All published articles of this journal are available on ScienceDirect.

Errors in Condom Use in the Setting of HIV Transmission: A Systematic Review
Authors Info & Affiliations
Abstract
Background:
The efficacy of condom use in declining HIV transmission may be compromised by their incorrect usage. Much focus has been paid on the regularity of condom usage but consumer mistakes and challenges must be considered. Breakage, slipping, leakage, incomplete use and other problems during the sexual event may compromise the protective role of the condom.
Objective:
To evaluate through a systematic review of published data, the type, and incidence of error and problems in condom use, and their possible role in reducing the preventive action of condoms.
Methods:
A systematic literature search for peer-reviewed articles published between January 2000 and January 2019, issued in English in peer-reviewed journals, and reporting the occurrence of condom errors/problems among HIV high-risk populations.
Results:
Twenty studies representing nine countries met the inclusion criteria. The most predominant mistakes associated with condom use included condom breakage, slippage, delayed condom application, early removal, issues related to erection loss and difficulties with fit and feel were reported, failure to squeeze out air, use of expired condoms, reuse of condom, and wearing the condom outside out were other issues noticed.
Conclusions:
Condom use problems and mistakes are prevalent across the globe. Educational efforts are needed to empower HIV the at-risk population with confidence and knowledge to improve correct condom use and increase preventive activity
1. BACKGROUND
Since the first description of the human immunodeficiency virus (HIV) more than 35-years ago, its high transmission rate continues to pose serious public health concerns around the globe [1]. Statistics from the World Health Organization (WHO) estimates that the virus has infected more than 70 million people since the first case was discovered in 1981 50% of whom have succumbed to the infection [2]. The WHO further projected that by the conclusion of 2017, between 31-43.9 million worldwide were HIV positive, with the highest rates (24.9 million) occurring in sub-Saharan Africa. In the United States (US), 93% of the 44,000 new cases of HIV reported in 2014 were mainly transmitted through sexual means [3]. As per the Center for Disease Control and Prevention (CDC) publication, a significant proportion of the incidences were detected among individuals who failed to apply condoms completely, or used incorrectly, and/or inconsistently [1, 4, 5].
Even though beyond 80% of the 1.2 million HIV positive Americans know their HIV status and 40% are receiving antiretroviral therapy (ART), the rest (approximately 20%) are unaware that they are infected and may spread it to others [6]. Likewise, a significant number of HIV-negative people have no idea of the status of their sexual partners [7]. Besides, other empirical findings suggest that the adoption of ART is known to help in the deterrence of HIV transmission by suppressing viral load in the victim’s blood, implying that undetectable viral load is ‘untransmittable’ during sex [8]. Nonetheless, a significant number of HIV patients do not observe the optimal degree of medication compliance that is needed to curb viral multiplication; therefore, they may still pass on the virus to their partners [7, 9-12]. Irrespective of an individual's level of compliance to ART or his or her HIV status awareness, it is projected that the right and constant use of condoms decreases the odds of spreading HIV via sexual means by 70% in both heterosexual couples and men having sex with men (MSM) [13, 14]. As such, behavioral strategies that ensure the availability of condoms have been the backbone of HIV mitigation attempts at the community, local, state and national levels in most countries. Regularly, Condom Distribution Initiatives (CDI), which are frequently employed in combination with other strategies, like health promotion activities and awareness creation, intent on ensuring condoms are extensively accepted, availed, and/or accessed by people at increased risk of acquiring HIV [7]. Malekinejad et al. posit that the application of many interventions alongside CDI enables public health efforts to straightforwardly and incidentally heighten the impact of CDI by revealing the socio-economic, attitudes, knowledge, and behavioral factors that shape condom use [1].
Nonetheless, the efficacy of condom applications in declining incidences of HIV, especially in high-risk populations, is compromised by lack and incorrect usage of the condom by the consumers [15]. For instance, the WHO outlined that the male condom has a specific failure rate of 15%, and 2% when used correctly as a birth control measure [2]. Extrapolated over the global population, this four-fold disparity poses significant consequences for the world's growth in population and, subsequently, health resources. The difference between incorrect and precise use has comparable relevance for the mitigation of Sexually Transmitted Infections (STIs) and HIV, implying that thousands of new infections can be prevented by enhanced user efficiency. The incongruity between perfect and typical rates of letdowns is ascribable to the amalgamation of both erroneous and unreliable use [15]. Considerably, much focus has been paid on the regularity of condom usage, and few studies have highlighted the specifics of consumer mistakes and challenges. Besides, there is a wealth of literature on the evaluation of distribution interventions instead of mistakes incurred during use. For instance, two recently published systematic analyses investigated the influence of condom use on HIV prevention in communities, but they diverged on the description of “community.” While Moreno et al. considered “community” to represent a geographical setting, like a district or city [16], Charania et al. used the term to imply institutions and establishments that host non-geographically demarcated sub-groups, like “the MSM community” [17]. In both studies, “community” is utilized incorrectly and, as a pragmatic issue, it is best for scientific reviews to encompass investigations employing the two perspectives [16, 17]. Moreover, while the former included randomized controlled trials (RCTs) from all over the world except the U.S, the latter incorporated many US-based non-RCTs and RCTs. Also, none proved if CDI decreased the occurrence rate of HIV, but both articles found a positive correlation between CDI and behavioral outcomes.
1.1. The Rationale of the Study
Regrettably, there are few investigations that have paid attention to the assessment of the correlates and prevalence of errors and problems that individuals may encounter when wearing condoms [18]. In this context, errors imply those practices that result in the wrong use of the condom, such as removing during the sexual act or exposing the condom to sharp appliances, while problems are those occurrences that are not straightforwardly within the control of the user, but may reduce the efficacy of its purpose. The issues may include challenges with fit and feel, slippage, breakage and erection difficulties [18]. Notably, neglecting to justify condom use errors and problems can result in false inferences with respect to condom efficacy or appraisal of deterrence initiatives. Besides, the suggested mistakes and problems may not only reduce the effectiveness of condoms in the mitigation of new HIV infections but may also dampen its uptake by causing frustrations or if users experience less pleasurable sex life due to them.
2. OBJECTIVE
The aim of the systematic review is to investigate the occurrence and the associated impacts of errors in condom use among populations at high risk of HIV infection.
3. METHODOLOGY
3.1. Search Strategy
Hand and automatic searches were conducted to guarantee the inclusion of all the appropriate studies. The automatic query was performed in three online databases, namely: PubMed, EMBASE, and PsychINFO for English papers published between January 2000 and January 2019. The search was limited to the aforementioned time frame since a previously published systematic review had covered articles published between 1995-2012. The search was done using a combination of diverse Boolean phrases, including: [“human immunodeficiency virus” or “HIV”, “acquired immunodeficiency syndrome” or “AIDS”] and [“condom failure rates” or “incomplete use” or “condom errors”] and [“homosexual” or “sexual” or “coital” or “heterosexual” or “anal” or “intercourse” or “oral”]. Due to indexing gaps, a hand search of key journals, including AIDS and Behavior, AIDS, and AIDS Education, that often issue research on Sexually Transmitted Infections (STI) and HIV was carried out to locate extra intervention studies (Appendix. 1).
3.2. Study Selection
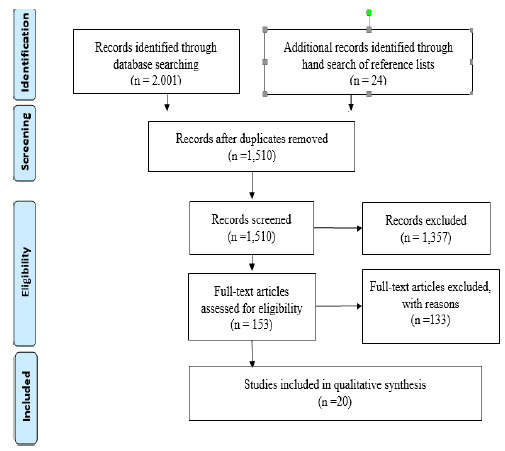
Articles were selected if 1) reported on the occurrence of condom errors/problems among HIV high-risk populations (MSM, serodiscordant couples, female sex workers) irrespective of study design, 2) if they were published between January 2000 and January 2019, and 3) it is issued in English, and the full text is available in a peer-reviewed journal. Out of the n=2,025 relevant studies, n=515 duplicate citations were removed. Abstracts of the n=1,510 articles were further screened leading to the elimination of another n=1357. Of the remaining n=153 studies, n=133 did not meet the inclusion criteria. Therefore, only n=20 investigations met the inclusion criteria and they were selected for appraisal in the systematic review (Fig. 1).
Two authors [AMJ & MDS] independently extracted data from the selected articles using standardized forms. For every investigation, the reviewers extracted the following data: citation, research framework, methods, study setting, outcomes, results, and limitations. The two reviewers then matched the extracted information and resolved differences through discussion and consensus. The methodological quality of all the selected papers was assessed using the Critical Appraisal Skills Programme (CASP), and all of the studies that met the systematic review’s inclusion criteria were presented in a tabular format (Table 1). The extracted data were synthesized thematically by first assembling the outcomes as per their quality, classifying the results based on the similarity in meaning, and lastly, subjecting the groupings to generate a single detailed set of synthesized results. Eventually, the findings were documented and reported in accordance with the PRISMA guidelines.
4. RESULTS
4.1. Characteristics of the Studies
Twenty studies conducted in nine countries fulfilled the inclusion criteria, and they documented outcomes for the use of condoms for either anal or vaginal penetration or both. Of the twenty articles, two were systematic reviews [18, 19], seven employed surveys [20-26], ten were cross-sectional [19, 27-36], and one was a simulation-based study that used structural-modeling [36]. Most of the studies took place in the United States (n=8), and one each in Canada, Scotland, China, South India, Cambodia, Italy, Croatia and Australia. Excluding the systematic reviews, 44% (n=8/18) involved men having sex with men, 11% (n=2/18) involved heterosexual men, 5.6% (1/18) on discordant couples, another two involved female sex workers and asylum seekers, while 16.7% (n=3/18) were heterosexual male and females.
Generally, two kinds of incidence approximate are considered, namely: 1) the fraction of respondents reporting an error(s) or problem(s) during condom use within a certain follow-up period, or 2) percentage of occurrences for which a problem or a failure transpired. Even though diverse terms were employed across the reviewed articles, the errors and mistakes were categorized into four major themes, namely: 1) problems associated with condom failure, slippage, or breakage, 2) incomplete use (including failing to wear the condom from the start to the end of intercourse, comprising of removal before the end of the act, or late application), 3) other mistakes, such as failure to check the expiry date, exposure of the condom to sharp objects, failure to squeeze out the air at the tip, wearing it inside out, re-use of the condom, and poor storage. Finally, 4) are the challenges with condom-related erection problems, including the fit/feel of condom, and erection loss during intercourse or while rolling on.
4.2. Condom Failure: Slippage or Breakage during Intercourse
Condom breakage frequencies varied from 3% to 37% among the respondents across n=10 studies [20, 22-25 , 27, 29-39]. Eight of the studies that reported breakage showed that the prevalence rates of slippage ranged between 2.1% and 28%. Some of these investigations detailed the exact time of the slippage during the sexual encounter (either when applying or when rolling out of the penis), while a number did not discuss the timing. Nonetheless, guesstimates for slippage at condom application and during withdrawal vacillated between 9% and 16% [27, 29]. Two studies identified ethnic/racial differences in terms of slippage rates. Black respondents posted a slippage frequency of condom twice as high than in their White counterparts. Leakage was also noted in one study [39].
| Author | Objectives | Design | Population | Findings | Limitations |
| Crosby et al. [18] | To explore the occurrence of self-reported condom use errors among Black MSM and to match the observed frequency with HIV serostatus. | Cross-sectional comparative study. | n=369 young Black MSM aged between 15-29 (US). |
Condom slippage and breakage were common among MSM, an issue that is associated with anal sex as opposed to vaginal penetration. Other prevalent condom errors include early removal, condom re-use, and early removal. Slippage and breakage affected 9% and 15% of the HIV-negative men respectively, compared to 16% and 30% of the HIV-positive counterparts. There is a need for repetitive education to enhance proficiencies on correct condom use. | Relied on self-reports, which may be marked by recall bias. Convenience sampling. |
| Kim et al. [19] | To determine the rate of condom failures, particularly breakage, and the allied behavioral and demographic antecedents in the last anal sex. | Survey. | n=9005 MSM (U.S). |
4% condom breakage rate The prevalence did not vary between respondents who indicated insertive and receptive anal penetration. |
The investigation focused on self-report data on condom failure due to breakage in the last anal intercourse. Thus, it did not offer a clear picture of condom breakage over time. |
| Remis et al. [37] | To test the supposition that a significant percentage of sexual spread is occurring irrespective of condom use among MSM. | Structural modeling. | MSM in Ontario, Canada. | At the time of the investigation, approximately n=92,963 HIV-negative men used condoms in more than 1 million acts of anal intercourse, and 117,1133 others without a condom. 14% of the respondents had HIV at the baseline By the end of the study, 693 new incidences of HIV among the study population, with more than 50% of them occurring among those who used condoms, 16% and 33% via oral and anal sex, respectively. |
|
| Godall et al. [35] | To assess the relationship between the frequency of errors/problems in condom use and the occurrence of STIs among MSM in Scotland. | Cross-sectional observational study. | n=792 of MSM (Scotland). |
The multiple number of unprotected anal intercourse (UAI) were the primary measure of STI acquisition. Awareness of proper condom usage was strongly linked to reduced odds of STI infections and low condom problem scores. |
A convenient sampling of MSM attending clinics may not be representative of the community-dwelling respondents. |
| Lau et al. [22] | To explore the frequency of unreliable use of condoms among HIV discordant partners. | Cross-sectional study. | n=88 HIV discordant couples from a rural village in China. | 27.9% recounted inconsistent use of condom protection, mainly due to the inaccessibility of condoms. Surprisingly, before HIV confirmation, consistent condom use was 24%. This means that HIV diagnosis did not improve constancy. |
The data was based on self-reports, which can be impartial due to recall bias. n=20 respondents provided incomplete information. |
| Yi et al. [23] | To investigate the risk factors for the unsteady application of condoms among MSM. | Cross-sectional analysis. | n=367 randomly selected MSM from Cambodia. | Unlike previous studies, there 62.3% consistent use, but the highest was among male sex workers (78.1%). However, the population was at increased risk of acquiring HIV due to the use of drugs that caused them to either remove or disregard condoms completely. |
The investigation surveyed factors that shape the general use of a condom with no description of the specific forms of sexual positions or types of partners. |
| Sanders et al. [15] | To determine the prevalence of numerous condom use mistakes and difficulties around the world. | Systematic review. | n=50 articles were reviewed. | The most frequent errors: removal of the condom during intercourse, placing the condom inside out, improper withdrawal, failure to squeeze out air at the tip, use of non-water-based lubricants, and leaving no space at the tip. Similarly, the commonly reported problems included challenges with fit and feel, failure to erect after wearing the condom, leakage, breakage, and slippage. |
A significant number of appraised investigations were carried out in developed countries where the rates of HIV are relatively lower than in evolving nations. |
| Crosby et al. [24] | To evaluate and match condom-use mistakes and problems. | Cross-sectional survey. | n=260 college students n=142 females and n=118 males (U.S) |
11% of the respondents recalled using sharp objects to open the condom packet 83% did not change the condom between sexual acts 14% disregarded the condom during intercourse 38% wore the condom after penetrative intercourse has began Problems comprised of breakage or slippage (28%), and loss of erection when applying the condom (15%) and 10% during the act. |
The results are limited by recall bias due to retrospective self-reports Convenient sampling. |
| Bradley et al. [25] | To investigate the precipitating causes of reported breakage of condoms in the last 30-days among female-sex-workers in South India. | Survey. | n=1,928 FEMALE SEX WORKERs (S. India). |
11.4% of the surveyed participants recalled of breakage at least once in the past 30-days Breakage was more likely to happen among participants who were: widowed/divorced/separated, <20-years-old, and used alcohol |
The study did not specify the forms of sexual acts when condom breakages occurred. |
| Crosby R et al. [26] | To review self-reported occurrences of condom use-associated errors among young black men. | Cross-sectional analysis. | n=475 young African American men are attending an urban STI clinic in the U.S. | 10-25% of the participants recalled experiencing condom errors in the past two months. 40% used damaged or expired condom Re-use of condoms Low-socioeconomic status was associated with the inaccessibility of condoms Having multiple sexual partners was a predictor of condom breakage and slippage. |
The study focused on a single population (young black men). This reduces the possibility of extrapolating the findings. |
| Zoboli et al. [27] | Assess condom application proficiencies among migrants in Italy. | Cross-sectional analysis. | > 18-year-old male asylum seekers in Italy. | The results showed that literacy levels affect the extent of awareness regarding transmission mechanisms of STIs, including HIV, as well as the quality of knowledge. The authors recommended that for condom users need instructions on the best application methods. | Only male respondents. |
| Baćak & Štulhofer [28] | To evaluate the incidence and correlates of condom-associated loss of erection, delayed use, slippage, and breakage among 18-25 aged Croatian adults. | Population-based national survey. | n=1005 (n=510 men and n=495 women) 18-25 years-old Croatian adults (Croatia) |
18%, 17%, 13%, and 34% of the respondents encountered breakage, erection loss, slippage, and delayed application, respectively. Condom breakage was more probably to be recounted by. |
There was no information about the type of sexual acts associated with the condom errors. |
| Crosby et al. [29] | The study sought to test the supposition that men commonly incur condom errors with many intimate partners. | Cross-sectional. | n=271 African-American men aged between 18 and 29 years old, seeking medical care for diagnosed STD at a metropolitan clinic in the U.S. | The respondents with ≥3 intimate female partners were highly likely to experience condom mistakes compared to their counterparts with two or fewer partners. (This information is essential in planning for “triage” for developing educational programs. |
Convenient sampling Reliance on self-reports. |
| Garofalo et al. [30] | To explore ethnic/racial disparities in HIV knowledgebase in MSM aged between 16-20 years and its association with errors in condom use. | Cross-sectional analysis. | n=344 MSM drawn from continuing longitudinal investigation (U.S). |
White men scored substantially higher than their Black counterparts on HIV knowledgebase. Increased awareness of HIV transmission mechanisms was allied to fewer errors when using a male condom. |
The respondents were sampled from one residential area; thus, the findings may not be representative of other young MSM. The sample was largely comprised of Blacks. |
| Crosby et al. [31] | To determine the pervasiveness of condom damage, and the specific practices resulting in the breakage among young heterosexual men. | Online survey. | n=278 young sexually active heterosexual men (U.S). |
31.3% of the respondents recounted experiencing condom breakage in the last three penetrative vaginal sex The correlates of condom breakage included: men with a recent infection of STI and reported cases of slippage. Other errors allied to condom breakage encompassed of erection loss, failure to remove the air at the receptacle tip, and using sharp objects to open the packet. |
Reliance on self-reported data limited the reliability of the findings. |
| Crosby et al. [32] | To evaluate condom usability and the correlation between perceived and actual ability. In addition, the study sought to assess the relationship between the illustrated ability and occurrence of STIs among Black adolescent girls. | Survey. | n=522 sexually active female adolescents from the African-American communities (U.S). |
26% of the respondents reported a history of STI, while vaginal swabs of 28% of the girls were positive for at least one STI at the time of the study. Incorrect application of the condom demonstrated by the respondents on the wood model would be associated with the incidence of STIs. |
Self-reported measures limited the cogency of the findings. The results are also restricted to condom application, yet the efficacy of condoms in infection prevention covers other factors including errors of slippage, breakage, or erection loss. |
| Hall et al. [33] | To assess the ability and poise to wear condoms effectively and consistently among young music festival attendees in Australia. | Survey . |
n=288 young adults aged between 18-29 years present at a music carnival (Australia). |
77% of the participants reported being confident in using condoms. The measures of self-assurance in condom use encompassed having >5 intimate partners and being male. Paying attention to packet instructions was allied to increased confidence 37% breakage 51% and 48% slippage during the act and withdrawal, respectively High school sex education did not cause any impact on condom errors. |
Self-reports and the long recall period (12months) increased recall bias. |
| Hernández-Romieu, et al. [34] | To compute and match the prevalence of incomplete condom use and condom mistakes as well as the regularity of condom inaccuracies, erection, and fit and feel difficulties among African American and Caucasian MSM. | Cross-sectional. | n=475 MSM who used a condom in insertive sex in the past six months (U.S.). |
82% reported using condoms in the past 180days, (77% and 87% White and Black MSM, respectively). 40% of Black reported delayed/late application. There was an ethnic disparity in condom inefficiencies. Although condom use was common among Black MSM, they were more likely to incur errors than their White counterparts. This implies that unequal infection with HIV among Black MSM may be heightened by the regularity of condom errors and failures, mainly slippage and breakage problems. 54% recounted fit/feel problems. | Self-reports and a six-month recall period reduced the validity of the findings. |
| D’Anna et al. [35] | To determine the incidence of condom use failures: incomplete use, slippage, and breakage, and their association with the respondent, partner/relationship characteristics among HIV uninfected MSM. | Survey. | n=1609 MSM STI patients enlisted from a larger trial (U.S). |
There were 100% condom use in 93 main and non-main relationships respectively, and 20% of the participants reported to have not used condoms in the past 90 days. Delayed use or early removal was the major error, while erratic use was a predictor of incomplete use particularly among MSM with multiple intimate partners. |
The survey focused on a single cohort of MSM: HIV negative. Hence, the findings may not be representative of HIV positive MSM. |
| Giannou et al. [36] | To re-evaluate the efficacy of condoms in decreasing the spread of HIV among heterosexual partners. | Systematic review /meta-analysis . |
25 studies involving n=10,676 HIV serodiscordantheterosexual couples. | HIV spread was significantly low among partners who consistently used condoms than non-users. Condom use decreases the danger of HIV transmission by 70%; however, there were several imperfections including slippage and breakage. |
Most of the reviewed papers relied on self-reports which are likely to increase the risk of recall bias. |
4.3. Incomplete Use
Ten of the studies reported cases of incomplete condom use, including failure to wear the during the whole act, early removal, or late application. In two of the studies, the type of inconsistency was not indicated or the faults were pooled in reporting [39-41] and in two articles involving MSM, cases of unprotected anal sex were attributed to new HIV infections among the participants [35, 37], while one about female sex workers found a 2.6% rate of complete disregard for condom among their clients [5]. In four investigations, combined regularity of delayed condom application and early removal was shown to vary between 12.3%-38% and 14%-36%, respectively [5, 27, 32, 39] investigation, only the occurrence rate of delayed use at 34% was reported [22]. Similarly, two other studies recounted disparities of inconsistent condom application with respect to the number of partners or the type of relationship the respondents shared with their sexual partners. Crosby et al. found that 36% and 53.1% of respondents with ≤ 2 and ≥ 3 intimate partners recalled incomplete condom use in the past 60 days [29], while in another study, the rates of inconsistency differed dependent on the type of sexual partners as follows: 21.9%, 24.1%, 27.0%, 29.7%, 35.8% and 44.9% for intimate partners who were male clients, female customers, male sex workers, female sex workers, boyfriends and girlfriends, respectively [30].
4.4. Problems with “Fit” and Feel and Condom-Related Erection Difficulties
From the appraised investigations, condom-associated challenges can arise at application or during the act. Loss of penal erection can transpire during intercourse or when putting on the condom. Nonetheless, only a single study reported both cases at 15%, and 10%, respectively [32], the findings of a systematic analysis included in the present review reported a range between 14.3%-28.1% and 9.9%-20.2% at application and during sex, respectively [18]. Two other investigations did not specify whether the erection problem occurred at application or during the act but reported combined frequencies of 17% and 21%, respectively [22, 31]. One other study reported erection loss as a common cause of breakage without outlining either the proportion of respondents who suffered or the period of occurrence [23]. One study reported erection problems to be twice likely to affect respondents with ≥3 intimate partners than those with a single sexual associate [22]. Three studies reported difficulties with “fit” and feel with the prevalence of 23% and 54%, respectively [27, 31], and a range of 7.0% - 29.9% in the systematic review [18].
4.5. Other Condom-Associated Errors
As portrayed in the table, eight classifications of additional errors associated with condom use were reported in the included articles. Three papers approximated the frequency of not squeezing out the air from the repository tip, recounted by 2.05% -50% of the respondents [23, 34, 39], while 2.64% -11% of the participants in three investigations exposed the condom to sharp objects like jewelry [23, 32, 39],. One of the studies highlighted other mistakes, including 37% of participants knowingly using the expired condoms, 19.7% re-used the condom later, 29.5% wore the condom inside out and 79% failed to check for probable damages [31].
5. DISCUSSION
As illustrated in Table 1, the systematic review encompassed the synthesis of findings of 20 peer-reviewed articles published between January 2000 and January 2019, reporting on the occurrence of condom use errors and problems among HIV high-risk populations. The temporal restriction allowed for comparison of the occurrence of condom use errors and challenges identified in the previously issued integrative review that included 50 papers issued between 1995-2012 [18]. The outcomes of the current systematic review illustrated that errors in condom use are common occurrences across the globe. Besides, although most of the selected investigations involve men having sex with men, the inclusion of diverse high-risk populations, including female sex workers, refugees, young heterosexual Black and Caucasian men, HIV discordant couples, college students, and sexually active female adolescents, indicate that condom-use mistakes and problems are placing millions of individuals at increased risk of acquiring or transmitting HIV. The predominant blunders encompass failure to eradicate the air at the tip of the condom before use, erection loss during application and while having coitus, experiencing discomfort due to “fit” and feel issues, complete disregard of condom use, inconsistent application (delayed application or removal before the end of the act), wearing the condom inside out, and most commonly, slippage and breakage errors.
From the synthesis of findings, the second largest proportion of the investigations were those exploring the occurrences of breakage and slippage faults? Undoubtedly, these investigations are essential provided that ruptures and slippage are the main types of failures in condom use. As stated by one study, the errors mentioned above place the sexual partner at extremely high risk of acquiring HIV through direct contact with fluids or a penis [18]. For instance, incident approximates of late application of condoms after unprotected anal or vaginal sex are frequently extensive compared to those for slippage or breakage. Therefore, this inaccuracy may embody a more probable risk of exposure than in rupture or slip-up.
In addition, grounded on correlates of condom errors in the explored studies, it is likely that users experience slippage and breakage frequently due to the simultaneous occurrence of other errors, or risky behaviors. For instance, the wrong way of handling or rolling on the condom on to the penis by opening the packet using a sharp object has been associated with the rupture of the condom [23, 42, 43]. These studies found that slippage/breakage was common among users with multiple sexual partners, those experiencing erection loss, failure to read and follow the instruction manual, and lack of confidence to use it owing to previous experience. In this regard, breakage may also be correlated with age, such that younger individuals like students, who are considered less experienced are likely to encounter breakage than older adults [24]. In addition, individuals with a high school level of education and below, particularly among racial minorities are more likely to encounter condom breakage. This is probably owing to the failure to observe the necessary information or they have not received adequate knowledge on the best approach of avoiding errors [20].
Condom slippage or breakage can remarkably demoralize a user's drive to employ a protective condom. Equally, the absence of self-efficacy and incentive to wear condoms may result in conducts, which might elevate the probability of condom slippage or breakage. In one of the investigations, the likelihood of incurring breakage/slippage is greater among people with many other mistakes. Thus, incomplete protection by the condom causes leakage, breakage/slippage, alongside other mistakes that can result in increased vulnerability to HIV and STIs. Another study also shows that condom failure also ensues following cases of erratic or complete disregard of condoms irrespective of the sexual event [25]. Thus, impactful interventions may be accomplished by conducting an extensive assessment of the incidences of other errors and challenges that precipitate the occurrence of breakage or slippage. One such error is that of incomplete use, which was reported by most of the selected studies in the present review.
Late application or early condom withdrawal before the conclusion of the penetrative intercourse has often been explored, and empirical evidence suggests that it is regularly reported. Nonetheless, irrespective of their pervasiveness, the exact length of time users takes before putting on a condom in the delayed application is unexplained. With regards to early condom withdrawal, it is evident that problems associated with loss of erection [22, 31]., and discomfort due to “fit” and feel issues are some of the antecedents for removal before the end of the act [27, 31]. Empirical evidence strongly suggests that protected sex remains the major public health intervention in curbing the rise of new HIV infections [31], particularly among young Black MSM [36]. This review concurs noting that young men may encounter difficulties with condoms that result in loss of erection, and are frequently reported among participants having multiple sexual partners and amidst people who engage in sex while under the influence of alcohol. Erection loss due to condom use remains an under-investigated subject; however, from the presented outcomes it is a strong predictor of slippage/breakage and incomplete use [27, 39]. It is also an essential determinant of perceptions towards prospective use of a condom.Even though the current systematic review recommends the correct use of condoms to prevent the transmission of HIV infections, innovative approaches, such as pre-exposure prophylaxis (PrEP) and treatment as prevention (TasP), have been identified to be more successful than condoms [43, 44]. Therefore, the aforementioned HIV preventive techniques are suggested as alternatives of condoms. We should consider, anyway, that HIV effective treatment or prophilaxys are not available in all countries and especially in low resources ones that are, as a matter of fact, the more interested in HIV transmission. In addition, we should consider that transmission of other sexually transmitted infections still need a correct use of condom to be prevented.
6. LIMITATIONS
Although the study’s results are supported by the existing literature, heightening the findings’ validity, they still have some limitations. First, an overwhelming majority of the appraised investigations were conducted in industrialized economies, mostly in the United States. In fact, excluding two papers issued in Cambodia and South India focusing on the risk factors for incomplete use and errors when using condoms, all the other eighteen studies were carried out in the U.S, Canada, China, and European countries. Besides, the two papers mentioned above did not identify the specific types of intimate partners or sexual activity associated with condom use errors. Yet, the burden of HIV/AIDS has been acknowledged to be more widespread in developing rather than in resource-rich countries [45, 46]. Therefore, additional studies that focus on participants from a broader array of countries, especially from evolving economies, are necessary. The upshots of such analyses will influence the formulation and implementation of strategies to foster the production of consistent condoms and subsequently, reduce HIV transmissions. Another major limitation of the systematic review is that a large share of the appraised articles relied on self-reports, which are likely to suffer from recall bias. Specifically, the majority of the articles did not mention the self-reporting tools employed in collecting the participants’ data. Hitherto, the selection of self-report instruments with sufficient measurement qualities for the evaluation of condom use errors is necessary, given that the diversity of measures associated with condom use mistakes and problems are related to multidimensional constructs. Lastly, the selection of English articles only has potentially introduced language bias in the current systematic review. Therefore, further studies should focus on using other data collection techniques alongside self-reports, as well as consideration of non-English publications to avoid language bias in future systematic reviews.
CONCLUSION
Nonetheless, it is clear from the synthesized findings that condom errors, particularly slippage/breakage and incomplete use, are common among adults, youth, and sexually active adolescents. The review recommends the heightening of condom use promotion initiatives that highlight both the correct and consistent application of the condom. In this case, both patients and clients should plan ahead before intercourse, and during the act, the user should ensure the condom is not expired, create room for safe opening by pushing the condom to one corner, and avoid the use of sharp item, like fingernails, razor, or teeth, in opening the condom package. Similarly, users should learn how to correctly wear the condom, including applying it before making any contact with the partner's vaginal, oral, or anal regions. After ejaculation, the user ought to hold the base of the condom when removing to avoid leakage or slips, and in case of any form of failure during intercourse, the act should be stopped, and it is necessary to apply a new one.
CONSENT FOR PUBLICATION
Not applicable.
STANDARD FOR REPORTING
PRISMA guidelines and methodology were followed.
FUNDING
None
CONFLICT OF INTEREST
The author declares no conflict of interest, financial or otherwise.
| P(population) | HIV high-risk groups |
| I (Intervention) | Condom use |
| Comparator | Correct condom use |
| Outcome | Condom use errors and problems |
| Search terms | “MSM” or “female sex workers” AND “condom use errors” or “condom problems”. |
ACKNOWLEDGEMENTS
Declared none.

