All published articles of this journal are available on ScienceDirect.

Improving the Risk of Treatment Failure in Antiretroviral Treatment: Support Group Attendance in the Post-COVID-19 Pandemic in Western Cape, South Africa — A Quality Improvement Approach
Authors Info & Affiliations
Abstract
Introduction
This study aimed to improve the attendance of people living with HIV (PLHIV) in the Risk of Treatment Failure (ROTF) support group via quality improvement initiatives at Delft Community Health Center, Western Cape, in South Africa.
Methods
A quality improvement approach (QI) was employed. The “five whys framework” was used to identify the root cause of low attendance of PLHIV in the ROTF support group. Plan–do–study–act (PDSA) cycles were conducted, and measures were set to monitor project outcomes. The project started with a baseline analysis with stakeholders to identify root causes and drivers of change. We implemented the required changes with continuous engagement of QI teams and PLHIV members.
Results
The number of PLHIV attendees in the ROTF support group increased with the implementation of the QI intervention, from non-attendance at baseline to improved attendance over subsequent months. One month after the QI intervention started in April 2023, 30% of the participants (3) attended the ROTF support group, and the number increased to five (100%) in the next month. It increased to thirteen in June 2023 (100%), and 19 attended the ROTF support group meeting in the final session. Three ROTF support group members attained the required VL suppression levels and graduated from the program.
Discussion
This QI project shows that structured, low-cost QI approaches can substantially improve attendance of people living with HIV in ROTF adherence support groups. Using the five whys framework to identify root causes and iterative PDSA cycles to address them led to improvements in participation, increasing from non-attendance at baseline to improved attendance within three months. Enhanced engagement was accompanied by meaningful clinical gains, including viral load suppression and graduation of three participants from the programme. These findings highlight the effectiveness of simple QI methods in strengthening adherence support and improving outcomes in resource-constrained primary healthcare settings when patient engagement, frontline involvement, and leadership support are prioritized. As a limitation, the study's small sample size and short study period make it difficult to ascertain clinical outcomes. Continuous quality improvement, scaled up with a larger sample size, could help to better ascertain clinical outcomes.
Conclusion
This study highlights the use of quality improvement approaches that improved PLHIV attendance in the ROTF adherence support group. Health and health outcomes can improve even in resource-constrained settings by optimally allocating available resources and adapting and adopting simple measures. The attendance of PLHIV in the ROTF adherence support group improved with the use of QI practices. Training in QI concepts and principles, as well as project implementation, is recommended to ensure QI sustainability through a robust methodology, skilled support structures, prioritization, and leadership involvement.
1. INTRODUCTION
South Africa has a high human immunodeficiency virus (HIV) burden, with the largest number of people living with HIV (PLHIV) and antiretroviral therapy (ART) programs worldwide. The highest number of HIV cases was reported in 2021 among sub-Saharan African (SSA) countries [1, 2]. South Africa, as a member of the United Nations, has endorsed the 95–95–95 strategies urging countries to provide effective HIV prevention options, ensuring that 95% of people living with HIV know their HIV status, 95% of people who know their status receive HIV treatment, and 95% of people on treatment are virally suppressed, accelerating the UNAIDS Fast-Track strategy [3]. The strategy is further linked to the goal of eradicating acquired immunodeficiency syndrome (AIDS) by 2030 and expediting the achievement of the Sustainable Development Goals (SDGs), particularly Goal 3, which aims to achieve good health and well-being [3].
Progress has been made in controlling the HIV epidemic, particularly in improving testing and treatment and reducing its incidence [2]. Despite having a high HIV prevalence, South Africa has made great progress in meeting the UNAIDS 95-95-95 targets. Among pregnant women, for example, 97.6% were aware that they were HIV positive, 96% were on ART, and 66% of ART-using women achieved viral load suppression in 2019 [4]. However, strengthening adherence counselling and support groups is needed to achieve viral suppression [4]. ART adherence is crucial for HIV prevention, as it effectively prevents transmission, which is commonly referred to as U=U (undetectable equals untransmittable) [5, 6]. Although high ART adherence levels have been recorded nationally in South Africa [7], poor adherence persists in some settings. For example, adherence performance varies significantly, with some reports indicating non-adherence rates of over 50%, and young individuals consistently demonstrating the lowest adherence levels. Some contributors to poor ART adherence include alcohol use, treatment fatigue, and stigmatization; in addition, waiting times, staff shortages, and negative attitudes have also been identified as contributors to suboptimal adherence [8, 9].
To address non-adherence challenges, the government initiated a comprehensive plan of action through the South African National Department of Health (NDoH), including several measures to strengthen linkages in the HIV care cascade [10]. Psychosocial support in the form of support groups has been recommended by the World Health Organization (WHO), the Joint United Nations Programme on HIV/AIDS (UNAIDS), and other evidence sources as a critical strategy for enhancing HIV care for decades [11]. However, HIV support groups face challenges such as stigma, limited resources, and gender disparities in participation, which can hinder their effectiveness in improving health outcomes for people living with HIV [12].
During ART adherence support sessions, those identified as at risk of non-adherence come together to share challenges and experiences of living with the virus without being judged, blamed, stigmatized, or isolated [13]. Such support groups have been shown to be effective in reducing mortality and morbidity, increasing adherence to care, and improving quality of life [11, 14, 15]. The ROTF support group is an example of such a support group, primarily bringing patients with elevated viral loads (VL) together for enhanced counselling and peer support [16].
Since 2015, the Delft Community Health Centre has provided ROTF support group services to PLHIV, which were disrupted by the COVID-19 pandemic, similar to many health sector services [17, 18]. Before the COVID-19 pandemic, between six and ten ROTF support group members congregated per session. However, after the emergence of the pandemic until the end of 2022, zero to three members were recorded per session. Therefore, the team embarked on a QI project to address this gap and improve the attendance and utilization of this vital support group structure. The QI project aimed to improve the attendance of PLHIV in the ROTF support group.
2. METHODS
2.1. Study Design
A quality improvement (QI) approach using the Five Whys framework and the PDSA cycle was employed to improve attendance at the ROTF support group, which was the main outcome measure. The ROTF individuals were defined as PLHIV who did not achieve a <50 c/mL laboratory viral load test while on ART, as they are at risk of ART failure [19]. Quality improvement projects, such as clinical research, have been shown to provide evidence on which to base interventions and improve patients' lives through the implementation of QI interventions [20].
The QI methodology uses a cycle approach that involves (a) identification of gaps in service delivery and root causes using identified QI tools, (b) development and implementation of QI change ideas via specified QI tools, and (c) process evaluation of the tested change ideas [21]. QI intervention starts with identifying gaps and causes using available QI tools such as process mapping, root cause analysis, Five Whys, fishbone diagrams, and others [22]. Then, possible solutions are identified in line with the root causes, leading to the development of a quality improvement plan (QIP). The plan is then implemented over time while monitoring the interventions via identified indicators; in this case, improving PLHIV attendance at the ROTF support group was implemented. Documenting and disseminating QI initiative outcomes is critical to ensure that others learn from the exercise. The QI process was followed to improve attendance at the ROTF support group in Delft Community Health Centre, Cape Town, Western Cape (Fig. 1).
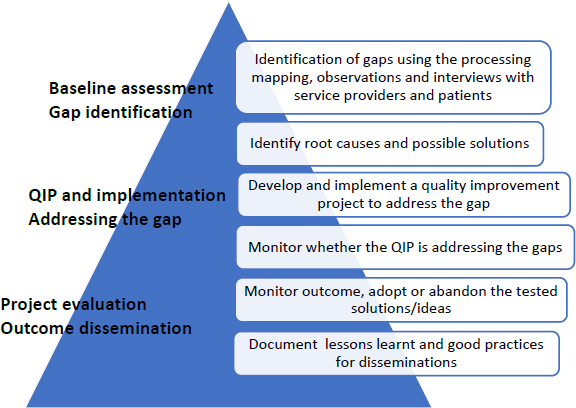
Quality improvement process applied to improve attendance in the ROFT support group at the Delft Community Health Center, Cape Town, Western Cape [21].
2.2. Study Site
The study was conducted at Delft Community Health Centre, Tygerberg Health subdistrict in Cape Town, South Africa, which serves the Delft informal settlement with a population of 152,030 people, of whom 7,640 patients were on the ART program.
2.3. The Process of Establishing a QIP Team
We used a quality improvement approach to revive the ROTF support group, which stopped during the COVID-19 pandemic. The QIP team was established and comprises the facility manager, the person in charge of the infectious disease unit (IDU), the administrator, and a representative from the support group. The QIP team members were trained in quality improvement approaches, including QI concepts.
2.3.1. Gap Identification and Root Cause Analysis
The QIP team identified the challenge of PLHIV’s poor attendance at the ROTF support group as a specific, measurable, achievable, and relevant goal that could be achieved within 3 months. The QIP team applied the Five Whys framework [23] to identify the root causes of poor attendance at the ROTF support group in detail (Fig. 2).
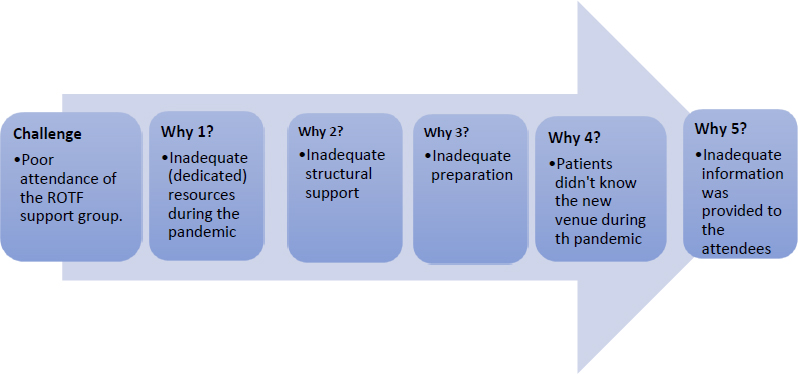
Root cause of poor attendance of the ROTF support group via “Five whys” root cause analysis, Delft Community Health Center, Cape Town [23].
The QI team conducted a Five Whys analysis and discussed the root causes of poor attendance at the ROTF support group. First, the COVID-19 pandemic depleted both human and physical resources, resulting in inadequate structural support, including the absence of dedicated staff and an appropriate space to run the sessions. This contributed to poor preparation for the meetings, and people living with HIV were not consistently aware of the session venue because this information was not consistently communicated.
2.3.2. Planned Quality Improvement Activities
The facility leader and QI team proposed solutions to address the root causes identified in the framework. These included obtaining a dedicated space for support groups, assigning a dedicated nurse to provide supervisory oversight to the convening counsellor, reserving a marked waiting area for ROTF patients before the commencement of support group meetings, and using a public address (PA) system to direct patients to their designated waiting area. These changes were tested via Plan–Do–Study–Act (PDSA) cycles.
2.4. Quality Improvement Measures
2.4.1. Outcome Measures
Improvement, defined as an increase in ROTF support group attendance, was the main outcome of the planned QI project, and the number of patients attending the sessions was the main outcome measure.
The QI change ideas and measures used to assess the process were observed as the improvement project was implemented. The parameters used to measure the QI activities were as follows: (1) announcements were made via a PA system in all facility waiting areas; (2) obtaining a marked dedicated space for a dedicated time; (3) assignment of a dedicated nurse to provide supervisory oversight to the convening counsellor; (4) sending mobile phone reminders to booked patients who would attend the ROTF support group; (5) preparing files and medication packages one day before the support group meeting; (6) dispensing files and pre-packaged medication to the convening counsellor one day before the support group meeting; and (7) peer shadowing conducted by experienced counsellors (Table 1).
| System changes and a change idea | Process measures and other process changes |
|---|---|
| 1. Announcements to be made using a PA system in all facility waiting areas | # of announcements |
| 2. Obtaining a clearly marked dedicated space for a dedicated time | Clearly marked, dedicated waiting area |
| 3. Identify a dedicated nurse to provide supervisory oversight to the convening | One dedicated nurse is assigned to oversee the ROTF support groups |
| 4. Sending mobile phone reminders to booked patients who will attend the ROTF support group | Number of reminders sent |
| 5. Preparing files and medication packages one day before the support group meeting | Number of files and medication packages prepared |
| 6. Dispensing of files and packaged medication to the convening counselor one day before the support group meeting | Number of files and medication packages dispensed to the counselor |
| 7. Peer shadowing of experienced counsellors | Number of peer shadowing events with experienced counsellors |
3. RESULTS
3.1. Description of Plan‒do‒study‒act (PDSA) Cycles
To improve attendance among PLHIV in the ROTF support group, QI activities were guided by the PDSA framework, with multiple PDSA cycles and system changes implemented. One of the PDSA cycles tested the use of a PA system, which aimed to enhance communication and engagement among PLHIV patients to improve attendance at the ROTF support group. The PA system announcement was planned for the waiting areas to inform ROTF patients about the support group.
The PA system announcement was discontinued after 2 weeks of use by health promoters and counsellors because clinicians began informing patients in consultation rooms and directing them to the designated waiting areas for ROTF. The study revealed that the PA system announcement stopped two weeks after the QI intervention, and a system change was observed (Fig. 3).
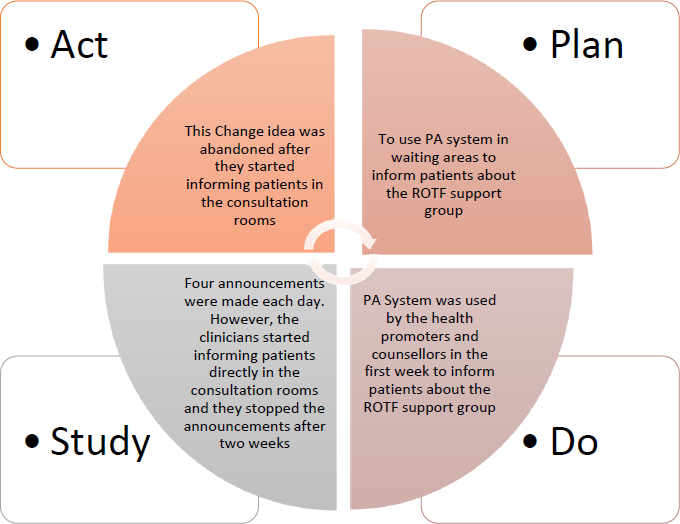
PDSA cycle for using the PA system for announcement to improve the attendance of the ROTF group, Delft Community Health Center, Cape Town, Western Cape.
3.1.1. System Changes and Testing Change Ideas
- System Changes: Secured a dedicated space and designated specific time slots for the intervention. Additionally, a nurse supervisor was identified to oversee the process.
- Change Idea 1: Tests the use of announcements via the PA system to enhance communication and engagement.
Multiple PDSA cycles and system changes were completed during this QI project. One of the PDSA cycles used was the PA system, which was intended to enhance communication and engagement among PLHIV, thereby improving attendance at the ROTF support group (Fig. 3).
The clearly marked sitting area was identified and reserved for ROTF patients, where they waited before the support group meeting commenced. Announcements were made using a public address (PA) system in all waiting areas of the facility to direct ROTF patients to their designated waiting area. A day before the session, counsellors sent mobile phone reminders to booked patients to attend support group meetings, and files and medication packages were prepared. The files and medication packages were dispensed to the convening counsellor a day before the meetings to ensure all preparations were completed on time. Experienced counsellors shadowed less experienced counsellors to transfer skills and knowledge.
3.2. The Facility Visits
Excluding the initial “meet and greet” facility visit, which took place on 24 April 2023, four other visits were undertaken during this project period. On this day, a QI team was established and oriented to the basic principles of QI. The QI team consisted of the IDU in charge, the oversight nurse, and the convening counsellor for the ROTF support group sessions. The team developed a QIP outlining activities, assigning responsible persons, and setting timelines. The facility manager briefed all facility staff on the QIP. The research team conducted visits on the days when ROTF support group members met and during PDSA cycle practice. The facility’s research and QI teams maintained constant communication via phone and in writing between facility visits.
Counsellors were reminded to send reminders to booked patients and to prepare patients’ files and medications at least one day before the support group meeting.
3.3. The First Facility Visits
Prior to this visit, the researcher contacted the facility manager to obtain approval and engage in the QI project. The first facility visit was conducted on 26 April 2023, and a QI project team, including a facility manager, an overseeing nurse, and a counsellor, was established. Training on QI concepts, principles, and methods was given to the QI team. The first visit was an observation visit to ensure the success of the project. A formal ROTF support session did not occur at the first visit because most expected patients with elevated VL did not turn up. Only 30% (three out of ten) of the invited participants attended at different times; therefore, a formal group session was not held. Instead, they were individually counselled. The QI project team developed a detailed plan of action, which was assigned to the responsible parties for execution before the next ROTF support group meeting.
3.4. The Second Facility Visit
This meeting was initially scheduled to be held on 23 May 2023, but, following the recommendation of one of the QI team members, it was postponed to 24 May 2023 to coincide with the patients’ clinic appointment date. However, 30% of PLHIV patients came on 23 May 2023, and they were individually counselled. Of the 10 patients booked from the previous month, only 30% attended on this day. Two new patients presented with elevated VL. A total of five PLHIV attended the meeting. The convening counsellor conducted the session with the champion nurse, who provided supervisory oversight.
3.5. The Third Facility Visit
The third meeting was conducted on 21 June 2023. Thirteen ROTF support group members attended this meeting. There were open, animated discussions on the use of garlic and “traditional” medicines alongside ARVs, barriers to and facilitators of treatment compliance, and how to address missed doses. Three baseline patients (seen on 26 April 2023) had blood samples drawn for VL assessment.
3.6. The Last Facility Visit
The fourth meeting was conducted on 19 July 2023. Nineteen ROTF support group members attended this meeting; group bonding and camaraderie were evident, and the conversation flowed easily among attendees and facilitators. All patients in attendance discussed treatment compliance and shared different ways they were mitigating barriers to it. The three baseline patients received blood test results, and all were virally suppressed, indicating adherence to their treatment regimens. These three members graduated from the ROTF support group.
At the end of the discussion, fruits and healthy snacks were provided to all attendees to encourage continued treatment compliance and ROTF support group attendance, and to help healthcare workers appreciate them (Fig. 4).
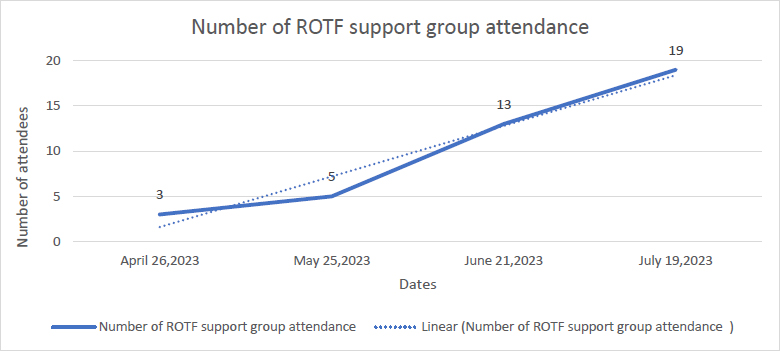
Number of ROTF support group attendance at Delft Community Health Center, Cape Town, Western Cape.
3.7. Outcome Measures
The main outcome measure for this QI project study was the increase in ROTF support group attendance following the implementation of planned interventions. There was no attendance at baseline for three months from January to March 2023. One month after the QI intervention started in April 2023, 30% of participants attended the ROTF support group (3 out of 10 ROTF patients booked), and the number increased to five (100%, five patients were booked) in the next month. It increased to thirteen in June 2023 (100% of booked patients), and in the final session, 19 attended the ROTF support group meeting, and three baseline patients graduated as they became virally suppressed.
3.8. System Changes, Process Changes, and Process Measures
The previously indicated system changes, process changes, and process measures were achieved to varying degrees. First, establishing a QI project team comprising the facility manager, oversight nurse, and counsellor was critical to getting the project off the ground. Training was provided to the QI team on QI concepts, principles, and methods. A dedicated space was obtained: a consulting room that later became too small as the number of attendees increased and was replaced with a larger room. The delegated nurse was assigned to coach counsellors during the sessions, and the use of a PA system was briefly implemented for two weeks but was later stopped, as directions and discussions provided by clinicians to patients were sufficient. Moreover, clear signage on the meeting room door provided accurate information and directions to ROTF support group attendees. The dedicated meeting room also served as the clearly marked waiting area.
4. DISCUSSION
Quality improvement approaches were used to address PLHIV’s poor attendance at an ROTF support group at the Delft Community Health Centre in the Western Cape. The quality improvement intervention highlighted the role of teamwork in addressing health system challenges related to poor attendance by PLHIV at the ROTF support group. The study highlighted the importance of raising awareness of available services and the need for a designated, dedicated space for support group meetings to increase attendance among PLHIV in ROTF support groups.
A team with clear roles and responsibilities is essential for quality improvement interventions. The study participants had clear roles and responsibilities, and the facility manager informed facility staff of the ongoing project. A passionate and enthusiastic team is important for the achievement of any QI project [20, 24]. The clinicians referred patients directly to the responsible counsellor to counsel them and recruit them into the support group. As a result of this teamwork, some of the planned activities, for example, the use of the PA system to provide information on the time, place, and duration of ROTF support group meetings, were no longer necessary, as the information provided by clinicians to patients was sufficient. Establishing a supportive QI team at the inception of any QI project is important for attaining the objectives [20, 24, 25].
The study highlighted the importance of raising awareness of available services to increase access after disruptions during the COVID-19 pandemic. COVID-19 disruptions affected access to ROTF support groups and numerous other services [17, 18]. This study highlights the need for orienting services for new patients at risk of ART non-adherence and unaware of the existence of ROTF support group sessions. The approaches used to raise awareness among prospective group members in this study maximized teamwork, whereby clinicians referred all at-risk patients to a counsellor for counselling and the subsequent appointment date in line with the support group meeting date. Raising awareness among prospective service users of available services has proven to be a key driver in improving access to and the quality of available health services [26, 27].
One root cause of the disruption of these support group sessions after the emergence of the COVID-19 pandemic was the lack of a dedicated and well-marked space for group members to meet due to resource constraints, a common QI project challenge [24]. In our case, the health facility had limited space, and the support group space was used for wellness services, as in many other resource-constrained settings. The facility manager, in discussion with the QI team, agreed and allocated space for the ROTF support group meetings. There is growing evidence of the importance of a safe physical and social space in promoting the uptake of health services, which is in line with what we found in our QI project [28]. The COVID-19 pandemic has left gaps in health systems that need to be addressed, and we propose quality improvement approaches to address these gaps [17, 18, 29].
The main outcome of this QI project was to increase the attendance of ROTF support group members at risk of being non-adherent to ART. The sustainability of quality improvement (QI) interventions should be ensured by continuously maintaining gains even after improvements have been made. To ensure continuity and sustainability, aligning the structures for implementing a quality improvement program (QIP) within the existing facility structures is crucial [30].
Training in QI concepts, principles, and project implementation is recommended to ensure QI sustainability through a robust methodology, skilled support structures, prioritization, and leadership involvement [30, 31]. Local solutions should be developed, documented, and shared according to the QI framework, with collaborative workshops facilitating dissemination to other facilities [21, 22, 31].
Even though three members became virally suppressed and were discharged or graduated after three months, the increase in viral load suppression reported in this study may not be attributed to the ROTF support group because there was insufficient time to demonstrate this effect, as at least a 6-month follow-up is required [32].
5. LIMITATIONS OF THE STUDY
Although we applied different quality improvement frameworks, including the Five Whys and the PDSA approach, the absence of a comparison group, the small number of participants, and the short study duration were limitations. This limits our ability to attribute changes in support group attendance and other outcomes solely to the intervention. The temporal associations observed between the intervention and the measured outcomes may instead reflect the influence of concurrent changes rather than being directly attributable to the Quality Improvement Project (QIP).
CONCLUSION
This study emphasizes the importance of quality improvement (QI) in addressing health system gaps caused by the COVID-19 pandemic. The implementation of service changes can be challenging; however, listening to and engaging service users is essential to overcoming these challenges [33]. This study also emphasizes the importance of teamwork in implementing QI projects and demonstrates that even in resource-constrained settings, improvements in health quality and outcomes can be achieved through optimal resource allocation and simple measures.
AUTHORS’ CONTRIBUTIONS
All the authors participated in the development and finalization of this paper. They were all involved in conceiving the topic and writing this paper. All the authors read and approved the final manuscript. J.N.: Guarantor of the manuscript.
LIST OF ABBREVIATIONS
| AIDS | = Acquired Immune Deficiency Syndrome |
| ART | = Antiretroviral Therapy |
| HIV | = HumaN Immunodeficiency Virus |
| NdoH | = National Department of Health |
| PDSA | = Plan‒do‒study‒act |
| PLHIv | = People Living with Human Immune Virus |
| QI | = Quality Improvement |
| ROTF | = Risk of Treatment Failure |
| SSA | = Sub-Saharan African |
| SDG | = Sustainable Development Goals |
| U=U | = Undetectable equals Untransmittable |
| UNAIds | = Joint United Nations Programme on hiv/aids |
| WHO | = World Health Organization |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethics approval to conduct this study was sought from Stellenbosch University Human Ethics Committee, South Africa ref. no. N22/06/068_RECIP_WITS_M200706.
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Consent was granted by the facility manager, the staff, and the patients prior to implementation of the QI project. Written informed consent to participate was received from participants.
AVAILABILITY OF DATA AND MATERIALS
The data of current study are available from corresponding author, [A.B], on a reasonable request.
FUNDING
This research is part of a bigger research on COVID-19 pandemic and health systems’ response in South Africa and Malawi. The RSA part of this study received funding from the South African Medical Research Council (SA MRC) under a Self-Initiated Research (SIR) Grant. The findings from this paper inform the bigger study.
ACKNOWLEDGEMENTS
The authors would like to thank the Delft Community Health Centre management and the QI team for their commitment to participating in the project, and all the participants. We also thank Dr Jeannine Uwimana-Nicol for her technical input. In addition, we thank the NDoH for permission to undertake the project.

