All published articles of this journal are available on ScienceDirect.

Determinants of the Discriminatory Behavior Experienced by People Living with HIV in Indonesia: A Cross-sectional Study of the Demographic Health Survey
Authors Info & Affiliations
Abstract
Introduction:
The discriminatory behavior experienced by People Living With HIV (PLWH) remains an unresolved problem in Indonesia. The aims of this research were to determine the factors associated with the discriminatory behavior experienced by PLWH in Indonesia.
Methods:
This study used cross-sectional design data by processing secondary data from the Indonesian Demographic Health Survey (IDHS) conducted in 2017. The total sample in this study was 15,413 records obtained via the two-stage stratified cluster sampling technique. The variables in this study were knowledge, information, socioeconomic and demographic details and the discriminatory behavior experienced by PLWH. The instrument refers to IDHS 2017. The data were analyzed using a chi-squared test and multinomial logistic regression.
Results:
The results obtained show that approximately 78.87% of respondents exhibited discriminatory behavior against PLWH in Indonesia. Respondents who had more knowledge about HIV [RRR: 25.35; CI: 2.85, 225.18] and who had earnings [RRR: 2.15; CI: 1.18, 3.92] were more at risk of discriminatory behavior than others. Respondents who lived in a rural area were less likely to engage in discriminatory behavior against PLWH than those who lived in urban areas [RRR: 0.51; CI: 0.29, 0.91].
Conclusion:
An increased understanding of HIV-AIDS and Indonesian people's acceptance of PLWH can occur through the provision of accurate information that is designed to prevent discriminatory behavior against PLWH. The government can consider this problem and further related policies so that PLWH can coexist in society and enjoy the same rights as those living without discrimination.
1. INTRODUCTION
HIV cases continue to be a significant global public health issue, and they have increased to approximately 33 million [1]. However, this situation has been accompanied by increasing discrimination against People Living With HIV (PLWH). Discrimination against PLWH is associated with the unfair treatment of individuals with a positive confirmed HIV status. This treatment can affect people around them, such as their family and close friends, and those who care for PLWH [2]. HIV-related discrimination can be experienced by people living with HIV and people who are related to, interact with and keep in touch with them. This discrimination includes poor social relations and other forms of pre-existing stigma [3, 4].
The National AIDS Commission, through the National Strategy and Action Plan for the Control of HIV and AIDS 2015-2019, adopted the UNAIDS strategy to achieve zero infections, zero deaths and zero discrimination in relation to PLWH [5]. In addition, the Indonesian government issued a policy through Minister of Health Regulation No. 21/2013 on combating HIV and AIDS discrimination against people with HIV by providing correct information about HIV and empowering PLWH [6]. This is in line with the UNAIDS targets for 90-90-90 by 2020, where 90% of PLWH know their status, 90% of PLWH receive antiretroviral therapy (ART) on a regular basis that is sustainable, and 90% of PLWH are undergoing treatment to suppress their viral load [7, 8].
An estimated 3.5 million people are living with HIV in the Southeast Asia region, which comprises 11 member countries, including Indonesia [9]. In Indonesia, the number of PLWH was 640.000 in 2018, with 46.000 people newly infected and 38.000 who died from an AIDS-related illness [10]. The HIV cases that are reported tend to increase every year, while the number of AIDS cases tends to be stable, with the highest number (10,315) occurring in 2016 [11]. The data and information available show that cases of HIV have spread to 407 of 507 districts/cities (80%) in all provinces [12]. The 3 provinces with the highest number of HIV cases are East Java, Jakarta and West Java, with 8.204 cases, 6.626 cases and 5.819 cases, respectively [13]. In 35% of countries with available data, over 50% of people report having engaged in discriminatory behaviors towards PLWH, including direct abuse and negative prejudice [14]. Recent research in Indonesia has shown that 78% of PLWH experience unpleasant actions that lead to discriminatory behavior from both their family and the community.
The effects of the stigma and discrimination from society experienced by PLWH are diverse and frequently encountered [4]. Discrimination does not only come from ordinary people. It can also come from the health care setting. Several reports have shown that health administration services in low-income and high-income nations have been known to provide low-quality care to patients with HIV [10]. In many countries, the general effect of an HIV-positive status can result in social exclusion, the loss or reduction of social support, and decreased opportunities for close relationships because of feelings of fear and discomfort with the discrimination that arises [15]. Other negative effects that are related to the health outcomes of PLWH are noncompliance with medication, anxiety and depression, lack of motivation and lower quality of life (Sweeney & Vanable, 2016; Turan et al., 2016; Turana, Fazelia, Raperb, Mugaverob, & Johnson, 2017; Kalichman, Katner, Banas, Hill, & Kalichman, 2020).
A previous study conducted in Indonesia evaluated the determinant factors of discriminatory behavior experienced by people who are HIV positive. The discriminatory variables included healthcare facilities, communities and families [20], healthcare workers, education, knowledge of the transmission and prevention of HIV, irrational fear of HIV transmission [21, 22], marital status and job status [24] and ethnicity [25]. A study on the discriminatory behavior experienced by PLWH based on knowledge, information, sex, age, wealth quintiles, education, residence and earnings has not been performed in Indonesia before. A study conducted by Harapan et al. (2013) focused on the discrimination faced by health care workers (HCWs). However, this study focused on the stigma faced by all individuals with HIV. Compared to the study by Situmeang, Syarif, & Mahkota, (2017), in this study, discriminatory behavior includes the family’s feeling of shame about a family member’s HIV status, not allowing children with HIV to attend school, hesitation about reactions from other people if the test is positive, people talking badly about people with HIV, and the fear of losing the respect of others. Furthermore, in this study, the sources for the information variables are internet, radio, newspapers/magazines, television, health professions, community meetings, seminars/counseling, and schools/teachers. This study aims to build an understanding of discriminatory behavior and to analyze the factors involved. Discriminatory behavior can prompt an attitude of unwillingness to continue treatment and/or therapy, and it can also increase the rate of mortality-related illness and decrease the quality of life.
2. MATERIALS AND METHODS
2.1. Study Design and Setting
This study used a cross-sectional design approach utilizing secondary data from the Indonesian Demographic Health Survey (IDHS) in December 2017. A cross-sectional design was used to determine the factors associated with the discriminatory behavior experienced by people living with HIV (PLWH) in Indonesia. The researcher obtained permission to use the survey dataset from Inner City Fund (ICF) International as part of the Demographic Health Survey program.
2.2. Participant and Sampling
The researcher combined the IDIR71FL dataset (Indonesian Individual Recode phase 7) and the IDMR71FL dataset (Indonesian Men Recode phase 7) to obtain the required female and male respondents. The data related to discriminatory behavior against PLWH are contained in both datasets. This study used data obtained from interviews with both men and women aged 15-54 years who had heard of HIV-AIDS. Those who had never heard of HIV/AIDS and any missing data were excluded from this study. The total population in this study was 59,636 respondents (male and female). The sample in this study was determined after being corrected by weight based on the number of provinces in Indonesia with the aim of obtaining the same data for each region in Indonesia. The total sample involved 15,413 respondents, with 3,566 males and 11,847 females. The sampling technique used two-stage stratified cluster sampling by selecting clusters from each stratum. A list of households was selected from each cluster. The selected households were then interviewed [26].
2.3. Study Measurements Tools
2.3.1. Discriminatory Behavior
The questions referring to discriminatory behavior against PLWH used in this study were as follows: “Would you want an HIV infection in the family to remain a secret?”, “Would you be ashamed if someone in the family had HIV?”, “Would you buy vegetables from vendors with HIV?”, “Should children with HIV be allowed to attend school with children without HIV?”, “Do people hesitate to take an HIV test because of the reaction from other people if it is positive?”, “Do people talk badly about people with or believed to have HIV?”, and “Do people with or believed to have HIV lose the respect of other people?” [26]. The Cronbach’s alpha value for the seven variables was 0.63. In this study, each variable was then re-coded with the statements “yes” and “no” to obtain the same statement related to discriminatory behavior. The response “don't know/not sure/depends” was excluded. All of the variables were compiled to obtain a new variable: discriminatory behavior. Discriminatory behavior was categorized into three groups: “no discrimination” if the responses were “no” for all variables, “some discrimination” if the respondent answered “yes” to 1-3 variables and “more discrimination” if the respondent answered “yes” to 4-7 variables.
2.3.2. Knowledge
The knowledge about HIV variable comprised several other variables that indicate the respondents' knowledge of HIV. These variables were “reducing risk of getting HIV: always using condoms during sex”, “reducing risk of getting HIV: having only 1 sex partner who has no other partners”, “one can get HIV from mosquito bites”, “one can get HIV by sharing food with people who have AIDS”, “a healthy-looking person can have HIV”, “HIV is transmitted during pregnancy”, “HIV is transmitted during delivery” and “HIV is transmitted by breastfeeding” [26]. The Cronbach’s alpha value for these variables was 0.80. Each variable was then re-coded with the statements “yes” and “no” to obtain the same statement related to HIV knowledge. The statement “don't know” was excluded. All of the variables were compiled to obtain a new “knowledge” variable. This variable was then divided into three categories: “no knowledge” if the respondent answered “no” for all variables, “some knowledge” if the respondent answered “yes” for 1-4 variables and “more knowledge” if the respondent answered “yes” for 5-8 variables.
2.3.3. Sources of Information
The sources of information about HIV comprised several other variables that indicate what the respondents had received in terms of information about HIV-AIDS. The variables related to the source for AIDS knowledge: internet, radio, newspapers/magazines, television, health professions, community meetings, seminars/counseling and school/teachers [26]. The Cronbach’s alpha value for these variables was 0.37. Each variable was re-coded with the statements “yes” and “no” to obtain the same statement regarding the source of information on HIV-AIDS. All of the variables were compiled to obtain a new “information” variable. This variable was then categorized into three groups, namely, “no information” if the respondent answered “no” for all the variables, “some information” if the respondent answered “yes” to 1-3 variables, and “more information” if the respondent answered “yes” to 4-7 variables.
2.3.4. Socioeconomic and Demographic Variables
The socioeconomic and demographic variables consisted of the sex variable: male or female. The age variable was categorized into four groups by age: 15-24 years old, 25-34 years old, 35-49 years old, and 50-54 years old [27]. The wealth quintile variable was determined based on a principal component analysis (PCA) [28] and categorized into richest, richer, middle, poorer, and poorest [29], [30]. The education variable was categorized based on Law Number 20 of 2003 concerning the National Education System in Indonesia [31]. The education category included higher education, secondary education, primary education, and no education. The residence variable was determined based on the Indonesian Population Census in 2010 [32], which was categorized into rural and urban. The employment variable was determined based on the employment status of the respondent and the respondents' earnings during the interview [26]. The employment variable was categorized as either “yes” or “no”. The respondents' earnings were categorized as “unpaid” if the respondent did not have an income. Meanwhile, the category “paid” indicated that the participant had an income in the form of cash only, cash and in-kind, or in-kind only.
2.4. Data Analysis
The data analysis conducted in this study used a chi-squared test for the bivariate analysis and multinomial logistic regression multivariate analysis. The researchers used the relative risk ratio (RRR) with a 95% confidence interval (CI) and a significance level of p<0.05. To conduct the analysis, the researchers used STATA version 16.1 software.
3. RESULTS
The results show that the majority of respondents, 78.87%, discriminated against PLWH. The majority of respondents (91.22%) knew about HIV%, and 85.4% had received information about HIV. Most of the respondents (46.86%) were aged 35-49 years, and the most predominant wealth quintile status was the richest category (29.55%). More than 50% of the respondents had a secondary education level, and more than 60% lived in an urban area. The majority of respondents worked and earned a living (Table 1).
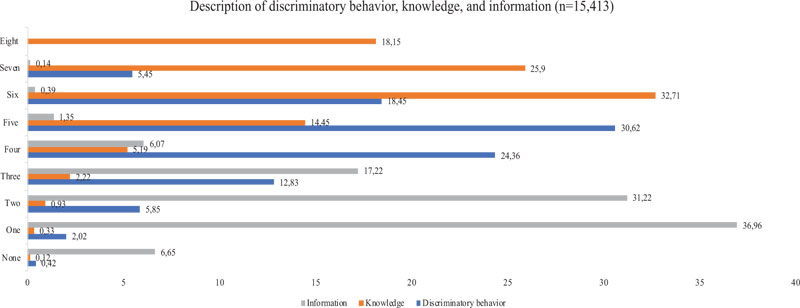
Fig. (1) shows the discriminatory behavior, knowledge, and information variables displayed by the respondent. From the figure above, one-third of the total respondents discriminated against PLWH according to five variables, and almost one-fourth of the total respondents discriminated against PLWH according to four variables. Only 2.02% discriminated against PLWH according to one variable, and 0.42% did not discriminate at all. More than one-third of the total respondents had knowledge about HIV according to six variables. One-fourth had knowledge of HIV related to seven variables. Meanwhile, only 0.12% of respondents did not know about HIV. According to the information sources, almost 40% of respondents obtained their information from only one variable. Meanwhile, 6.65% of respondents did not obtain any information about HIV.
Based on the bivariate analysis, almost all the variables had a relationship with the discriminatory behavior experienced by PLWH in Indonesia. However, no relationship was found for the currently working variable (Table 2).
| Characteristics | n | % |
|---|---|---|
| Discriminatory behavior No discrimination Some discrimination More discrimination |
65 3,191 12,157 |
0.42 20.70 78.87 |
| Knowledge No knowledge Some knowledge More knowledge |
18 1,336 14,059 |
0.12 8.67 91.22 |
| Information No information Some information More information |
1,025 13,162 1,226 |
6.65 85.40 7.95 |
| Sex Male Female |
3,566 11,847 |
23.14 76.86 |
| Age 50-54 35-49 25-34 15-24 |
427 7,223 4,860 2,903 |
2.77 46.86 31.53 18.83 |
| Wealth quintiles Poorest Poorer Middle Richer Richest |
1,865 2,370 2,981 3,643 4,554 |
12.10 15.38 19.34 23.64 29.55 |
| Education High education Secondary education Primary education No education |
4,539 8,541 2,285 48 |
29.45 55.41 14.83 0.31 |
| Residence Urban Rural |
9,747 5,666 |
63.24 36.76 |
| Currently working No Yes |
1,211 14,202 |
7.86 92.14 |
| Respondents’ earnings Unpaid Paid |
1,979 13,434 |
12.84 87.16 |
| Variables | Discriminatory Behavior | X2 | |||||
|---|---|---|---|---|---|---|---|
| No | Some | More | |||||
| n | % | n | % | n | % | ||
| Knowledge No knowledge Some knowledge More knowledge |
1 10 54 |
0.01 0.06 0.35 |
11 350 2,830 |
0.07 2.27 18.36 |
6 976 11,175 |
0.04 6.33 72.50 |
62.15*** |
| Information No information Some information More information |
7 52 6 |
0.05 0.34 0.04 |
258 2,737 196 |
1.67 17.76 1.27 |
760 10,373 1,024 |
4.93 67.30 6.64 |
31.39*** |
| Sex Male Female |
17 48 |
0.11 0.31 |
844 2,347 |
5.48 15.23 |
2,705 9,452 |
17.55 61.32 |
25.39*** |
| Age 50-54 35-49 25-34 15-24 |
2 29 22 12 |
0.01 0.19 0.14 0.08 |
121 1,594 883 593 |
0.79 10.34 5.73 3.85 |
304 5,600 3,955 2,298 |
1.97 36.33 25.66 14.91 |
42.65*** |
| Wealth quintiles Poorest Poorer Middle Richer Richest |
15 13 9 12 16 |
0.10 0.08 0.06 0.08 0.10 |
514 518 653 718 788 |
3.33 3.36 4.24 4.66 5.11 |
1,336 1,839 2,319 2,913 3,750 |
8.67 11.93 15.05 18.90 24.33 |
103.61*** |
| Education High education Secondary education Primary education No education |
17 30 17 1 |
0.11 0.19 0.11 0.01 |
780 1,842 550 19 |
5.06 11.95 3.57 0.12 |
3,742 6,669 1,718 28 |
24.28 43.27 11.15 0.18 |
75.52*** |
| Residence Urban Rural |
28 37 |
0.18 0.24 |
1,787 1,404 |
11.59 9.11 |
7,932 4,225 |
51.46 27.41 |
104.34*** |
| Currently working No Yes |
2 63 |
0.01 0.41 |
276 2,915 |
1.79 18.91 |
933 11,224 |
6.05 72.82 |
5.37* |
| Respondents’ earnings Unpaid Paid |
17 48 |
0.11 0.31 |
491 2,700 |
3.19 17.52 |
1,471 10,686 |
9.54 69.33 |
34.74*** |
Table 3 shows the results of the multivariate analysis using a multinomial logistic regression with a 95% CI. In this analysis, we used knowledge, information, socioeconomic details and demographic characteristics to predict discriminatory behavior against PLWH with the category “no discrimination” as a baseline outcome. From the analysis, knowledge, residence and earning responsiveness were found to be associated with the risk of engaging in “more discriminatory behavior” against PLWH. Respondents with more knowledge were 23.35 times more likely to be at risk of expressing more discriminatory behavior than “some discriminatory behavior” and “no discriminatory behavior” compared with those with no knowledge [RRR: 25.35; CI: 2.85, 225.18]. The respondents from rural areas were 0.51 times less likely to be at risk of expressing more discriminatory behavior than some discriminatory behavior and no discriminatory behavior compared with the respondents who lived in an urban area [RRR: 0.51; CI: 0.29, 0.91]. Meanwhile, respondents with paid work were 2.15 times more likely to be at risk of displaying more discriminatory behavior than some discriminatory behavior and no discriminatory behavior compared with the respondents who had no earnings [RRR: 2.15; CI: 1.18, 3.92]. Other variables, such as information, sex, age, wealth quintile and education, had no risk related to discriminatory behavior targeting PLWH in Indonesia.
4. DISCUSSION
Most of the respondents who had more knowledge about HIV had a greater chance of engaging in discriminatory behavior than people who did not have knowledge. Discrimination happens because of the many misconceptions about the way HIV is transmitted, such as through mosquito bites and using shared cutlery [33], even though that knowledge is false. People who have more knowledge about HIV/AIDS will fear and discriminate against PLHIV [34-36]. Thus, many people have negative views about PLHIV [37] because people believe that PLHIV can transmit HIV/AIDS to others [35, 38]. People do not accept the risk, so they prefer to stay away from rather than live with PLHIV [38].
| Variables | Some Discriminatory Behavior | More Discriminatory Behavior | ||
|---|---|---|---|---|
| RRR | 95% CI | RRR | 95% CI | |
| Knowledge | ||||
| No knowledge | 1.00 | 1.00 | ||
| Some knowledge | 2.96 | [0.33, 26.18] | 12.91** | [1.35,122.88] |
| More knowledge | 4.26 | [0.51, 35.02] | 25.35*** | [2.85,225.18] |
| Information | ||||
| No information | 1.00 | 1.00 | ||
| Some information | 1.09 | [0.47,2.53] | 1.19 | [0.52,2.75] |
| More information | 0.65 | [0.19,2.16] | 0.87 | [0.26,2.85] |
| Sex | [0.61,2.12] | [0.72,2.46] | ||
| Male | 1.00 | 1.00 | ||
| Female | 1.14 | 1.33 | ||
| Age | ||||
| 50-54 | 1.00 | 1.00 | ||
| 35-49 | 0.83 | [0.18,3.78] | 1.05 | [0.23,4.74] |
| 25-34 | 0.57 | [0.12,2.69] | 0.91 | [0.19,4.22] |
| 15-24 | 0.66 | [0.13,3.43] | 0.89 | [0.17,4.58] |
| Wealth quintiles | ||||
| Poorest | 1.00 | 1.00 | ||
| Poorer | 0.89 | [0.41,1.94] | 1.11 | [0.51,2.40] |
| Middle | 1.42 | [0.59,3.44] | 1.67 | [0.69,4.01] |
| Richer | 1.05 | [0.44,2.49] | 1.32 | [0.56,3.10] |
| Richest | 0.82 | [0.33,2.01] | 1.11 | [0.46,2.72] |
| Education | ||||
| High education | 1.00 | 1.00 | ||
| Secondary education | 1.28 | [0.66,2.47] | 1.12 | [0.58,2.15] |
| Primary education | 0.7 | [0.30,1.59] | 0.62 | [0.27,1.42] |
| No education | 0.46 | [0.05,4.06] | 0.22 | [0.02,1.92] |
| Residence | [0.38,1.20] | [0.29,0.91] | ||
| Urban | 1.00 | 1.00 | ||
| Rural | 0.67 | 0.51** | ||
| Respondents’ earnings | [0.99,3.33] | [1.18, 3.92] | ||
| Unpaid | 1.00 | 1.00 | ||
| Paid | 1.81* | 2.15** | ||
Therefore, it is necessary to build accurate knowledge to reduce the stigma associated with PLHIV. Accurate knowledge can be disseminated through government programs and health education with a more comprehensive and open approach. It is hoped that the knowledge received by the community regarding PLHIV is direct and precise and can reduce discriminatory behavior.
Accurate information will not cause discriminatory behavior towards PLHIV. This is consistent with a study conducted in Nigeria by Simpson in which PLHIV, who participated in group activities in the community did not experience discrimination and were accepted well [39, 40]. Individuals who have more information will not be worried about PLHIV. Good information in schools about HIV prevention and transmission also helps the community properly understand HIV/AIDS [41]. Providing information using media, including advertising campaigns and entertainment designed to educate as well as amuse (“edutainment”) and the integration of nonstigmatizing messages into TV and radio [42] can also have a positive impact. When many people have accurate information about HIV, there will be no discrimination against PLHIV.
Sex and age were not linked with discriminatory behavior against PLHIV. In Indonesia, parents teach tolerance to children [43]. Everyone also understands how to respect others, regardless of their age or gender. Adults are understanding, tolerant, mature, open, forgiving, and nonjudgmental [44]. Adults understand that humans are not always right and do not deserve to be discriminated against due to their mistakes or because they have a disease such as HIV infection; it is also understood that these individuals should receive social support [45]. Studies in China have also shown that PLHIV must obtain social support from humans in general to have a good quality of life [46]. Discrimination has a negative impact on PLHIV. They need to receive support and care to improve their quality of life. Solidarity, accurate information, and an understanding of tolerance from childhood to adulthood are necessary to prevent discrimination.
Wealth quintiles were not correlated with discriminatory behavior against PLHIV. People who have high or low economic status did not discriminate. Members of Indonesian society uphold the values of humanity. They respect each other and do not want to hurt others [47]. Their religious and cultural values do not let them hurt or harm others because of stigma, and this is consistent with research conducted in Ghana that found that negative stigma is contrary to the teachings of that society [48]. People with HIV/AIDS are human beings who have human rights protections, guaranteed health services from the government, and access to proper healthcare, and they have the right to work and live their lives [48]. People in the high and low wealth quintiles should not discriminate against PLHIV.
The results of the study indicate that level of education is unlikely be a factor in discrimination against PLWH. These results are in line with research conducted by Jacobi et al. (2020) at the Secondary School, Government High School, Bokwango, and the Government Bilingual Grammar School, Molyko, Africa. Students are taught by from HIV-positive teachers have more knowledge about and understand appropriate behavior to prevent stigma against PLWH [49]. Another study conducted by Maughan-Brown and Spaull (2014) showed that among students in grade six, those who received information about HIV had a better understanding of and avoided misconceptions about HIV transmission. Therefore, they were less likely to engage in discriminatory behaviors [50].
Respondents at all four levels of education in this study, including those with no education, were not likely to engage discriminatory behavior. People with certain education levels may not engage in discriminatory behavior because they already understand how the disease is transmitted and realize that people with HIV need support for treatment [37, 51]. At each stage of education, teachers and other sources can provide information about HIV/AIDS to students who have little knowledge about it. People with no education are also less likely to discriminate because the information they obtain is limited, and they do not have sufficient knowledge regarding the transmission of this disease. Therefore, people with no education consider people with HIV to be the same as healthy people in general.
Residence is correlated with discriminatory behavior. Those who live in rural areas are more likely to engage in discriminatory behavior directed against PLWH than those who live in urban areas. These results are consistent with research conducted in India, which found that there are more barriers, such as less information on safe sexual behaviors, to combating HIV in rural areas [52]. A study in China found that PLHW in rural central China suffer from the burden of HIV-related stigma at a moderate to high level [53]. A study in India found that PLWH who live in rural areas are more likely to experience more stigma and discriminatory behavior due to the low family support and social support in these areas [36]. Research in Alaska and New Mexico conducted by Brems (2010) showed that stigma in small urban areas is significantly lower than that in other types of communities [54].
In this study, respondents in rural areas were more likely to engage in discriminatory behavior. In the Indonesian context, this is influenced by beliefs about society and culture. Individuals in rural societies believe that PLWH deserve punishment and should be given a negative label because of their sins [3]. Rural society often associates PLWH with risky behavior, such as free sex (especially among homosexual individuals) and drugs, even though housewives who are loyal to their husbands, and even innocent babies, can be infected with HIV. Therefore, the community usually has no sympathy for PLWHA. However, PLWHA may die if they do not receive optimal care. Consequently, the government must be aware of this issue and provide services and spaces that are accessible to everyone, especially PLWH, where all people without exception can experience the same security, comfort and protection and PLWHA do not experience stigma and discrimination from society.
The respondents’ earnings were also correlated with discriminatory behavior. Individuals who were paid or had an income were more likely to engage in discriminatory behavior. This finding is similar to those of previous studies by Amaral (2013) on the experience of stigma and discrimination and the implications for healthcare-seeking behavior among PLWH [55]. People who have earnings can access higher education and seek information about HIV. Thus, they feel as if they know more and tend to underestimate others who earn low pay. This statement supports the study by Kebaso (2016), which found that people with a low level of education who had low pay tended to experience stigma and discrimination [56]. Discriminatory behavior was more likely to be experienced by the paid respondents with a low income than by the other paid respondents. This finding is related to their ability to afford their expenses. They are less likely to have negative opinions of themselves [57]. Another study mentioned the same problem: PLWH with a lower economic status experience food insecurity and limited or no access to nutritional food in their daily life [58]. Low pay leads to inequitable access to health and other social services, making individuals who have low earnings an easy target for discrimination. In addition, people may have a high level of knowledge, but it is not necessarily good knowledge that includes an accurate understanding of HIV. A great deal of understanding is required concerning the problems faced by people with HIV. In this case, the role of government and health workers is very important in providing good and accurate information to the whole community using various methods and media platforms.
CONCLUSION
People's knowledge, earnings and residence are the factors that are correlated with the discrimination experienced by PLWH in Indonesia. The level of knowledge about HIV is directly proportional to the display of discriminatory behavior because low levels of knowledge are associated with negative views and misconceptions. Building a body of accurate knowledge makes it possible to reduce the level of discriminatory behavior. With regard to earning, stigma and discrimination are often exhibited by those with a high income, and this finding is related to the ease of obtaining information. Meanwhile, people living in villages are less likely to discriminate, and they tend to accept PLWH because they adhere to the principles of togetherness and sociality. Based on the results of this study, the government can consider and develop further policies to reduce the discriminatory behavior experienced by PLWH. These individuals should be able to live and have their rights respected like other people. Information about HIV should be provided.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
We use secondary data from Indonesian Demographic Health Survey. Thus, ethics approval granted by the Ministry of Health of Indonesia. Permission to use the dataset was obtained from ICF International, Indonesia with number 145686 as part of the Demographic Health Survey program.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION.
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
The authors confirm that the data supporting the findings of this study are available within the article.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflicts of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

