All published articles of this journal are available on ScienceDirect.

A Randomized Controlled Trial on the Usefulness of Mobile Text Phone Messages to Improve the Quality of Care of HIV and AIDS Patients in Cameroon
Authors Info & Affiliations
Abstract
Background:
HIV and AIDS are major public health problems in the world and Africa. In Cameroon, the HIV prevalence is 5.1%. Cellphones have been found to be useful in the provision of modern health care services using short message services (SMS). This study assessed the effectiveness of SMS in improving the adherence of people living with HIV and AIDS to their treatment and care in Cameroon.
Methods:
This intervention study used a randomized controlled trial design. Ninety participants seeking treatment at the Nkwen Baptist Health Center were recruited between August and September 2011 using a purposive sampling method. They were randomly allocated into the intervention and control groups, each containing 45 participants. In the intervention group, each participant received four SMSs per week at equal intervals for four weeks. The patients were investigated for adherence to ARVs by evaluating the number of times treatment and medication refill appointments were missed. Data were collected using an interviewer-administered questionnaire before and after intervention and analysed on STATA.
Results:
The baseline survey indicated that there were 55(61.1%) females and 35(38.9%) males aged 23 - 62 years; the mean age was 38.77 ± 1.08. Most participants were teachers [12 (13.3%)], farmers [11 (12.2%)], and businessmen [24 (26.7%)]. Adherence to ARVs was 64.4% in the intervention group and 44.2% in the control group (p = 0.05). 2(4.4%) patients in the control group failed to respect their drug refill appointments while all the 45(100%) participants in the intervention group respected their drug refill appointments. 54.17% of married people and 42.9% of the participants with primary and secondary levels of education missed their treatment. Key reasons for missing treatment were late home coming (54%), forgetfulness (22.5%), and travelling out of station without medication (17.5%). Other factors responsible for non-adherence included involvement in outdoor business (60.87%), ARV stock out (37.8%), and not belonging to a support group (10.23%). Twenty eight (62.22%) subjects in the intervention group were able to take their treatment regularly and on time.
Conclusion:
SMS improved adherence to ARVs. Key constraints which affect adhere to ARV medication can be addressed using SMS.
INTRODUCTION
Human Immunodeficiency Virus (HIV) is a public health problem all over the world. Anti-Retroviral Therapy is one of the main ways of controlling infections with HIV. Excellent adherence to ART is essential to avoid the development of resistance; hence, treatment should not be interrupted [1]. Adherence to antiretroviral therapy is a powerful predictor of survival for individuals living with HIV and Acquired Immunodeficiency Syndrome (AIDS) [2]. If adherence to Anti-retrovirals (ARVs) is not kept above 90%, HIV can develop mutations that lead to drug resistance. This makes first line ARVs ineffective thereby worsening the epidemic.
According to Rabkin and colleagues [3], missing even a few doses of ARV treatment a week risks viral resistance and treatment failure; and may be worst in the long run than taking no medication at all. The quality of care and adherence to ARV treatment has witnessed a decline in follow up and an increase in defaulting [4].
Mobile phones are becoming ever more important in African nations particularly in the health context where they have increased the efficiency of service delivery to the poor [5]. In Yaounde, Cameroon, studies by Rougemont and co-workers [6] indicated that care delivery to people living with HIV and AIDS could be improved through the use of cellphones using Short Message Services (SMS). Data for 2010 showed that globally, over 33.3 million people (up from 28.6 million in 2001) were living with HIV giving a prevalence of 0.8 % and 5,254,000 people were on ARV treatment giving an ARV coverage of 36% [7]. By the end of 2010, 34 million people worldwide were living with HIV and AIDS.
In Sub-Saharan Africa, over 22.5 million people (prevalence of 5.0%) were infected with the virus and over 3.9 million of them were on ARV treatment [7]. In 2009, 610,000 people were living with HIV in Cameroon [8] and 76,228 people were on ARV. In 2010, 249,341 people were eligible for HIV treatment in Cameroon but only 88,589 people were on ARVs. By June 2011, according to the National AIDS Control Committee [9], the number of people on ARVs in Cameroon was 97,418.
When patients are not closely monitored right from the initial stage, some may be lost to follow up. The Cameroon Ministry of Public Health [10] revealed that out of the 37,081 patients on treatment by the end of June 2007, only 34,788 came back at the end of September 2007. About 6.2% of the patients (2,293) dropped out of active treatment during this quarter [10]. The HIV prevalence in Cameroon is 5.1% with regional variations but the North West Region had the highest prevalence of 8.6% in 2010 [11].
Many studies have been carried out to measure adherence using various approaches such as self-reports, clinical assessments, pill counts, drug refills, directly observed therapy, and biological assays among others. This study was undertaken to assess the usefulness of cellphone text messages to improve the adherence of HIV and AIDS patients to their treatment and care in the North West Region of Cameroon.
MATERIALS AND METHODS
Study Area
This study took place in the Bamenda Health District which is found in the North West Region; a savannah zone of the Republic of Cameroon. The Region has a population of 2,297,710 inhabitants spread over a total surface area of 17,500 Km2 with an average population density of 131 inhabitants per Km2 and an HIV prevalence of 8.6%.
The Bamenda Health District is located in the Regional Headquarter of Bamenda. The district has a population of 341,864 inhabitants spread over 17 Health Areas with 17 Health Centers, 11 clinics, 6 nursing homes, and 16 pharmacies that take care of the population. The district has 4 treatment centers for people living with HIV and AIDS: Mezam Polyclinic (lay private facility), St. Mary Health Center, Nkwen Baptist Health Center, and the Bamenda Regional Hospital.
The Bamenda Health District has an undulating topography with wonderfully green scenery in the rainy season. It has two seasons; the rainy and dry seasons. The road network in the district is good with a majority of the Health Areas linked to the District Health Service by tarred roads. The district has characteristics of a highly cosmopolitan town with people of all ages, sexes and all works of life and social classes. The population is constituted of people from many tribes and regions of the country.
The Nkwen Baptist Health Area where the study took place has a treatment center which receives on average 2,000 people living with HIV/AIDS (PLWHIV) on ARV treatment a year.
Study Design and Setting
The study was an intervention study that used a randomized controlled trial design. It was a hospital-based study among PLWHIV. It used self-reports of participants where timely and regular taking of ARVs as well as respecting medication refill appointments were instituted as the main indicators to assess adherence to treatment at baseline. The treatment center at the Nkwen Baptist Health Area receive patients not only from the region but also from other towns of the country like Mamfe, Bafoussam, Douala, Buea, and Yaounde among others.
Sample Size Determination
A sample size of 90 patients was recruited from the Baptist Health Center-Nkwen, Bamenda. In calculating the sample size for this study design, the following considerations were made: the minimum difference or the effect size was set at 25% assuming that the adherence rate before the study was 70% and that adherence would be at 95% after the intervention. The power was set at 80% to detect this difference of 25% in adherence between the control and intervention groups. The statistically significant difference was set at 0.05. The proportion of individuals in the two groups was the same giving a ratio (r) of 1.
The sample size of 86 was thus calculated using the STATA command: sampsi p1p2, p(0.8) r(1) in the STATA statistical software version 9, but 90 was retained for the study (45 in the intervention arm and 45 in the control arm).
Study Population
The study population was made up of all people living with HIV and AIDS, who sought treatment and care at the Baptist Health Center in Nkwen between August and September, 2011. This site was chosen through simple random selection. There were four treatment centers in Bamenda Health District, one of which was selected randomly. The study sample was 90 people (35 males and 55 females).
Those who were eligible for the study were from 18 years of age and above, owned a cellphone, were able to read SMS, had been on ARVs for at least one month and actually gave their consent to take part in the study by signing the consent form.
Those who accepted to take part in the study were serially registered on a list. This process went on regularly until a total of 90 persons were purposively sampled (Fig. 1). Each eligible person had the chance to be selected once, therefore, those who visited the treatment center more than once within the recruitment period were not considered again during their subsequent visits.
All the 90 participants were recruited before they were randomly allocated to the two groups. Using this serially numbered list of 90 participants, ballots were prepared and we randomly drew out numbers without replacing until we got 45 patients in group A and 45 in group B.
Group A was the intervention group and group B was the control group. The serial numbers represented the participants’ codes. Participants in the intervention group, besides their standard treatment and care, received educative SMS messages; while those in the control group received only their standard treatment and care. The intervention was mainly sending cellphone SMS to patients which started immediately after random allocation. The same series of messages were sent to each participant in the intervention group four (4) times a week for four (4) weeks. The messages were sent between 5-7 a.m and between 4-6 p.m.
The time of sending messages to participants varied because patients had different times that they always take their medications.
Ethical Considerations
An administrative clearance for the study was obtained from the Faculty of Health Sciences of the University of Buea and the Regional Delegate of Public Health for the North West Region. An ethical clearance was obtained from the Cameroon Baptist Convention Institutional Review Board to carry out the study. The respondents signed a consent form which contained the necessary information explaining the procedures, risks, discomfort and person to contact when more information is needed among others.
Data Collection
Data was collected by administering questionnaires to respondents in two phases. One set of questionnaires was administered at the beginning of the study to collect baseline data and another set at the end of the period of intervention to collect data for comparison. These questionnaires were administered and data collected immediately because they were interviewer-administered questionnaires. These two sets of data were then compared to ascertain the effect of the intervention. In the second set of data, the difference in adherence was also established between the intervention and control groups.

Flow diagram showing recruitment and random allocation of study participants into intervention and control groups.
Data Management and Analysis
The questionnaires were filled on clinic days and cross checked daily during the data collection period for completeness and correctness. Missing or incomplete data was collected from the patients during the next clinic days. The data were entered into excel spread sheets. The complete and edited data set was imported into the STATA software version 10.1 [12], serial number 1919525597 [12], for statistical analyses. P-values were based on t-test for the comparison of means, and chi-square test for the comparison of proportions at 95% confidence level.
RESULTS
Participants included 45 PLWHIV in the intervention group and 45 PLWHIV in the control group. The demographic characteristics of the participants are shown in Table 1.
Demographic characteristics of the study participants.
| Demographic Characteristics |
Baseline | Randomized Control Trial | ||||
|---|---|---|---|---|---|---|
| No (%) | Intervention No (%) |
Control No (%) |
p-value | |||
| Age (years) | 21-30 | 23(25.6) | mean | 38.76 | 38.74 | 0.30 |
| 31-40 | 33(36.7) | |||||
| 41-50 | 20(22.2) | Std. Err. | 1.64 | 1.43 | ||
| 51-60 | 12(13.3) | |||||
| 61-70 | 2(2.2) | 95% CI | 35.44 – 42.07 | 35.85-41.64 | ||
| Total | 90(100.0) | |||||
| Gender | Male | 35(38.9) | 18(51.4) | 17(48.6) | 0.96 | |
| Female | 55(61.1) | 27(49.1) | 28(50.9) | |||
| Total | 90(100.0) | 45(50.0) | 45(50.0) | |||
| Education | Primary | 36(40.0) | 17(47.2) | 19(52.8) | 0.35 | |
| Secondary | 35(38.9) | 17(48.6) | 18(51.4) | |||
| High school | 14(15.6) | 9(64.3) | 5(35.7) | |||
| University | 5(5.6) | 2(40.0) | 3(60.0) | |||
| Total | 90(100.0) | 45(50.0) | 45(50.0) | |||
| Marital status | Married | 48(53.3) | 26(54.2) | 22(45.8) | 0.62 | |
| Single | 28(31.1) | 14(50.0) | 14(50.0) | |||
| Divorced | 2(2.2) | 1(50.0) | 1(50.0) | |||
| Widowed | 12(13.3) | 4(33.3) | 8(66.7) | |||
| Total | 90(100.0) | 45(50.0) | 45(50.0) | |||
| Occupation | Teaching | 12(13.3) | 7(58.3) | 5(41.7) | 0.38 | |
| Farming | 11(12.2) | 5(45.5) | 6(54.5) | |||
| Business | 24(26.7) | 11(45.8) | 13(54.2) | |||
| Jobless | 4(4.4) | 2(50.0) | 2(50.0) | |||
| Driving | 9(10.0) | 7(77.8) | 2(22.2) | |||
| Others | 30(33.3) | 15(50.0) | 15(50.0) | |||
| Total | 90(100.0) | 45(50.0) | 45(50.0) | |||
| Religion | Catholic | 36(40.0) | 19(52.8) | 15(47.2) | 0.64 | |
| Presbyterian | 32(35.6) | 17(53.1) | 15(46.9) | |||
| Baptist | 14(15.6) | 5(35.7) | 9(64.3) | |||
| Others | 8(8.8) | 4(50.0) | 4(50.0) | |||
| Total | 90(100.0) | 45(50.0) | 45(50.0) | |||
ADHERENCE TO ARVs IN THE INTERVENTION AND CONTROL GROUPS
The number of times patients missed treatment for one month in each study arm is shown in Fig. (2). The association between the treatment duration and ARV adherence is shown in Table 2. However, two patients could not provide complete information on treatment duration and adherence to ARVs. Out of the 40 respondents who defaulted treatment, 13 (32.5%) had been on treatment only for one year, and 10 (25.0%) only for two years.
Association between duration of treatment and ARV adherence.
| Duration since on ARV treatment (years) | Defaulted No (%) |
Adhered No (%) |
Total No (%) |
|---|---|---|---|
| 1 | 13(32.5) | 10(20.8) | 23(26.1) |
| 2 | 10(25.0) | 9(18.8) | 19(21.6) |
| 3 | 7(17.5) | 13(27.1) | 20(22.7) |
| 4 | 9(22.5) | 8(16.7) | 17(19.3) |
| 5 | 1(2.5) | 3(6.3) | 4(4.5) |
| 6 | 0(0.0) | 1(2.1) | 1(1.1) |
| 7 | 0(0.0) | 3(6.3) | 3(3.4) |
| 8 | 0(0.0) | 1(2.1) | 1(1.1) |
| Total | 40(45.6) | 48(54.5) | 88(100) |
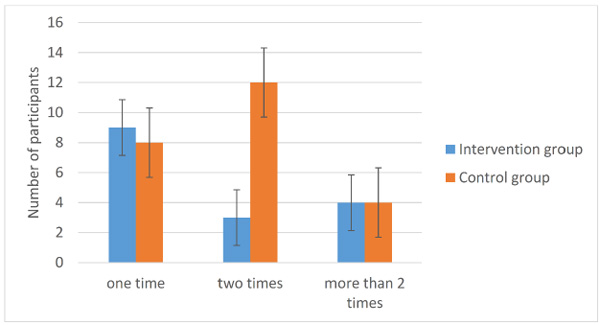
Number of times patients missed treatment for one month in each study arm.
FACTORS CONTRIBUTING TO NON-ADHERENCE TO ARVs
Reasons why patients missed treatment are shown in Table 3. Some of the reasons why people do not belong to support groups (Table 4) accounted for some of the factors that contribute to non-adherence to ARVs as shown in Table 3. From Table 4, 11(12.2%) patients could not provide any reason for non-adherence to ARVs. Coming back home late or unable to respect medication schedule (45%), travelling out of station without medication (17.5%) and forgetfulness (22.5%) were the most prominent reasons why people missed taking their drugs.
From Table 4, majority [29 (36.7%)] of respondents in both the intervention and control groups were not aware of the existence of support groups, 21 (26.6%) were very busy, while 10 (12.7%) indicated they were still to join. Some said they did not want to join while others said they did not have the money to register into support groups, 5 (6.3%) and 6 (7.6%) respectively.
Reasons why people missed ARV treatment in the Nkwen Baptist Health Area in 2011.
| Reasons | Total (%) | Intervention with SMS No (%) |
Control No (%) |
p-value |
|---|---|---|---|---|
| Came back home late [Unable to Respect medication schedule] |
18(45.0) | 12(75.0) | 6(25.0) | 0.002 |
| Drugs not available | 2(5.0) | 0(0.0) | 2(8.3) | |
| Forgot | 9(22.5) | 0(0.0) | 9(37.5) | |
| Got up late | 2(5.0) | 0(0.0) | 2(8.3) | |
| Travelled and forgot taking drugs along | 7(17.5) | 2(12.5) | 5(20.8) | |
| Very busy | 2(5.0) | 2(12.5) | 0(0.0) | |
| Total | 40(100) | 16(40.0) | 24(60.0) |
Reasons for not belonging to support groups in the Nkwen Baptist Health Area in 2011.
| Reason | Total No (%) |
Intervention No (%) |
Contro l No (%) |
p-value |
|---|---|---|---|---|
| Lack of money to register | 6(7.6) | 2(4.9) | 4(10.5) | 0.214 |
| Does not want to join | 5(6.3) | 2(4.9) | 3(7.9) | |
| Hates being in groups | 1(1.3) | 1(2.4) | 0(0.0) | |
| Husband refused | 1(1.3) | 0(0.0) | 1(2.6) | |
| Not aware | 29(36.7) | 16(39.0) | 13(34.2) | |
| Just negligence | 1(1.3) | 0(0.0) | 1(2.6) | |
| No Support Group in my area | 3(3.8) | 3(7.3) | 0(0.0) | |
| Still to join | 10(12.7) | 3(7.3) | 7(18.4) | |
| No confidentiality in SG* | 2(2.5) | 0(0.0) | 2(5.3) | |
| Very busy | 21(26.6) | 14(34.1) | 7(18.4) | |
| Total | 79(100) | 41(51.9) | 38(48.1) |
*SG= Support Group
LEVEL OF ACCEPTANCE OF THE USE OF CELLPHONE SMSs IN THE CARE OF PLWHIV
The results obtained from the intervention arm of the study about SMSs revealed the following information as presented in Table 5. More than half [26 (57.8%)] of the respondents who received SMSs indicated that the messages were good and wished that they should continue. Of all responses, 9 (20%) of the respondents indicated that they were very happy because the messages were encouraging. Also, 9 (20%) of the respondents indicated that the messages gave them psycho-social support. Proposals sought from patients to improve treatment and care is presented in Table 6. From Table 6, 25 (28.4%) participants wished that drug refill (appointments for drug refills) should be done every two months rather than every one month. Out of this number, 10 were in the intervention group and 15 were in the control group. Of the 45 respondents who received SMS messages, 15 (17%) wished that SMS messages should be sent to their phones throughout the treatment period. Thirteen (14.8%) of the respondents (5 in the intervention arm and 8 in the control arm) wished that the cost of CD4+ T cell count test be reduced and 11 (12.5%) of the respondents indicated that the center should always have drugs available for patients. Though 8 (9.1%) of the respondents indicated that they were satisfied with the present care that they were receiving, 4 (4.5%) indicated that delay time at the clinic should be reduced as much as possible.
Suggestions on improving SMSs for care of PLWHA in the Nkwen Baptist Health Area in 2011.
| Suggestions | No (%) |
|---|---|
| Encouraged on the constitution of nutritional intake | 1(2.2) |
| The messages are good, I wish they continue | 26(57.8) |
| The messages are very encouraging (Psycho-social support). | 9(20.0) |
| Very happy and encouraged by the messages | 9(20.0) |
| Total | 45(100) |
Other interventions solicited by patients to improve treatment and care in the Nkwen Baptist Health Area in 2011.
| Other interventions to improve on treatment and care | Frequency | ||
|---|---|---|---|
| Total No (%) |
Intervention No (%) |
Control No (%) |
|
| Delay (waiting) time should be reduced | 4(4.5) | 1(2.2) | 3(7.0) |
| Fills satisfied with the present care | 8(9.1) | 3(6.7) | 5(11.6) |
| Needs 2 months’ refill of drugs | 25(28.4) | 10(22.2) | 15(34.9) |
| Needs financial assistance | 4(4.5) | 3(6.7) | 1(2.3) |
| Needs assistance to help her husband | 1(1.1) | 0(0.0) | 1(2.3) |
| The center should always have drugs | 11(12.5) | 4(8.9) | 7(16.3) |
| The cost of CD4 test should be reduced | 13(14.8) | 5(11.1) | 8(18.6) |
| Health talks should be given on what to do | 1(1.1) | 1(2.2) | 0(0.0) |
| Would like to be assisted nutritionally | 3(3.4) | 1(2.2) | 2(4.7) |
| Would like to be encouraged on feeding | 2(2.3) | 2(4.4) | 0(0.0) |
| Would like to be receiving SMSs throughout the treatment period | 15(17.0) | 15(33.3) | 0(0.0) |
| Would like to have additional drugs | 1(1.1) | 0(0.0) | 1(2.3) |
| Total | 88(100) | 45(51.1) | 43(48.9) |
EFFECTS OF SMS ON THE CARE OF PLWHIV
All the 45 respondents who received SMSs in their phones acknowledged that these messages were useful for their treatment and care. The various ways by which respondents of the intervention arm felt about the effects of SMSs are shown in Table 7.
The ways by which SMSs influenced participants’ knowledge and behaviour in the Nkwen Baptist Health Area towards their treatment and care.
| Influence of SMSs to respondents | No (%) |
|---|---|
| Now knows the importance of CD4 test | 4(8.9) |
| The messages have given psycho-social support | 2(4.4) |
| The messages have helped me take my treatment regularly and on time | 28(62.2) |
| They have helped me to be cautious with my sexual life | 1(2.2) |
| They have reminded me of my appointment day | 7(15.6) |
Of the 45 respondents, 28 (62.2%) took their treatment regularly and on time because of the reminder SMSs, 7 (15.6%) were able to respect their appointment day and 4 (8.9%) indicated that they were now aware of the importance of CD4+ T cell count test in their treatment and care. The overall key findings of the study after the SMS interventions in both arms are shown in Table 8. A Comparison of the level of adherence to ARVs in baseline data with the intervention and control groups as shown in Table 9. The results in Tables 8, 9 indicate that SMSs have improved the treatment and care of people living with HIV and AIDS.
DISCUSSION
The results indicated that age (p=0.3), gender (p=0.96), level of education (p=0.35), marital status (p=0.62), and occupation (p=0.38) did not have any statistically significant relationship with the use of SMSs in both the intervention and control arms. This demonstrates and confirms the fact that the compared study groups had similar characteristics.
This study established that patients who were on standard care and received SMSs adhered to their ARV treatment more than those who received only standard care (64.4% Vs 44.2%; p=0.05). These results are in line with the results obtained by Lester and colleagues [13] and Pop-Eliches and co-workers [14] who showed that patients receiving SMSs adhered better than those who did not. The study also revealed that adherence to ARVs had a correlation with the duration of treatment as 57.5% of those who were on ARVs for more than 3 years adhered better than those on treatment for less than 3 years. We speculated that patients on ARVs for a short period of time might not yet be used to the demanding, boring and lifelong ARV treatment. Therefore, the more the number of years a patient is on treatment, the less the rate of treatment defaulting. The duration of treatment was also found to have a relationship with the use of traditional medication alongside ARVs. More of the study participants who were on ARVs for a maximum of two years were also taking traditional medication as compared to those who had been on ARVs for more than two years. This could be due to inadequate knowledge of the fact that associating traditional medication and ARVs is not medically correct as most traditional medication hardly have verifiable specifications about dosage and associated side effects. This could consequently harm rather than improve on the health of the patient.
Overall key findings after SMS interventions in both arms of the study.
| Variable | Findings | Intervention No (%) |
Control No (%) |
p-value |
|---|---|---|---|---|
| Adherence | Proportion of respondents who missed treatment in the past one month | 16 (35.6) | 24 (55.8) | 0.056 |
| Proportion of respondents who belong to Support Groups | 4(8.9) | 5(11.6) | 0.67 | |
| Proportion of respondents who failed to respect refill appointments | 0(0) | 2(4.4) | 0.15 | |
| Proportion of respondents on traditional treatment | 3(6.7) | 2(4.7) | 0.68 | |
| Factors contributing to non-adherence | Came back home late | 12(26.7) | 6(13.9) | 0.002 |
| Drugs not available | 0(0.0) | 2(4.6) | ||
| Forgetfulness | 0(0.0) | 9(20.9) | ||
| Got up late | 0(0.0) | 2(4.6) | ||
| Travelled and forgot taking drugs along | 2(4.4) | 5(11.6) | ||
| Very busy | 2(4.4) | 0(0) | ||
| Acceptance of SMS strategy | Willing to receive SMSs for treatment and care | 45(100) | 43(100) | |
| Effects of SMS messages | Now knows the importance of CD4+ T cell count test | 4(8.9) | Not applicable | |
| The messages have given psycho-social support | 2(4.4) | Not applicable | ||
| The SMSs have helped me take my treatment regularly and on time. | 28(62.2) | Not applicable | ||
| They have helped me to be cautious with my sexual life | 1(2.2) | Not applicable | ||
| They have reminded me of my appointment day | 7(15.6) | Not applicable | ||
Comparison of the level of adherence to ARVs at baseline and with the intervention and control groups.
| Variable | Baseline No (%) |
After intervention No (%) |
Intervention No (%) |
Control No (%) |
p-value |
|---|---|---|---|---|---|
| Proportion of respondents who missed their treatment in the past one month | 38(42.2) | 40(45.45) | 16 (35.6) | 24 (55.8) | 0.05 |
| Proportion of respondents who belong to support groups | 9(10.0) | 9(10.23) | 4(8.9) | 5(11.6) | 0.67 |
| Proportion of respondents who failed to respect refill appointments | - | 2(4.4) | 0(0.0) | 2(4.4) | 0.15 |
| Proportion of respondents who also take traditional treatment | 12(13.3) | 5(5.7) | 3(6.7) | 2(4.7) | 0.68 |
Patients who were married missed their treatment more often than those who were not as 54.17% of patients who missed their treatment were married. Married patients may be more involved with family responsibilities that are likely to interfere with their adherence to ARVs. Also, failing to respect drug refill appointments was observed more in the control group as opposed to the intervention group. Similar results were obtained by Rougemont and co-workers [6] where 30% of participants failed to return for drug refill. Failing to refill drugs implies interruption in treatment which contributes to poor adherence. It was demonstrated that people with a lower level of education missed their treatment many more times as compared to those with higher levels of education. This falls in line with findings by Kalichman and associates [15] that people with higher levels of health literacy adhere better to their medication.
The study revealed that there were a number of factors associated with missing treatment which directly impacted on adherence. These factors in the control group included coming home late, unavailability of drugs, forgetfulness, getting up late, and travelling without taking drugs along, as opposed to the situation in the intervention group where the factors included coming back home late, being very busy and travelling without taking drugs along (p=0.00).
The study showed that being involved in outdoor business is a factor that significantly contributes to non- adherence to ARVs as 60.87% of those who were involved in outdoor business missed their treatment. This suggests that the busy nature of those involved in business rendered them more likely to miss their treatment. The findings also revealed that ARVs were not always available for patients at the treatment center as only 78.4% of patients received their drugs whenever they went for drug refill. This has been confirmed by Eboko [16]. If drugs are not always available, adequate adherence of > 90% cannot be attained and so resistance to ARVs may likely develop. This has been confirmed by Mills and colleagues [2] who showed that HIV can develop mutations if adherence is not kept above 90%. Other studies [3, 17- 19] have showed that some of these factors were demonstrated to be associated with missing treatment and consequently poor adherence.
This study demonstrated that patients showed a significant level of acceptance of the cellphone SMSs strategy for their treatment and care. It revealed that 57% of patients who received the messages actually expressed the wish for the strategy to continue. By implication, these messages, if well targeted, will serve as reminders to respect treatment time, drug refill appointments and other laboratory investigations which will increase adherence and improve on the quality of care.
Looking at the effects of SMSs, results revealed that 28 (62.22%) of patients were able to take their treatment regularly and on time while 15.56% of the patients were actually reminded of their appointment day for drug refill. These findings are in conformity with the study carried out in Uganda by Chang and colleagues [20]. Other findings have also demonstrated that SMSs have a modifying effect on some of the drug related practices by patients [21, 22]. Of the 12 patients who were initially on traditional medication alongside ARVs, 7(58.3%) abandoned it after the intervention. Information self-reported by patients showed that SMSs sent to them, were successful in dissuading patients from taking traditional medication alongside ARVs.
The study is important because it improved adherence to ARVs and revealed some factors that contributed to non-adherence which, if targeted through SMSs, will continue to increase adherence and consequently reduce treatment failure, hence, improving the quality of life of HIV and AIDS patients.
CONCLUSION
With a constant struggle to improve on the quality of care, innovative approaches such as the use of cellphone SMSs for the care of people living with HIV and AIDS (adherence in intervention = 64.4% while adherence in control group = 44.2%) would motivate patients to be more involved and committed to their treatment and care.
Despite the efforts by the health system to provide quality treatment and care, and reduce treatment failure, there are a number of individual, system and environmental factors that impinge on adherence to ARV treatment. These factors which included forgetfulness, unavailability of ARVs, busy work schedule, and travelling without drugs, need to be addressed at the level of all treatment centers to ensure good adherence.
The use of cellphone SMSs in the care of people living with HIV and AIDS is a strategy that is accepted by patients, given that it is non-invasive. However, it will be cost effective to institute this strategy on a large scale.
AUTHORS’ CONTRIBUTIONS
NDS designed the study, oversaw data collection and supervised the work, participated in data analysis, drafted the manuscript and substantially revised it for academic content; LI conducted the study, performed the analysis and drafted the manuscript; NFP oversaw data collection and supervised the work and substantially revised the manuscript for academic content. JCNA and TEA participated in data collection, drafted the manuscript and substantially revised it for academic content. All authors read and approved the final copy of the manuscript.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
We heartily thank all the participants who gave their consent and participated in the study. We extend our sincere appreciations to the Director of the CBC Health Board for permitting us use their facility. We thank all the nurses and care givers of the Nkwen Baptist Health Center for their full co-operation in data collection. This is part of the work of the Masters in Public Health in field epidemiology that was successfully defended by Mr. Lange Innocent in 2012 at the Department of Public Health and Hygiene of the University of Buea.

