All published articles of this journal are available on ScienceDirect.

The Development and Implementation of an Outreach Program to Identify Acute and Recent HIV Infections in New York City
Authors Info & Affiliations
Abstract
Introduction: Since 2004, the authors have been operating First Call NYU, an outreach program to identify acute and recent HIV infections, also called primary HIV infections, among targeted at-risk communities in the New York City (NYC) metropolitan area.
Materials and Methodology: First Call NYU employed mass media advertising campaigns, outreach to healthcare providers in NYC, and Internet-based efforts including search engine optimization (SEO) and Internet-based advertising to achieve these goals.
Results: Between October 2004 and October 2008, 571 individuals were screened through this program, leading to 446 unique, in-person screening visits. 47 primary HIV infections, including 14 acute and 33 recent HIV infections, were identified.
Discussion: Internet and traditional recruitment methods can be used to increase self-referrals for screening following possible exposure to HIV.
Conclusion: Community education of at-risk groups, with the goal of increased self-diagnosis of possible acute HIV infection, may be a useful addition to traditional efforts to identify such individuals.
INTRODUCTION
Substantial barriers have hindered efforts to identify persons with acute HIV infection. The flu-like symptoms associated with this syndrome are non-specific, and acute HIV infection is often misdiagnosed [1]. Additionally, there are barriers to discussion of patients’ sexual history in clinical settings [2-4]. Finally, lack of knowledge among at-risk individuals about the signs and symptoms of acute HIV infection reduces the likelihood that individuals will seek care while symptomatic [1, 5].
Most efforts to educate the public have promoted ELISA testing with western blot confirmation despite the up to 3 month “window period” before these tests accurately detect HIV infection [6]. Even if aware of the symptoms of an acute HIV infection, people may not know about other methods of testing, where to seek them out, and the cost of such tests may be prohibitive.
Acute HIV infection has been shown to be an important driver of HIV transmission, in part because of high levels of viremia prior to the development of a full anti-HIV immune response [7-9]. Recent HIV infection also may be an important driver of HIV transmission [7]. Due to the substantial barriers described, acutely and recently HIV-infected individuals may engage in high-risk behaviors unaware of their HIV status [10-12].
We received funding from the National Institutes of Health in 2004 to study the immunology and pathogenesis of acute and recent HIV infection, collectively referred to as primary HIV infection (PHIV). Recruitment was accomplished by educating at-risk communities about the signs and symptoms of acute HIV infection as well as instructing those with recent risk to self-refer for HIV testing. Diverse at-risk communities were engaged by multiple means to raise awareness of the signs and symptoms of acute HIV infection and to highlight the importance of early detection. Our recruitment strategy was multi-staged and depended in part on modern marketing techniques. New York City (NYC) has a very diverse and disparate population, and at-risk communities are similarly diverse and disparate. Capturing the attention of potential volunteers can be challenging in a city with a saturated media market [13]. This publication reports on our recruitment strategies, marketed under the title “First Call NYU,” for identifying persons with acute and recent HIV infections. The knowledge we gained on the use of advertising media may be of value to epidemiologists developing their own recruitment strategies for studies of HIV or other diseases.
MATERIALS AND METHODOLOGY
The study and all recruitment materials and activities were approved by the relevant Institutional Review Boards (IRBs). The project offered testing to volunteers in the New York metropolitan area, including NYC, Long Island, northern New Jersey and southern Connecticut, who reported high-risk exposure(s) to HIV in the prior 90 days. A high-risk exposure for this project was defined as any of the following activities with an HIV-positive partner or partner of unknown HIV status: unprotected anal or vaginal intercourse, performing oral sex on a male partner to ejaculation, or sharing needles or syringes. Testing offered through this program was presented to the public as distinct from routine HIV testing, i.e. testing in the absence of a recent high-risk exposure. Volunteers seeking routine testing were referred elsewhere.
Potential volunteers called a dedicated telephone number to complete a risk assessment with a trained HIV counselor. Telephone calls received outside the hours of 7:00 AM – 8:00 PM were returned within 24 hours. Telephone screenings were semi-structured, allowing counselors to not only disseminate information about the signs and symptoms of acute HIV infection, but also to address volunteers’ specific concerns. Interviewers entered data into an interactive, computerized database while simultaneously conducting the telephone screenings. This method of data collection allowed for weekly analysis of recruitment efforts. Once a recent high-risk exposure to HIV was established, we collected a history of symptoms and made an appointment for in-person testing, interview and counseling.
Volunteers presenting for their initial clinic visit completed written informed consent for study screening and a New York State-approved consent for HIV testing. Volunteers were then offered rapid HIV 1/2 antibody screening and plasma HIV ribonucleic acid (RNA) viral load testing to detect acute HIV infection, along with HIV pre- and post-test counseling and risk-reduction counseling. Preliminary positive results from a rapid enzyme-linked immunosorbent assay (ELISA) were confirmed by western blot.
We defined persons with acute HIV infection to be those with an HIV viral load ≥2,000 copies/ml and either (1) a negative HIV ELISA, (2) a positive HIV ELISA and a negative or indeterminate western blot, or (3) a positive HIV ELISA and positive western blot but a documented negative HIV ELISA in the prior 30 days.
We defined those with recent HIV infection by use of the serologic testing algorithm for recent HIV-seroconversion (STARHS). STARHS identifies persons with recent HIV infection as those in whom the standard HIV ELISA and western blot are positive, but a less-sensitive ELISA is negative. In the present analyses, STARHS was calibrated so that recent HIV infections were estimated to have been initially infected sometime in the previous 129 days [7].
Volunteers identified with acute or recent HIV infection were offered enrollment in the clinical trials associated with the PHIV study. Volunteers ineligible for the PHIV study were offered enrollment in other clinical trials being conducted at NYU Langone Medical Center or were referred to other institutions. Appropriate referrals were made for volunteers needing treatment for sexually transmitted infections, mental healthcare and primary care.
Recruitment efforts for the PHIV study were conducted under the name “First Call NYU.” The name of the project was chosen not only for easy identification but to suggest an action step to potential volunteers that the project was “the first place to call” for concerns about HIV infection. From the beginning of the project, “branding” was employed, similar to the process used in private industry to raise visibility of a company or product. Branding was achieved through the use of consistent fonts, design, imagery and language, including memorable taglines, in all recruitment materials [14, 15].
Multiple full-color photographic advertisements, flyers with tear-off stubs, and double-sided palm cards were developed to target at-risk communities such as men who have sex with men (MSM), male-to-female (MTF) transgendered individuals, and women of racial or ethnic minorities. An additional target audience was the “leather community,” a subgroup of MSM who engage in sadomasochistic sexual practices and those individuals who dress in leather as a sexual fetish. High-profile members of the gay community, such as photographers and artists, collaborated with us to create the visual content of some advertisements.
Recruitment materials presented the signs and symptoms of acute HIV infection to facilitate self-diagnosis and were intended to educate the community and raise awareness. All content used in advertisements, including taglines, was developed by study staff who had frequent contact with volunteers. Language was tailored to be community-appropriate. Taglines included, “Are you sure it’s the flu?” and “Did you get more than just his phone number?” Study staff selected the models to appear in the advertisements and made an effort to include models of various races and ethnicities to reflect targeted populations, and staff collaborated with an outside designer for the graphic design of the materials.
Print Advertisements
From program inception through the present, a period of approximately 4 years, 55 print advertisements appeared in lesbian, gay, bisexual, and transgender (LGBT) magazines and newspapers, and in newspapers serving minority immigrant communities. The appearance of print advertisements was timed to coincide with important community events in NYC, such as gay pride events and other events attended by MSM, leather community expositions, and World AIDS Day.
Posters and Palm Cards
Approximately 11,000 posters with tear-off stubs and 100,000 palm cards were distributed in NYC, targeting neighborhoods with historically high concentrations of MSM and ethnic or racial minorities. With the support of local business owners, posters were prominently displayed in such locations as bathhouses catering to MSM, bars and clubs, convenience stores, laundromats, community centers, beauty salons, and other community gathering points. Palm cards were distributed alone and in “condom packs,” small plastic bags containing 2 condoms and a packet of personal lubricant. These “condom packs” were readily available in bars and clubs, and distributed at community and LGBT-lifestyle events.
Examples of printed recruitment materials may be viewed at: http://www.hivinfosource.org/firstcallarticle.
Outreach Events
Study staff attended community events to distribute recruitment materials, answer questions about acute HIV infection, collect contact information from potential volunteers, and distribute condom packs. Recruitment materials were selected to be venue- and event-appropriate in collaboration with event organizers and venue managers.
In addition to recruiting at bars and clubs, study staff attended leather community expositions and bathhouses catering to MSM. Through partnering with venue management, study staff was able to access at-risk communities that are typically considered difficult to reach. A description of research conducted at NYC bathhouses can be found elsewhere [16, 17].
Study staff conducted outreach at approximately 30 community events. Information about First Call NYU was distributed at 2 NYC bathhouses on a weekly basis concurrent with on-going research from February 2006 to April 2007 [17].
Internet Recruitment
Study staff used the Internet as a recruitment tool in an effort to reach other MSM sub-communities. Web banners were placed on websites on which MSM meet sex partners, or “hook-up” websites. A First Call NYU profile also was created on each of these websites that presented information about the study and signs and symptoms of acute HIV infection. These profiles appeared in search results when users searched for potential sex partners. Since program inception, web banners have appeared on 4 “hook-up” websites, and user profiles were actively monitored on 2 of those sites. Study staff also answered questions via email and in real-time by one-on-one instant messaging with potential volunteers using these sites.
To facilitate recruitment, our institution’s HIV research-related website (http://www.hivinfosource.org/firstcallnyu) was redesigned in December 2006. The redesign was guided by principles of search engine optimization (SEO). SEO boosts user traffic from web searches and increases the likelihood that a website will appear on the first page of search results when a web user searches for related terms. SEO principles also were used to target Internet users geographically located in NYC. The result of these efforts was 12,533 unique visits to the First Call NYU webpage from February 2007 to October 2008 (19 months). Data describing visitors to the programs website prior to February 2007 were unavailable due to an internal server error.
An Internet-based advertising campaign was launched for First Call NYU in October 2007 in collaboration with a firm that runs a widely-used Internet search engine. Advertisements, paid for on a per-click basis, appeared in the right-hand column of pages displaying search results and on contracted websites with content relevant to our target communities. Clicking on an advertisement would bring the user to our webpage. Advertisements appeared when users searched for keywords related to the signs and symptoms of primary HIV infection, such as HIV testing, sexually transmitted infections, HIV risk-related terms such as condom break, post-exposure prophylaxis (PEP), and inconclusive HIV test results. Keywords were chosen by study staff based on their relevance to the at-risk communities and incorporated colloquial terms used for the aforementioned keywords to better target laypeople. Common misspellings of keywords were also included to maximize the possibility of reaching all potential volunteers. Negative keywords were identified and used to avoid presenting advertisements to users who were searching for things other than HIV, such as other viral illnesses. Between October 2007 and October 2008, the First Call NYU advertisements appeared 179,934 times along side search results, and were clicked on 4,601 times by search engine users. The total cost of the Internet advertising campaign during this period was $2,065.72, with an average cost-per-click of $0.42.
Outreach to Service Providers
Healthcare providers serving at-risk communities were contacted to create a bi-directional referral network. Study staff contacted physicians in private practice, hospital clinics, community-based organizations, and methadone maintenance treatment programs. In-service education programs were conducted for providers and their staff, with special efforts made to include support staff. Service providers also were asked to display program materials in waiting rooms and other common spaces.
Since study inception, 133 healthcare providers were contacted, and 11 of these providers requested recruitment materials. In-service education programs were conducted for 10 of the 133 providers originally contacted.
A summary of recruitment efforts over time is presented in Table 1.
Recruitment Methods, Yield, and Total Costs (US Dollars) of First Call NYU, New York City, USA, October 2004 –October 2008
| Recruitment Method | Yield (Number of Telephone Calls Received) | % of All Telephone Calls Received | Cost Incurred |
|---|---|---|---|
| Print Advertisement1 | 95 | 21.3% | $51,738 |
| Word-of-Mouth | 97 | 21.7% | 0 |
| Internet Search2 | 53 | 11.9% | $2,066 |
| Referral Network of Healthcare Providers, CBOs and MMTPs3 | 52 | 11.7% | $3,123 |
| Other Websites4 | 23 | 5.2% | $496 |
| Previous Study Volunteers | 22 | 4.9% | 0 |
| Bathhouse5 | 20 | 4.5% | $1,790 |
| “Hook-up” Websites6 | 21 | 4.7% | 0 |
| Passive Recruitment (flyers, condom packs, and palm cards)7 | 7 | 1.6% | $10,471 |
| Outreach Events | 5 | 1.1% | $14,503 |
| Unknown | 51 | 11.4% | - |
| Total | 446 | 100.0% | $84,187 |
1 Costs associated with design of print advertisements and placements of advertisements.
2 Costs associated with Internet PPC campaign.
3 Costs associated with the production and design of physical materials distributed to providers.
4 Costs associated with design of web banners, not placement of banners.
5 Costs associated with the production and design of physical materials distributed at bathhouses.
6 Costs associated with design of web banners, not placement of banners. Banner placement was donated in-kind by the operators of the websites.
7 Costs associated with physical materials other than condoms. Condoms were provided free of charge by the NYC Department of Health and Mental Hygiene.
Numbers of Acute and Recent HIV Infections Identified by First Call NYU by Recruitment Method and Results, NewYork City, USA, October 2004 – October 2008
| Recruitment Methods | Number of Acute HIV Infections Identified (% of Total Acute Infections) | Number of Recent HIV Infections Identified (% of Total Recent Infections) | Total Acute and Recent HIV Infections Identified (% of Total) |
|---|---|---|---|
| Print Advertisement1 | 2 (14.3%) | 3 (9.1%) | 5 (10.6%) |
| Word-of-Mouth | 4 (28.6%) | 7 (21.2%) | 11 (23.4%) |
| Internet Search2 | 0 (0) | 1 (3.0%) | 1 (2.1%) |
| Referral Network of Healthcare Providers, CBOs and MMTPs3 | 4 (28.6%) | 15 (45.5%) | 19 (40.4%) |
| Other Websites4 | 1 (7.1%) | 1 (3.0%) | 2 (4.3%) |
| Previous Study Volunteers | 2 (14.3%) | 1 (3.0%) | 3 (6.4%) |
| Bathhouse5 | 0 (0) | 0 (0) | 0 (0) |
| “Hook-up” Websites6 | 0 (0) | 0 (0) | 0 (0) |
| Passive Recruitment (flyers, condom packs, and palm cards)7 | 1 (7.1%) | 0 (0) | 1 (2.1%) |
| Outreach Events | 0 (0) | 1 (3.0%) | 1 (2.1%) |
| Unknown | 0 (0) | 4 (12.1%) | 4 (8.5%) |
| Total | 14 (100%) | 33 (99.9%) | 47 (99.9%) |
| Total cost per Acute | $6,013 | Total cost per Acute or Recent | $1,791 |
1 Includes design of advertisements in printed media.
2 Costs of Internet-based advertising campaign.
3 Costs associated with the production and design of physical materials distributed to providers.
4 Includes costs of design of web banners, not placement of banners.
5 Includes costs associated with the production and design of physical materials distributed at bathhouses.
6 Costs associated with design of web banners, not placement of banners. Banner placement was donated in-kind by the operators of the websites.
7 Costs associated with physical materials other than condoms. Condoms were provided free of charge by the NYC Department of Health and Mental Hygiene.
RESULTS
Between October 2004 and October 2008, 571 individuals completed a telephone screening to determine eligibility for the program. Of the total number of volunteers who completed a telephone screening, 497 tests were performed on 446 unique volunteers. The percentage of telephone screenings to completed in-person testing sessions was 89.7%. Not all volunteers who were tested completed a telephone screening. A summary of recruitment efforts and numbers of calls to the study telephone number over time is presented in Fig. (1).
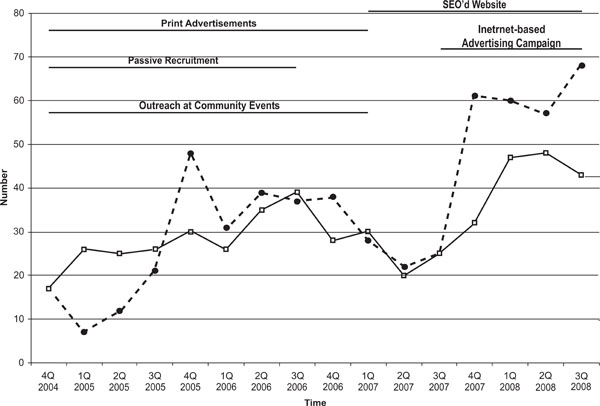
Number of unique callers to the dedicated First Call NYU phone line (dotted line) and unique in-person screening visits conducted by First Call NYU study staff (solid line) by calendar quarter, New York City, NY, October 2004 through October 2008. Time intervals of various methods of recruitment employed are also plotted.
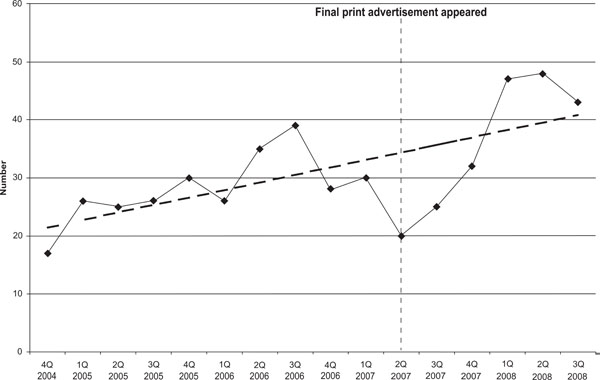
Number of unique volunteers screened by First Call NYU study staff by calendar quarter, New York City, NY, October 2004 through October 2008. A fitted trend line is also plotted.
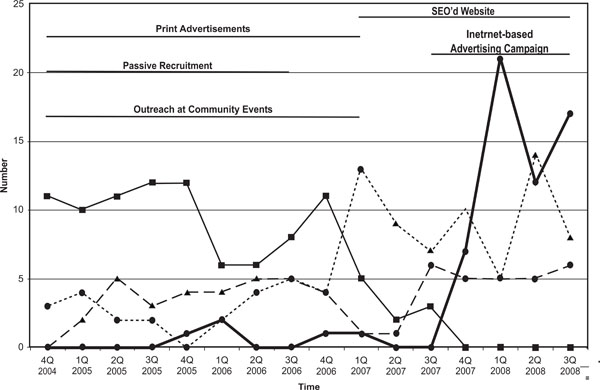
Number of unique volunteers seen through First Call NYU in New York City by 4 most successful recruitment methods -- Internet Search (heavy black line), Word-of-Mouth (broken line), Print Advertisements (thin black line) and Provider Referrals (dotted line) – by calendar quarter, New York City, NY, October 2004 through October 2008. Time intervals of various methods of recruitment employed are also plotted.
The most effective methods of recruitment (Table 1) were word-of-mouth (21.7%), print advertisements (21.3%), Internet search engines leading users to the program’s webpage (11.9%), and healthcare provider referrals (11.7%). As described in Table 2, the efforts that identified the most acute and recently infected volunteers were Referral Network of Healthcare Providers (40.4%), word-of-mouth (23.4%), print advertisements (10.6%) and volunteers of unknown referral source (8.5%). Many study volunteers reported seeing advertisements in multiple places or mediums before calling to screen for First Call NYU. This anecdotal finding suggests that multiple, diverse recruitment pathways had a synergistic effect and extended the reach of recruitment messages. We unfortunately did not collect data that could allow verification of this impression.
The total cost of recruitment efforts, excluding staff time, was $84,187 over four years (Table 1). The costs reported for print advertisements, referral network, passive recruitment and outreach events include “hidden costs,” such as graphic design and production of materials. Costs associated with print advertisements, outreach events and passive recruitment were likely higher than would be incurred in many other regions of the USA due to the generally higher advertising costs in NYC. The costs associated with Internet searches, which include SEO, Internet advertisements, and web banners would not be expected to vary substantially among geographic areas. Excluding staff time, the total cost per acute infection identified (n=14) was $6,013 and the cost per acute or recent infection identified (n=47) was $1,791.
2.1 – 2.25 full time employees (FTEs) were utilized throughout First Call NYU. Study staff included study coordinators, research nurses, outreach coordinators, data managers, and trained HIV tester/counselors. Total staffing costs ranged from $80,750 to $85,250 per year. Including staff time, the total cost per acute infection identified (n=14) was $11,942 and the cost per acute or recent infection identified (n=47) was $3,557. Not included in the staffing estimates were the time of the faculty-level investigators or the study physicians, although these individuals provided guidance to the recruitment efforts, occasionally gave talks at public or professional forums to increase recruitment, and provided patient care following identification of HIV infections.
14.8% (n=74) of all tests performed were found to be positive for HIV, including 2.9% (n=14) that were identified during acute HIV infection and 6.9% (n=33) that were not acute but were identified within 129 days of HIV infection as determined by STARHS.
As seen in Figs. (1, 2), volunteer response continued to increase even after print advertisement and community outreach ceased. Print advertisements continued to yield eligible volunteers for approximately 1 year after the last appearance of an advertisement (Fig. 3). Following the discontinuation of print advertisements, recruitments attributed to “word-of-mouth” rose, resulting in a steady stream of responses.
DISCUSSION
First Call NYU advertising aimed to prompt potential volunteers to self-refer for diagnosis of acute or recent HIV infection. The combination of print, Internet and community outreach resulted in identification of 14 acute and 33 recent HIV infections over a four-year period. The 2.8% yield of acute infections per HIV test performed by this program was 133 times the 0.02% yield obtained by Pilcher et al., who tested 109,250 persons in North Carolina over a 12 month period to identify 23 acute HIV infections [18]. Priddy et al., who tested 2,202 individuals over a 14 month period to identify 26 recent HIV infections, including 4 acute infections, incurred lower costs per patient identified than First Call NYU, but utilized a universal screening methodology and did not notify individuals in real-time [19]. The NYC Department of Health and Mental Hygiene performed pooled PCR testing on approximately 21,000 specimens collected between July and December 2008, yielding 17 acute infections [20]. While these programs occurred over different periods of time, and one occurred in the context of a lower community-wide HIV prevalence, our relatively high yield suggests that there is a place for targeted screening of at-risk communities.
The success of this program did not appear to be the result of any single method of recruitment. Methods evolved over time based on an understanding of the cumulative effects of recruitment strategies and weekly monitoring of recruitment numbers. Anecdotal reports from study volunteers suggested that multiple, concurrent methods of recruitment worked synergistically. It is possible that various methods reinforced and amplified each other as potentially demonstrated by the high number of volunteers recruited by word-of-mouth. Future research should include measurement of these possible effects.
Community rapport and branding of the First Call NYU name was established using consistent imagery and language and by collaborating with diverse partners. Although some of the methods of recruitment employed were not as directly effective as others, the presence of First Call NYU in the targeted communities furthered market saturation. For example, as seen in Fig. (3), print advertisements continued to yield eligible volunteers for approximately 1 year after the last appearance of an advertisement. Furthermore, it may have been that the cumulative effect of all methods that yielded a constant stream of eligible volunteers. Future research should explicitly measure these potential effects of recruitment.
Provider referral was an important and cost-effective method of recruiting acute and recently HIV-infected volunteers. However, solely relying upon this method of recruitment would have yielded fewer cases identified (n=19) than achieved through multiple methods (n=47). It is important to note that other investigators have used only provider referrals to recruit volunteers, which may have limited enrollment in their research studies [20-33]. Thus, provider referral is an important component for the identification of this population that can be supplemented with additional, diverse recruitment efforts.
In total, 76.9% (n=343) of volunteers seen in person and 51.1% (n=24) of those identified with acute or recent HIV infection self-referred to the program. These data demonstrate that with appropriate prompting and community education, members of at-risk communities can be empowered to self-refer for testing while in the acute or recent periods of HIV disease.
Internet recruitment contributed to the dissemination of study messages. Future efforts should initiate SEO and Internet advertising campaigns at the beginning of recruitment. These methods may benefit from a longer period of use to fully optimize their potential. While Internet-based efforts appear to be useful for recruitment, the duration of impact of such efforts is unknown and requires further research. It is important to note that Internet methods are evolving rapidly and need to be monitored by the practicing epidemiologist to obtain the maximum benefit from these methods.
Although the cost per acute infection identified was higher than other reported screening efforts [34], these costs may have been influenced by the higher costs of advertisement and staffing associated with NYC. First Call NYU continues to identify acute infections, and it is possible that costs per acute identified may be lower at program conclusion. Schackman et al. in 2006 estimated that the lifetime undiscounted costs of treatment of HIV in the USA was $618,900 [35]. It is impossible to determine the number of secondary infections that were prevented by the identification of acute and recent infections in this program, but the costs associated with identifying these acutely and recently infected persons are modest compared to lifetime costs of treatment.
Persons with acute and recent HIV infection are critical for understanding of HIV pathogenesis, preventing secondary HIV infections, thus decreasing the tempo of the HIV epidemic [36]. Furthermore, if future research demonstrates a substantial clinical benefit from initiation of antiretroviral therapy very early in infection, epidemiologists will have an obligation to devise and apply multiple methods such as those described in order to identify individuals with acute and recent HIV infection [21, 24, 25, 27-30, 37].
CONCLUSION
The multi-method recruitment strategy described may be effective for recruiting acute and recent HIV infections in other at-risk groups or geographic locations. Future research should be conducted to evaluate the efficacy and feasibility of these strategies in other locations, with other at-risk communities, and in the study of other diseases.
CONFLICT OF INTEREST
There have been no involvements that might raise the question of bias in the work reported or in the conclusions, implications, or opinions stated.
ACKNOWLEDGEMENTS
This work was supported in part by grant AI057127 and Center for AIDS Research grant AI027742 from the National Institute on Allergy and Infectious Diseases, National Institutes of Health, to the New York University School of Medicine. The authors would like to thank Bellevue Hospital Center and the NYU/Bellevue AIDS Clinical Trials Unit Community Advisory Board for assistance with this research.

