All published articles of this journal are available on ScienceDirect.

Examining HIV and STIs Related Knowledge Among Male Adolescents in Saudi Arabia
Abstract
Background:
Sexually Transmitted Infection (STI) is a major global cause of acute illness, long-term disability and death, with serious medical and psychological consequences. Knowledge and awareness about the transmission of sexual disease play an important role in the prevention of the disease. Very little is known about HIV and STI in adolescents and associated factors in Saudi Arabia.
Objective:
The aim of this study was to examine the association between self-rated STI knowledge and HIV and STI knowledge test scores, as well as to investigate the association between adolescents’ HIV and STI knowledge and their demographic background and sexually related behaviors.
Methods:
A multi-stage cross-sectional study was conducted using a self-administered questionnaire, recruiting 453 male adolescents (15 and 20 years) from private and public male high schools in Riyadh, the capital city of Saudi Arabia.
Results:
More than half (53.4%) of the adolescents reported their STI knowledge as excellent or good (42%). However, based on the total score scale of HIV and STI knowledge, 64.3% had a poor level of knowledge. The sexual information sources commonly cited were friends (70%) and internet (40.0%); and the least cited sources were fathers (16%) and mothers (15%). The logistic regression analysis revealed that adolescents’ father and mother education (>12 years) were positively associated with adolescent’s HIV and STI knowledge level (OR= 1.6, 95% CI: 1.1-2.4, p= 0.040) and (OR= 1.8, 95% CI: 1.2-2.8, p= 0.010). No significant association was found between adolescents’ HIV and STI knowledge and their sexual behaviors and attitudes.
Conclusion:
Findings suggest that a high proportion of male adolescents have poor HIV and STI related knowledge. Poor knowledge and reliance on potentially unreliable informational sources coupled with an over-estimate perception of STI expertise suggests that improvements in STI and HIV education should be addressed. Additional research is needed to help identify factors (beyond knowledge) associated with sexual behavior and attitudes that may increase the risk for STIs and HIV among adolescents.
1. INTRODUCTION
Adolescence is generally considered to begin with the onset of puberty. Adolescence is a period when remarkable changes and challenges are experienced in many aspects, physically, socially, psychologically, as well as sexual development. Consequently, during this period, adolescents may engage in risk behaviors that put their health and lives in danger. Many diseases in adulthood, which can lead to serious illness or premature death [1], have their roots in adolescence, including risky behaviors related to Sexually Transmitted Infections (STIs). Moreover, sex at a young age may influence sexual risk behaviors that place adolescents at increased risk for unintended pregnancy and Sexually Transmitted Infections/Diseases (STIs/STDs), including the Human Immunodeficiency Virus (HIV) [2]. Although the social, psychological and health-risks of adolescent sexual behaviors are well known, adolescent’s sexual health-related issues are largely neglected in many countries, including Saudi Arabia.
Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS) which are spread through various sexual contacts and activities are recognized as major public health issues worldwide. Currently, over 30% of all new HIV infections globally are estimated to occur among youth ages 15 to 25 years [3]. Moreover, every day, thousands of young people are infected with HIV across the globe, which results in nearly two million new infections per year [4]. Young people’s risk of becoming infected with HIV is closely related to the age of sexual debut [3]. Data from Youth Risk Behavior Surveillance among high school adolescents reported that 39.5% previously had sexual intercourse [5]. Unfortunately, no comparable data is available in Saudi Arabia, however, a study investigating sexual behaviors among adolescents in Saudi Arabia found that 38% had experienced some type of sexual contact [6].
Although treatment is available for most STIs, prevention is preferable since they can have serious, long-term health and social implications. Many adolescents are at risk of acquiring STIs, and they are much more susceptible to spreading them when there is a lack of accurate health information and reproductive health services [7]. Improving knowledge related to STIs prevention is an important aim of sexual and reproductive health education and is crucial for healthy sexual behaviors. Findings from a review study suggest that sexual health education is effective in increasing sexual knowledge [8], which in turn can promote positive attitudes and healthy sexual behaviors. Effective sexual education is also a vital part of HIV prevention [9]. Effective sexual education can “provide young people with age-appropriate, culturally relevant and scientifically accurate information” [10]. Besides sexual health education may help reduce the risks of negative outcomes from sexual behaviors. Yet, the association between sexual knowledge and sexual behavior is unreliable and uncertain. A review by the Cochrane Collaboration on adolescents’ sexually-related health concluded that most interventions appeared to have a positive effect on knowledge and attitudes, though the effect on behavior was less consistent [11].
Although, there is growing recognition of the importance of addressing the sexual and reproductive health of adolescents [12], open discussion of sexual and sexuality issues can be difficult in several countries and among diverse cultures for many reasons. In Saudi society, discussing sexual health-related matters, particularly among adolescents, is considered a taboo. Moreover, sex education is highly controversial issue in Saudi Arabia and other Gulf Cooperation Council Countries (Kuwait, Bahrain, Qatar, Oman, and the United Arab Emirates). Adolescents in Saudi Arabia face massive challenges due to increasing globalization, urbanization, and other external forces including digital communication that might play a vital role in their sexual health knowledge and behaviors. Nowadays, media are significant providers of sexual information and knowledge [13, 14], often promoting the idea that being sexually active makes a person mature and attractive, which in turn can lead to the development of potentially damaging attitudes and beliefs [15].
Unfortunately, studies addressing sexual health-related issues are extremely lacking. This study can promote the need for the development of policies and practices by the policy makers and local communities for effective sexual health intervention including sexual education.
2. METHODS
2.1. Subjects and Ethical Clearance
This study involved male adolescents, aged between 15 and 20 years, attending their 10th, 11th and 12th high school years in Riyadh City, Saudi Arabia. A multi-stage stratified sampling procedure was applied to select the students from private and public schools (4 schools in total), and from different class levels to yield a representative sample of male high school students in Riyadh. In total, a sample of 453 students was randomly included in this study. Ethical approval was obtained from the Ministry of Education, Ethical Review Committee, Riyadh Region. To ensure their consent; the researcher indicated to adolescents that their participation in the study was totally voluntary and that they could refuse to take part in the study. All information was collected and analyzed anonymously, and the results would be used only for research purposes.
2.2. Survey Measures
The survey instrument was derived from instruments used in many studies assessing sexual health-related issues among youth worldwide: Youth Risk Behaviors Surveillance (YRBS) from the U.S. Centers for Disease Control and Prevention [16] and the Global School-based Student Health Survey (GSHS) by the World Health Organization [17]. The questionnaire was first piloted, and a pretest was conducted among small groups of high school students to ensure its validity; more details of the methodology are available elsewhere [6, 18].
Adolescents were asked to rate their perception of their STIs knowledge. Moreover, six items were used to assess their basic knowledge of HIV and STIs as follows: 1. “AIDS is a fatal disease”; 2. “STIs/STDs spread through several sexual practices”; 3. “A person can have an STI/STD and not experience symptoms”; 4. “HIV can be transmitted during the first contact with an infected person”; 5. “Condom should be used one time only”; and 6. “A condom can protect against STIs/STDs.” Items were assessed with three response options (“No”; “I do not know”; “Yes”). “No” and “I do not know” responses were valued as “zero point”, and responses with “Yes” were considered as right answers and were given “one point”. Subsequently, final scores ranged from 0 to 6, with high scores suggesting good knowledge. Then, for further analysis, the scale was categorized according to whether they had a “good level of sexual knowledge” (score of 5-6) or a “poor level of sexual knowledge” (score ≤ 4). Moreover, the students’ background characteristics including age, school grade, type of school and parental education level, and their sexual-related behaviors were collected.
2.3. Data Analysis
Data completeness and accuracy were assured by double-checking records upon data entry completion. The data was coded, entered, cleaned, and analyzed using the SPSS Version 22.0 statistical software (Armonk, NY: IBM Corp.). First, descriptive statistics were conducted to provide profiles of the participants, their HIV and STI related knowledge, and their sources of information. Second, ANOVA and cross-tabulation statistical analyses were performed investigating the relationship between self-rated STI knowledge and HIV and STI test summary scores. Third, two binary regression analyses were performed to investigate the associations among adolescents’ HIV and STI related knowledge and their socio-demographic variables, and sexual behaviors and attitudes. Good HIV and STI knowledge served as the dependent variable(s). Both Odds Ratio (OR) and its 95% Confidence Level Interval (CI) were provided, and an alpha level of less than 0.05 was set as statistically significant.
3. RESULTS
As presented in Table 1, the mean as well as the median participant age was 17 years with a Standard Deviation (SD) of +/-1.33. Less than half of participants (40.8%) were younger than 17 years of age.
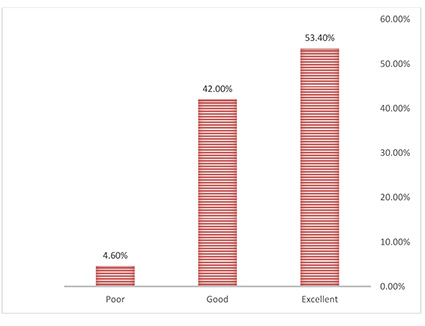
A total of 242 adolescents (53.4%) described their level of STI related knowledge as excellent, 190 (42%) described it as good, and 18 (4%) described themselves as having a poor level of STI knowledge (Fig. 1).
Of the 453 adolescents, 422 (93.2%) correctly stated that HIV/AIDS is a fatal disease (Table 2). The majority (79.7%) knew that HIV/AIDS can be acquired by first sexual intercourse with an infected person. Also, 53.9% of them knew that HIV/AIDS can spread through several types of sexual practices other than penetrative sex. Also 53.6% agreed that a person can have HIV/AIDS and not experience symptoms. Slightly more than half (52.8%) knew that condoms could be only used one time, and 46.6% knew that condoms are a method of preventing STI transmission.
Table 3 shows the respondents' index of the HIV/AIDS related knowledge. It showed that a low percentage of adolescents (11%) correctly responded to all the six items.
One-way ANOVA analysis (Table 4) revealed no differences between the students' mean scores of HIV/AIDS related knowledge and their self-reported level of sexual knowledge (F = 2.247, P = 0.107), indicating that the majority incorrectly self-assessed their level of STI related knowledge.
| Variable | No. | % |
|---|---|---|
| Age (grouped) 15-16 17-18 19-20 Total |
185 203 65 453 |
40.8 44.8 14.3 100 |
| Father’s educational level ≤12 years >12 years Total |
216 235 451 |
47.9 52.1 100 |
| Mother’s educational level ≤12 years >12 years Total |
323 130 453 |
71.3 28.7 100 |
| Type of schools Public schools Private Schools Total |
270 183 453 |
60 40 100 |
| Statements | Yes |
|---|---|
| No. % | |
| HIV/AIDS is a fatal disease | 422 93.2 |
| HIV can be transmitted by first sexual contact with an infected person | 361 79.7 |
| HIV can be transmitted through several sexual practices | 244 53.9 |
| A person can have HIV and not experience symptoms | 243 53.6 |
| Condoms should be used one time only | 239 52.8 |
| A condom can protect against STIs | 211 46.6 |
| Scores | Number of Students | Percentages (%) |
|---|---|---|
| 0 | 10 | 2.2 |
| 1 | 22 | 4.9 |
| 2 | 50 | 11.0 |
| 3 | 97 | 21.5 |
| 4 | 113 | 24.5 |
| 5 6 |
111 50 |
24.4 11.0 |
| Total | 453 | 100 |
| Perceived Sexual Knowledge | N | Mean score | Std. Deviation |
|---|---|---|---|
| Excellent | 242 | 3.9 | 1.41 |
| Good | 190 | 3.7 | 1.48 |
| Poor | 18 | 3.4 | 1.41 |
Table 5 shows that more than half (64.3%) of the adolescents in this study had poor sexual knowledge. Among those who reported their level of knowledge as excellent and good, 62.4% and 65.8% respectively were observed to have poor knowledge.
Fig. (2) displays the reported resources for sexual information among surveyed students. The most commonly reported resource was friends (69.8%). Other important resources among adolescents were internet (40.2%), school and teachers (39%), religious men (32.5%), hospitals and health services (30.5%), and siblings (26.7%). Parents were the lowest reported sexual information source.
Table 6 represents the relationship between adolescents’ level of STI related knowledge and their socio-demographics. Among adolescents’ socio-demographic variables, only adolescents’ age was positively associated with having a good level of sexual knowledge. Compared with younger adolescents (15-16 years), adolescents of age 17-18 years were two times more likely to have good knowledge (OR= 2.3, 95% CI: 1.1-4.5, p = 0.020), and those aged 19-20 years were three times more likely to have good knowledge (OR = 3.1, 95% CI: 1.3-7.30, p = 0.011).
As shown in Table 7, no significant association was found between having good sexual knowledge and students’ sexual behaviors and sexual attitudes.
| Perceived STI Related Knowledge | Index-based HIV and STI Related Knowledge | ||
|---|---|---|---|
| Good Level N. (%) |
Poor Level N. (%) |
Total N. (%) |
|
| Excellent Good Poor |
91 (37.6) 65 (34.2) 5 (27.8) |
151 (62.4) 125 (65.8) 13 (72.2) |
242 100 190 100 18 100 |
| Total | 161 (35.7) | 289 (64.3) | 450 100 |
χ2 = 1.055, p = 0.590.
| Variables | OR [95% C.I.] | P-value |
|---|---|---|
| Age 15-16 years (ref) 17-18 years 19-20 years |
- 1.4 [0.8-2.1] 1.5 [0.8-2.8] |
- 0.163 0.162 |
| School type Public school (ref) Private school |
- 1.2 [0.8-1.7] |
- 0.413 |
| Father’s education level ≤ 12 years (ref) > 12 years |
- 1.6 [1.1-2.4] |
- 0.040 |
| Mother’s education level ≤ 12 years (ref) > 12 years |
- 1.8 [1.2-2.8] |
- 0.010 |
| Variables | AOR [95% C.I.] | P-value |
|---|---|---|
| Masturbation daily Yes (ref) No |
- 0.7 [0.4-1.0] |
- 0.072 |
| Had sexual experience in the past Yes (ref) No |
Ref 0.8 [0.5 - 1.2] |
- 0.260 |
| Had a friend who had any sexual experience Yes (ref) No |
- 0.6 [0.4 - 1.8] |
- 0.093 |
| Most men practice sexual intercourse before marriage Yes (ref) No |
- 0.9 [0.6 - 1.7] |
- 0.889 |
4. DISCUSSION
It is well known that several factors are associated with young people’s sexual health behaviors and negative attitudes (i.e. premarital sex, multiple sex partners), and outcomes including a lack of knowledge and the sources of information regarding HIV and STIs. In this study, the majority of the surveyed adolescents reported their level of knowledge as excellent and good. Yet, when their HIV and STI related information was investigated, the results showed that most adolescents were having poor sexual knowledge. In line with this, a systematic review study from the Middle East countries has found a general lack of sexual and reproductive health knowledge [19]. Thus, the finding of this study indicates a huge gap in sexual health-related knowledge, which must be seriously tackled by policymakers and educational authorities in Saudi Arabia. Sexual health education activities conducted by the school nurses and health educators can assist in increasing knowledge and fostering informed decision making in teens. It has been suggested that sexual health education is effective in increasing sexual knowledge [8], as well as vital for STIs prevention [9].

This study found that Saudi adolescents rely on multiple sources of information about sex-related issues. Consistent with previous research, the adolescents in this study relied heavily on friends and the media for sexual information [13, 14, 20]. They received less information from reputable sources such as schools, health professionals, health services and parents. Communication with parents regarding sexual health issues was reported to be limited. It is obvious that a gap exists between Saudi parents and their sons in discussing sexual health-related issues. Similarly, a lack of communication has been reported among female adolescents in Saudi Arabia [21]. This finding can be explained due to cultural taboos on such topics, societal denial, and a lack of awareness of the importance of empowering adolescents through correct information and knowledge. The information received from peers and mass media is sometimes misleading and can cause serious damage to a student’s perceptions of and attitudes toward risk behaviors. These findings support the suggestion that peers, media and the internet play far more important roles in the lives of adolescents than do family members. Often, because of cultural obstacles, many adolescents do not feel comfortable discussing sex-related issues with their parents [22, 23]. This may leave them at a high risk of sexual-related behaviors and other associated problems. Further work is needed to determine whether parent-related knowledge of adolescent sexuality is associated with improving their adolescents’ sexual related knowledge.
This study investigated the relationship between adolescents’ HIV and STI related knowledge with its determinants (e.g. adolescents’ socio-demographic) and outcomes (e.g. adolescents’ sexual attitudes and sexual behaviors). One of the findings that should be emphasized is the adolescents with a lower level of HIV and STI related knowledge belonged to parents with a lower level of education, and this is consistent with a previous study [24]. Moreover, logistic regression analysis showed that having good sexual knowledge was not associated with adolescents’ sexual behaviors and attitudes. This is consistent with several previous studies [11, 25, 26], reporting no association between level of sexual knowledge and sexual behaviors and attitudes among adolescents, suggesting that sexual health-related issues sometimes appear to be contradictory and confusing. It has been stated that people’s sexual behaviour is ‘a complex private activity, being subject to social, cultural, moral and legal issues’ [27]. In line with that, adolescent sexual behaviour is influenced by several compound set of interactions of biology, individual perceptions, personality characteristics and values, and socio-cultural norms [28], implying that sexual behaviour is not a simple phenomenon with a few determinants.
Information about sexual knowledge and STIs/STDs in Islamic countries, where premarital and non-marital sex and homosexuality are prohibited by religion, is notably limited. An assumed low prevalence of risky sexual behaviors and STIs, as well as the cultural unacceptability of non-marital sex, cultural denial, and a lack of awareness, is the expected reason for this limited knowledge. Thus, it is vital that sex education in schools be implemented for the benefit of adolescents. School can be an important setting for children and adolescents to gain direct knowledge, attitudes, and experience. School settings provide an important opportunity to reach large numbers of young people with sex education before they become sexually active [10]. To make this educational experience more successful and effective, it is critical to pay attention to students’ needs and the school environment as a whole. Thus, it would be important to make sexual health education compulsory in schools and part of the school curriculum. National policies and comprehensive strategies addressing adolescents’ needs are urgently required in Saudi Arabia to promote healthy behaviors and prevent risky ones among adolescents [6, 18, 29, 30].
Potential limitations of this study must be acknowledged. First, the main factors limiting the study were cultural taboos. Adolescent students in middle school were not included in this study. Although health risk behavior starts at an early age, asking young children sexual health-related questions would not be permitted. Also, for political and cultural reasons, adolescent female students were not included in this study. Moreover, due to sensitivity issues or perceived inappropriateness, some of the more detailed questions such as type of sexual behaviors and homosexuality could not be asked. A third potential limitation was the cross-sectional nature of the study and the resulting inability to infer causation. Finally, due to a feasibility issue, as well as limited resources, the findings sought from this study could not be generalized for the whole country. Thus, further research in this area should be implemented in the near future.
CONCLUSION
The finding of this study is conclusive that the majority of male adolescents had an inaccurate perception regarding their sexual knowledge and poor level of STIs related information. This study has important programmatic and policy implications. First, the priority is to be given for adolescents’ education regarding sexual health-related issues including STIs/STDs. Also, findings from this study can persuade researchers, practitioners, and policymakers to establish and develop policies that provide optimal conditions for safe adolescence and adulthood. Furthermore, to better understand youth and create effective interventions, encouragement of and support for research investigating adolescent sexual health-related issues are highly needed.
LIST OF ABBREVIATIONS
| HIV | = Human Immunodeficiency Virus |
| AIDS | = Acquired Immunodeficiency Syndrome |
| STI | = Sexual Transmitted Infection |
| SPSS | = Statistical Package for the Social Sciences, also known as IBM SPSS Statistics |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study protocol and tools were approved by the Ministry of Education, Ethical Review Committee, Riyadh, Saudi Arabia.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
To ensure the patient's consent; the researcher indicated to adolescents that their participation in the study was totally voluntary and that they could refuse to take part in the study.
AVAILABILITY OF DATA & MATERIALS
The data that support the findings of this study are available from the corresponding author, [A.A], upon reasonable request.
FUNDING
None.
CONFLICT OF INTEREST
The author declares no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The author would like to thank the Ministry of Education and all schools and students who participated in this study.

