 externally displaced into neighboring Nigeria [23]. The armed conflict initially started as localized conflicts in certain districts in the NW and SW regions but quickly spread into a generalized armed conflict in both regions leading to disruption of movement, dysfunction of many health facilities, and numerous ghost towns [23]. This indeed led to a drop in health facility visits and retention in care for children and adolescents on lifelong ARVs, as observed from this study. Our findings were congruent with those of Marta et al. [24], who showed that sociopolitical crises in resource-limited settings lead to treatment interruptions and subsequent drug resistance among people with HIV/AIDS.
Adolescence is a stage of transition from childhood to adulthood, associated with specific challenges (including puberty) and vulnerability (such as early sexual debut, HIV, and STI acquisition) [25]. In addition, coping with the clinical and psychosocial impact of HIV imposes a substantial burden on this vulnerable group [25]. These developmental features may hinder an effective adherence to chronic medical therapies.
According to findings from the healthcare workers, some caregivers, due to stigma, do not come to the health facilities with their children nor tell family members of their health condition, which has contributed to poor retention in some children and adolescents. Our findings were consistent with previous findings in a systematic review in SSA [26], Malawi [27], Ethiopia [28], and Kenya [29]. A Qualitative study in Ethiopia [30] also demonstrated stigma as a cause for poor retention among adolescents. They described how they feared being seen by others while taking medication, visiting the clinic for appointments, and collecting ART medication as they were afraid of being stigmatized. Medication times and hospital appointments were not respected due to the fear of shame from friends and the risk of disclosing their status [30]. This highlights the need to intensify interventions to reduce HIV-related stigma and discrimination in all domestic and social circles.
Lack of timely disclosure at the appropriate age also emerged as a theme for poor retention in older children and adolescents. Our findings were in line with a qualitative study conducted among healthcare workers in South Africa [31], where they referred to the regrettable, negative outcomes of delaying disclosure to older children and adolescents that they had observed in their interaction with children and adolescents. When children are not informed of their status on time, this leads to treatment default as they continue to take medication without being informed about their HIV diagnosis. They become rebellious or refuse to take treatment or stop attending the clinic completely. Systematic review shows adherence to antiretroviral therapy (ART) improved post-disclosure in children in resource limited settings [32].
According to healthcare providers, some of the children come to the health facility, but since they do not know their HIV status or the reason why they are taking medications, they tend to shy away from care. The World Health Organization (WHO) also recommends that age-appropriate disclosure and caregivers’ regular support are essential to improve retention in ART care [1].
Lack of understanding of the disease process and treatment by caregivers was also reported as a reason for poor retention in care for children and adolescents. Similar findings were obtained in Malawi [27], where healthcare workers reported attrition as a result of HIV mothers themselves or their children feeling better, i.e., a lack of understanding of the treatment process. Our findings show the need for healthcare workers to constantly educate caregivers and adolescents on the disease process/treatment outcome and the importance of continuous and timely adherence to treatment.
Seeking alternative forms of healthcare with religious leaders and traditional healers was another reason for poor retention in children and adolescents. This decision to seek alternative care appeared to be influenced by religious teachings and traditional beliefs. This finding suggests the need for continued community sensitization about HIV and its treatment. Our findings aligned with those obtained in Malawi [27, 28], where seeking alternative healthcare was associated with LTFU.
In our study, the shortage of ARVs was cited by some key informants as a reason for poor retention in children and adolescents. At the peak of the sociopolitical crises, the hospital gave ARVs just for two weeks when the stock was limited to keep everyone on treatment. This discouraged many caregivers who lived in distant areas and had to pay the high cost of transportation for ARV refills just after two weeks. Similar findings associated with the shortage of commodities, including ARVs in Malawi [27], were reasons for poor retention. Sub-optimal regimens and other regimen combinations may lead to poor efficacy and retention. There is a need to devise emergency strategies to ensure that ARVs are constantly available for children and adolescents in conflict-affected areas. Moreover, for children and adolescents living in far distances and hard-to-reach areas, there is a need for a multi-month dispensation of ART.
CONCLUSION
Our study has shown a high incidence of LTFU in children and adolescents. Our study showed predictors of LTFU like health facility in a rural setting, younger age category, living with non-biological caregivers, short duration on ART, and long distance to health facility and different causes, such as multiple caregivers, long distances/cost of transportation, peer pressure, refusal, dating and marriage among adolescents, stigma, competitive life activities, lack of timely disclosure, poverty, lack of partner/family support, lack of understanding on the disease process and treatment, alternative forms of health care, and shortage of ARVs/poor efficacy, operating at different levels influencing LTFU in children and adolescents. This study has shown that multiple factors beyond health system factors contribute to loss-to-follow-up in resource-limited countries like Cameroon. This suggests that multi-faceted and timely interventions targeting a number of factors are needed to comprehensively address LTFU in children and adolescents.
STUDY LIMITATIONS AND PERSPECTIVES FOR FUTURE STUDIES
This study had several limitations. The sites were not randomly selected because we wanted to include a geographically diverse sample. We were limited to certain areas due to safety concerns. Furthermore, we limited the KIIs to HCWs and including the adolescents might provide further insights into the issues faced. There is a need for more studies to capture the magnitude of loss to follow up among children and adolescents in the non-conflict affected areas of Cameroon.
AUTHORS' CONTRIBUTIONS
PMT participated in the supervision of the research process, from the design and data collection to manuscript development, and read and corrected the manuscript for the scientific content. CWA participated in the design, data collection, qualitative data transcription, coding and interpretation, quantitative data analysis, drafting of the manuscript, correction and proofreading for the scientific content. PNA participated in manuscript writing, coding and classification of data and proofreading of the final manuscript for scientific content, and FNB participated in data collection, data analysis/interpretation and proofreading of the final manuscript for the scientific content. EMK participated in the study design, design of data collection instruments, supervision of data collection, validation of final data, manuscript writing and proofreading for scientific content. All authors read and approved the final copy of the manuscript.
LIST OF ABBREVIATIONS
| LTFU | = Loss to Follow up |
| HF | = Healthcare Facility |
| ART | = Anti-retroviral Therapy |
| HIV | = Human Immunodeficiency Virus |
| AIDS | = Acquired Immunodeficiency Syndrome |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical clearance was obtained from the Cameroon Baptist Convention Health Services Institutional Review Board (Ref number: IRB2021-42).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
The willingness of the study participants was asked using a written consent form and verbal consent. Participants were free to withdraw from the study if they felt so, with no effect on them.
STANDARDS OF REPORTING
COREQ guidelines were followed in this study.
AVAILABILITY OF DATA AND MATERIALS
Data available in CSV format upon request. Will need guidance in making our data set open in zenodo as well as in signing all the data sharing agreements?.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
We acknowledge and appreciate the staff at the various pediatric HIV treatment centers in the Northwest and Southwest Regions of Cameroon where the study was conducted who actively took part in the study. Their contributions have been essential to the global fight against HIV and AIDS in children and adolescents.

