All published articles of this journal are available on ScienceDirect.

Incidence Rate and Time to Occurrence of Renal Impairment and Chronic Kidney Disease among Thai HIV-infected Adults with Tenofovir Disoproxil Fumarate Use
Authors Info & Affiliations
Abstract
Background:
Tenofovir disoproxil fumarate (TDF) is a major antiretroviral therapy for Thai human immunodeficiency virus (HIV) infected adults. TDF is associated with a decrease in renal function. There is limited data about the use of TDF with the incidence and time to renal impairment and chronic kidney disease (CKD) in Thai HIV-infected adults.
Objectives:
To study the association of TDF with the incidence rate and duration of renal impairment and CKD in Thai patients.
Methods:
A retrospective cohort study in Thai naïve HIV-infected adults was conducted to compare the incidence rate and time to renal impairment and CKD in TDF and non-TDF groups. The incidence rate was analyzed by person-time. Time to renal impairment and CKD were analyzed by Kaplan-Meier curves and log-rank tests.
Results:
A total of 1,400 patients were enrolled. The incidence rates of renal impairment in TDF and non-TDF groups were 27.66/1,000 and 5.54/1,000 person-years. The rate ratio was 4.99 (95% confidence interval [CI] 2.66–9.35). The incidence rates of CKD in both groups were not significantly different. Themean difference of eGFR between the TDF and non-TDF groups was 1.92 ml/min/1.73 m2 (p = 0.022). Time to onset of renal impairment between the TDF and non-TDF groups was found to differ by approximately 20 months.
Conclusion:
The incidence rate of renal impairment was about five times higher in the TDF group. A rapid decline of eGFR occurred in the first 2–3 years of treatment. Therefore, the renal function of HIV-infected patients should be monitored so that the severity of renal impairment could be evaluated and CKD could be prevented.
1. INTRODUCTION
Human immunodeficiency virus (HIV) infection is a major public health problem. UNAIDS reported that there were about 38 million patients infected with HIV at the end of 2019 and there were about 690,000 patients who died from HIV-associated diseases. Additionally, 1.7 million patients with HIV are newly diagnosed each year, and 25.4 million patients receive antiretroviral therapy (ART) [1]. Currently, life expectancy in HIV-positive people is longer due to the effectiveness of ART. ART has improved significantly in recent years. The death rate from opportunistic infections has extremely decreased, but the death rate from non-infectious chronic disease among HIV-infected patients receiving ART has increased in the same way as patients without HIV, who mostly die from cardiovascular disease, liver disease, and renal disease [2].
In the U.S., there were patients with HIV (12.2%) who died from the renal disease between 1996 and 2006 [3]. In South Africa, patients with HIV who died from the renal disease increased to 67% between 1999 and 2006 [4]. Furthermore, the mortality rate from the renal disease has increased in patients with HIV in South America [5]. The result of a study reported that, after following HIV-infected patients who had an estimated glomerular filtration rate (eGFR) <60 ml/min/1.73 m2and in whom urine protein was detected for a period of 5 years, the death rate of this patient group was 48%, while the death rate in the group of patients without proteinuria dropped to 23%. In the HIV-infected patient group with eGFR > 60 ml/min/1.73 m2, no mortality was detected [6].
Since the HIV epidemic in the early 1980s and the first case of renal abnormality in 1984, many types of renal pathological abnormalities have been reported [7]. In the era prior to the use of ART, the causes of renal abnormality were associated with younger HIV-infected patients with high HIV viral loads [8-12], opportunistic infections [13-16], bloodstream infections [17, 18], HIV immune complex diseases [19-22], and HIV thrombotic microangiopathy [23, 24]. When HIV-infected patients are receiving ART, the cause of the renal abnormality is acute tubular necrosis in approximately 48% of the patients, with major stimulating factors, including drugs (pentamidine, aminoglycosides, trimethoprim-sulfamethoxazole, and non-steroidal anti-inflammatory drugs), ART, and dehydration that occurs in conjunction with the state of infection, low blood pressure, and respiratory failure [25, 26].
When renal impairment occurs and is not treated properly, it can lead to CKD.The incidence of renal impairment and CKD among HIV-infected patients was different from region to region and different amounts of proteinuria were detected [27, 28]. At present, with the use of ART, the incidence of renal impairment was 5.9/100 person-years [29].Also, the prevalence of CKD ranged from 7.2% to 32% [30, 31]. Nowadays, the cause of renal impairment and CKD in HIV-infected patients is attributed to ART [32, 33]. The data showed that patients who receive tenofovir disoproxil fumarate (TDF), one of the main antiretroviral drugs, increase their chances of having CKD by 1.56-fold compared to those receiving ART without TDF [34].
A few studies on HIV-infected patients with renal impairment and CKD have been conducted in Asia. TDF is recommended as one of the major drugs in the preferred antiretroviral regimen for the treatment of HIV-infected adults in Thailand and developing countries [35]. TDF is a cause of renal impairment and CKD. Moreover, no study on the incidence and time to event of renal impairment, and CKD in Thai HIV-infected adults has been conducted. Therefore, we aimed to study the association of TDF with the incidence rate and duration of renal impairment and CKD in Thai patients.
2. METHODS
2.1. Study Design and Population
A retrospective cohort study was conducted among HIV-infected Thai adults who attended the HIV Clinic at Police General Hospital, Bangkok, Thailand, between January 1, 2009, and December 31, 2015. Inclusion criteria were as follows: (1) attendance at the HIV Clinic at Police General Hospital, (2) naïve, (3) age ≥ 18 years old, and (4) baseline eGFR > 90 ml/min/1.73 m2. The exclusion criterion was a duration of follow-up < 1 year.
Baseline demographic and clinical characteristics, as well as follow-up laboratory data investigations, were retrieved and reviewed. The demographic data included gender, age, weight, height, body mass index (BMI), any underlying condition that may predispose to renal function decline (e.g., hypertension, diabetes mellitus, and hepatitis B and C virus co-infection), concurrent nephrotoxic drugs (e.g., angiotensin-converting enzyme [ACE]-inhibitors, angiotensin-receptor blockers [ARBs] and chronic or high-dose non-steroidal anti-inflammatory drugs [NSAIDs]). Baseline laboratory parameters at the time of initiation of ART were CD4 cell counts and serum creatinine. Follow-up parameters were HIV viral load, CD4 cell count, body weight and serum creatinine every 6 months after the initiation of ART. The eGFR was calculated using the simplified Levey modification of diet in renal disease (MDRD) formula [36]. Renal impairment and CKD, defined by eGFR < 60 ml/min/1.73 m2and eGFR < 60 ml/min/1.73 m2for at least 3 months, respectively. The study was reviewed and approved by the Institutional Review Board of Faculty of Medicine, Chulalongkorn University (IRB No. 309/59) and the Institutional Review Board of Police General Hospital (IRB No. 62/2559).
2.2. Sample Size Determination
The results from this study are binary outcomes that referred to the reference data from the literature about the past incidence of renal impairment [37]. The formula for a cohort study was used for calculating the sample size [38]. Using two population proportion (P1=0.09, 1-P =0.91), level of significance (α=0.05), power of the study (β=0.8) from a previous study [37], the sample size was summarized as 638 per group. However, we calculated an increase in sample size by 10% per group due to the drop-out rate. We subsequently studied 700 subjects per group.
2.3. Data Analysis
Demographic and clinical characteristics were compared between the TDF and control groups by using the Chi-square test and presented by using frequencies and percentages for categorical data and means and standard deviations (SDs) for continuous data with normal distribution. Fisher’s exact test was used to test the association between TDF use and renal impairment. The incidence rate was analyzed by person-time. The mixed-model method was used to determine the mean difference of eGFR between the TDF and non-TDF groups. Kaplan-Meier (KM) plots were used to visualize the association of duration of TDF use to renal impairment and CKD. Significance was calculated by the log-rank test, considered only if the p-value was <0.05 (95% confidence interval [CI]). Statistical analyses were performed using STATA/SE 15.0 software (StataCorp.2009.Stata Statistical Software: release 15.0, College Station, TX: StataCorp LP).
3. RESULTS
A total of 1,400 HIV-infected patients were included in the analysis. There were 432 (61.71%) males in the TDF group and 457 (65.29%) males in the non-TDF group. The mean age in the TDF group was 39.09 (± 9.20) years old and 39.32 (± 9.20) years old in the non-TDF group. The mean serum creatinine and eGFR before the initiation of ART were 0.75 (± 0.12) mg/dl and 112.73 (± 16.51) ml/min/1.73 m2 in the TDF group and 0.75 (± 0.11) mg/dl and 113.92 (± 12.57) ml/min/1.73 m2 in the non-TDF group, respectively. The mean CD4 cell count before the initiation of ART was 150.94 (± 70.97) cells/mm3 in the TDF group and 153.38 (± 70.18) cells/mm3 in the non-TDF group. The mean BMI before the initiation of ART was 22.37 (± 1.31) kg/m2 and 22.42 (± 0.93) kg/m2 in the TDF and non-TDF groups, respectively. There were 24 (3.43%) patients with hepatitis B virus co-infection in the TDF group. Baseline demographic and clinical characteristics of HIV-infected patients are presented in Table 1.
There were 52 and 12 patients with renal impairment in the TDF and non-TDF groups, respectively. The incidence rates of renal impairment in the TDF group were 27.66/1,000 person-years and 5.54/1,000 person-years in the non-TDF group after a 7-year follow-up period (Table 2). The rate ratio was 4.99 (95% CI 2.66–9.35, p < 0.001) (Table 3). Nine patients with CKD in the TDF group were observed, while five patients with CKD were determined in the non-TDF group. The incidence rates of CKD in the TDF group were 4.52/1,000 person-years and 2.29/1,000 person-years in the non-TDF group (Table 2). The rate ratio was 1.98 (95% CI 0.66–5.91, p = 0.220) (Table 3).
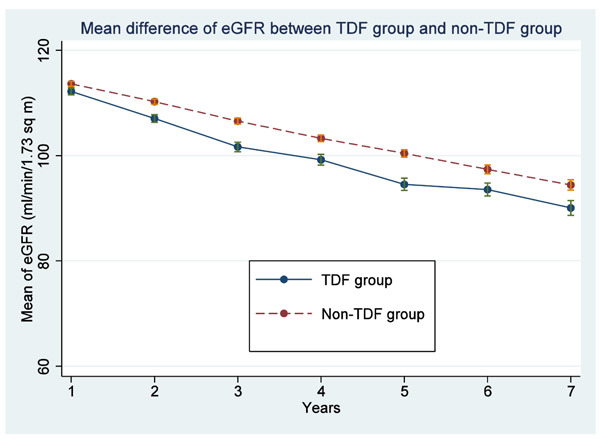
The mean eGRF in the TDF and non-TDF groups was 105.36 (± 52.85) ml/min/1.73 m2 and 107.27 (± 52.84) ml/min/1.73 m2, respectively, and was analyzed using a mixed-model method. The mean difference of the eGFR in both groups was 1.92 ml/min/1.73 m2 (95% CI 0.32–3.51, p = 0.022) (Fig. 1). The mean eGFR in both groups tended to decrease from the baseline, and the mean eGFR in the TDF group rapidly decreased in the first 2–3 years; then, the tendency of mean eGFR was quite steady.
|
TDF group (n =700) |
Non-TDF group (n =700) |
p-value | |
|
Gender Male (%) Female (%) |
432 (61.71) 268 (38.29) |
457 (65.29) 243 (34.71) |
0.16 |
|
Age (years old) Mean (±SD) |
39.09 (±9.20) | 39.32 (±9.20) | 0.63 |
|
Creatinine (mg/dl) Mean (±SD) |
0.75 (±0.12) | 0.75 (±0.11) | 0.42 |
|
eGFR (ml/min/1.73 m2) Mean (±SD) |
112.73 (±16.51) | 113.92 (±12.57) | 0.13 |
|
CD4 cell counts (cells/mm3) Mean (±SD) |
150.94 (±70.97) | 153.38 (±70.18) | 0.52 |
|
BMI (kg/m2) Mean (±SD) |
22.37 (±1.31) | 22.42 (±0.93) | 0.39 |
|
Co-infection Chronic hepatitis B (%) Chronic hepatitis C (%) |
24 (3.43) 8 (1.14) |
0 (0) 9 (1.29) |
<0.001 0.81 |
|
Underlying disease Hypertension (%) Diabetes mellitus (%) Dyslipidemia (%) |
44 (6.29) 20 (2.86) 222 (31.17) |
37 (5.29) 22 (3.14) 235 (33.57) |
0.42 0.75 0.46 |
|
ART (%) TDF + FTC/3TC + EFV TDF + FTC/3TC + NVP AZT + 3TC + EFV AZT + 3TC + NVP d4T + 3TC + EFV d4T + 3TC + NVP |
626 (89.43) 74 (10.57) 0 (0) 0 (0) 0 (0) 0 (0) |
0 (0) 0 (0) 508 (72.57) 85 (12.14) 51 (7.29) 56 (8.00) |
|
|
Concurrent nephrotoxic drug ACEI (%) ARB (%) NSAIDs (%) |
9 (1.29) 13 (1.86) 4 (0.57) |
10 (1.43) 11 (1.57) 6 (0.86) |
0.82 0.68 0.53 |
| Loss (%) | 58 (8.29) | 60 (8.57) | 0.85 |
| - | TDF group (/1,000 person-years) |
Non-TDF group (/1,000 person-years) |
| Renal impairment | 27.66 | 5.54 |
| Chronic kidney disease | 4.52 | 2.29 |
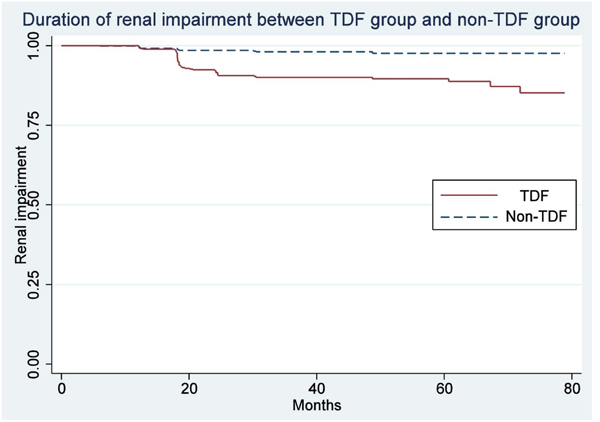
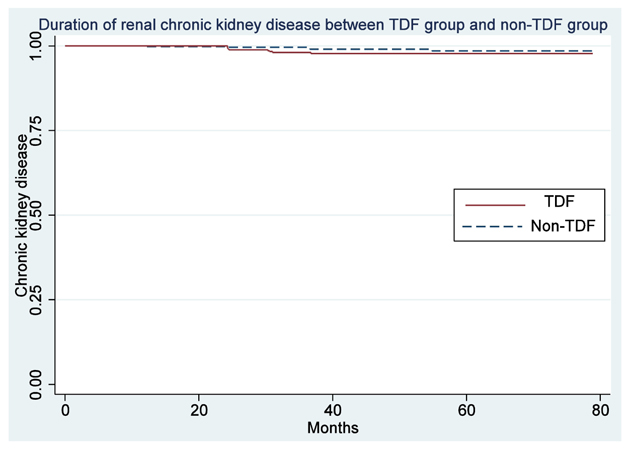
Data analyzed using the log-rank test showed that the duration of renal impairment in the TDF group and non-TDF groups differed by approximately 20 months. Statistically significant differences in renal impairment were found in the TDF and non-TDF groups (p < 0.001) (Fig. 2). There was no difference in the duration of CKD in the TDF and non-TDF groups, including no difference found after follow-up (p = 0.210) (Fig. 3).
| - | Rate ratio | 95% CI | p-value |
| Renal impairment | 4.99 | 2.66-9.35 | <0.001 |
| Chronic kidney disease | 1.98 | 0.66-5.91 | 0.220 |
4. DISCUSSION
This was the first study to investigate the incidence of renal impairment and CKD in Thai naïve HIV-infected patients. The study showed that the incidence of renal impairment in the TDF group was 27.66/1,000 person-years, which was around five times higher than that in the non-TDF group. The incidence of renal impairment in the TDF group was lower than the incidence in the previous study on Thai HIV-infected patients by Chaisiri et al., which found the incidence of renal impairment to be 16.20/100 person-years [39]. The possible cause may be that almost all the patients in the study by Chaisiri et al. received ART before receiving TDF, which is associated with a greater chance of renal impairment than in HIV-infected patients who have not received ART.
Additionally, the researcher used a different percentage of eGFR, which was a decrease in eGFR > 25% from the baseline eGFR to diagnose renal impairment. On the other hand, the current study used an eGFR < 60 ml/min/1.73 m2 to diagnose renal impairment. Using a decrease in eGFR > 25% from the baseline eGFRas a criterion for the diagnosis of renal impairment may result in a higher incidence of renal impairment than using an eGFR <60 ml/min/1.73 m2 as a criterion. Also, protease inhibitors (PIs) were used in the study, comprising approximately 30% of ART regimens. Multivariate logistic regression was analyzed in the previous study, and PIs were found to be a factor contributing to decreased renal function with an odds ratio (OR) of 2.12 (95% CI 1.15–3.92, p = 0.016). While in our study, we did not find HIV-infected patients receiving PIs in the first regimen. According to previous studies, approximately 60% of the patients weighed < 60 kg and had a median BMI of 19.60 (17.90–21.90) kg/m2. Analyzed by univariate and multivariate logistic regression, it was found that low body weight and low BMI resulted in decreased renal function, with an OR of 1.33 (95% CI 1.19–1.48, p <0.001) and 2.26 (95% CI 1.74–2.94, p <0.001), respectively [39].
In our study, the incidence of renal impairment was lower than the incidence of renal abnormality in the study by Tanuma et al., which occurred in a cohort of patients in Asia-Pacific countries, with an incidence of renal abnormality of 1.75/100 person-years [40]. Compared to the incidence of renal impairment from the study by Mocroft et al., which studied HIV-infected patients, 47% were Caucasian, 43% were of unknown race, and 8% were black. Moreover, the study was using the definition of renal impairment as an eGFR ≤ 70 ml/min/1.73 m2, which was different from our study. Also, 63% of the patients had previously received ART. This resulted in a higher incidence of renal impairment in our study (27.66/1,000 person-years)compared with that of the study by Mocroft et al. (4.78/1,000 person-years) [41]. Compared to the rapid decline of eGFR in the study by Scherzer et al., it was found that the rapid decline of eGFR was defined as a decrease of eGFR by 3 ml/min/1.73 m2 per year. The decline of eGFR was 93.20/1,000 person-years in the TDF group and 53.80/1,000 person-years in the non-TDF group, respectively [37].
Likewise, compared to the study by Ryom et al., the incidence rate of renal impairmentobserved in the TDF group, compared to the non-TDF group, was 1.18 (95% CI 1.12–1.25), which was lower than in our study [42]. In addition, there are no studies in Thailand showing the incidence rate of renal impairment in the TDF group compared to the non-TDF group.
The incidence of renal impairment varied from several studies.This is because there are different definitions of impaired renal function or decreased renal function, including the difference between populations used in the study.It was found that most of the patients had been previously exposed to ART, and the race of the population in other studies was different, which could make a difference in the results of the study.
The incidence of CKD in the TDF group was 4.52/1,000 person-years, which was not significantly different than in the non-TDF group. The rate ratio was 1.98. These data were similar to the data in the systematic review and meta-analysis by Islam et al. [34]. They found that the relative risk in the TDF usage group compared to the non-TDF usage group was 1.56 (95% CI 0.83–2.93). There is no data comparing groups with and without TDF usage in Asia, including Thailand and other countries.However, Pongpirul et al., who studied the incidence of renal diseases in HIV-infected patients receiving ART, determined that this incidence was lower than the previous incidence of CKD in Thailand. The incidence of CKD in Thai patients with HIV was found to be 10.39/1,000 person-years because the patients in the previous study received ART, and some of them had renal impairment before they started ART [43]. Compared with the results from the two studies, the incidence of CKD in the TDF was different in our study. Our study had a higher incidence of CKD in the TDF group as compared with that in the study by Mocroft et al., where the incidence of CKD was 1.33/1,000 person-years [41], while the study by Scherzer et al. showed an incidence of CKD of 18.70/1,000 person-years in the TDF group and 7.50/1,000 person-years in the non-TDF group [37].
Furthermore, studies in foreign countries and Thailand have not been found showing the rate ratio of CKD in the TDF group compared to that in the non-TDF group. The incidence of CKD in patients receiving TDF or another ART was different, and the differences were based on characteristics of the study population, such as race, age, baseline eGFR, hepatitis B and/or C virus co-infection, and underlying disease (including hypertension and diabetes mellitus). Compared to previous studies, the mean difference of eGFR in the TDF and non-TDF groups of our study was similar to that of the study by Cooper et al. The mean difference of eGFR in the TDF and non-TDF group was 3.92 (95% CI 2.13–5.70) ml/min/1.73 m2 [44], and it also had similar results to the study done by Martin et al., with a mean difference of eGFR of 2.70 ml/min/1.73 m2 [45].
From our study and previous studies, the results of the corresponding reduction in eGFR duration in patients with TDF usage showed a decrease in eGFR during the first 2–3 years after receiving TDF. Compared to a Thai study (Chaisiriet al.), it was found that the median time for a reduction of eGFR by 25% compared to the initial eGFR prior to the initiation of TDF was 28 months (95% CI 25.20–30.80) [39]. This result is close to the result of our study, although different definitions of renal impairment were used.
In our clinical practice, when patients have an eGFR < 60 ml/min/1.73 m2, we decrease the dose of ART depending on renal function, which may lead to a decreased incidence rate of CKD in this study following the recommendation of guidelines for antiretroviral therapy in HIV-1 infected adults and adolescents, the recommendations of the Thai AIDS Society (TAS) 2008 and Thai national guidelines for ART in HIV-1 infected adults and adolescents 2010 [46, 47]. There were no significant differences in the two groups, except a higher incidence of hepatitis Bvirus co-infection in the TDF group. Hepatitis B and C virus co-infection may lead to renal disease [48-52]. In our study, the patients who were detected as having hepatitis B virus co-infection received TDF along with emtricitabine or lamivudine as the recommendation of guidelines for antiretroviral therapy in HIV-1 infected adults and adolescents, the recommendations of the Thai AIDS Society (TAS) 2008 and Thai national guidelines for antiretroviral therapy in HIV-1 infected adults and adolescents 2010 in order to decrease the problem of hepatitis B virus resistance to lamivudine [46, 47].However, no patients with hepatitis B and C virus co-infection and renal abnormalities were found in our study.
Our study shows that the eGFR in the TDF group steadily declined. Therefore, the renal function of HIV-infected patients in Thailand should be closely followed in the first 2–3 years in order to evaluate the severity of renal impairment and prevent CKD in the future. One of the limitations of the study was its retrospective nature. Therefore, we could not examine some factors that affect renal impairment and CKD, such as some types of diet. Secondly, there was no urinary analysis. Thus, only eGFR was used to diagnose renal impairment and CKD. Finally, there was no HIV viral load result before starting ART because there were no guideline recommendations to test for HIV viral load before starting ART in Thailand [35, 46, 47, 53].
CONCLUSION
In this population, the incidence rate of renal impairment in the TDF group was around five times higher than that in the non-TDF group. The incidence rate of CKD was not different between both groups. After the initiation of TDF, eGFR rapidly declined in 2–3 years. Therefore, the renal function of HIV-infected patients with TDF usage should be carefully monitored so that the severity of renal impairment could be evaluated and CKD could be prevented in the future.
AUTHORS' CONTRIBUTIONS
JV, TR and NH were responsible for the conceptualization; JV and PP were responsible for the formal analysis; JV and NH acquired funding; JV, TR and NH were responsible for the investigation; JV, TR and NH were responsible for the methodology; JV was responsible for project administration; TR and NH were responsible for the supervision; JV and PP were responsible for writing the original draft; JV, TR, PP and NH were responsible for writing, reviewing and editing.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was reviewed and approved by the Institutional Review Board of Faculty of Medicine, Chulalongkorn University (IRB No. 309/59), and the Institutional Review Board of Police General Hospital (IRB No. 62/2559).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Not applicable.
STANDARDS OF REPORTING
STROBE guidelines and methodology were followed.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available from the corresponding author [J.V] upon reasonable request.
FUNDING
This study was supported by the 90th Anniversary of Chulalongkorn University Fund (Ratchadaphiseksomphot Endowment Fund), Chulalongkorn University (Grant No. GCUGR1125602004D).
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors would like to thank Assist. Prof. Chonnikant Visuthranukul, M.D. for her suggestions. We would like to thank the nurses of the HIV Clinic, Police General Hospital, for their enormous support.

