All published articles of this journal are available on ScienceDirect.

Utilization of ART Services Among People Living with HIV During the COVID-19 Pandemic: A Case of Kampala District
Abstract
Introduction:
The intense pressure on the health system coupled with strict measures have interrupted ART service utility during the COVID 19 pandemic. In this study, we assessed the Utilization of ART services among People Living with HIV during the COVID-19 pandemic in Kampala District, Uganda.
Methods:
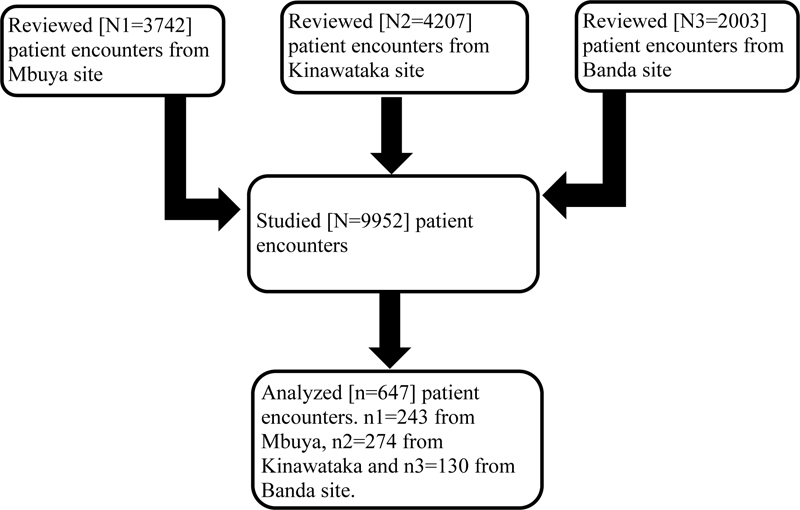
We studied 9952 records of patient encounters between 24th March and 1st June 2020 from the Open Medical Records System (EMR) and obtained an analytical sample of 647 encounters for PLHIV enrolled in Kampala district; 243 from the Mbuya site, 274 from Kinawataka site and 130 from Banda site. We assessed factors associated with inadequate ART utilization using the modified poison regression (generalized linear model with a poisoned family and a log link) and reported clustered robust standard errors with their corresponding Prevalence Ratios.
Results and Discussion:
The rate of ART utilization during the COVID-19 pandemic in the Kampala district was inadequate (14.71%). PLHIV who were in WHO clinical stage 3 had aPR=18.065, 95%CI=17.396 18.759, and P-value =0.001 as compared to those in WHO stage 1. PLHIV who were obese had aPR=1.439, 95% CI=1.103 1.879, P-value =0.007 as compared to those with normal BMI.
Conclusion:
The factors associated with inadequate ART utilization were body mass index and WHO clinical staging of the disease. This information is crucial for strengthening HIV programs and interventions in terms of access to ART services, with a focus on obese infected individuals and those with advanced HIV disease during pandemics that require lock-down measures.
1. INTRODUCTION
The COVID-19 pandemic presents several challenges to the Human Immunodeficiency Virus (HIV) service delivery, particularly in Sub-Saharan Africa, which suffers from an overwhelming epidemic of infectious diseases [1-3]. Quarantine and social distancing in a bid to curb the spread of the novel coronavirus have disrupted the 95, 95-95 UNAIDS targets [4]. While there is currently limited knowledge about the potential effects of COVID-19 on people living with HIV [4], healthcare professionals acknowledged that HIV-positive patients on successful antiretroviral therapy (ART) with suppressed viral load would most likely fair better against COVID-19 than those with uncontrolled HIV and weakened immune systems [4, 5].
In Uganda, measures to control the spread of COVID-19 were implemented from March 2020. These included a ban on public and private transport, the closure of schools, suspension of mass gatherings, closure of non-essential businesses, travel restrictions from one district to another and the enforcement of curfew, among others. While deemed necessary to prevent the spread of the COVI-19 outbreak, lockdown measures in Uganda had an immediate impact on daily life and HIV services [6, 7].
The prohibition on public and private transportation dramatically hampered facility-based HIV care in Reach Out Mbuya, as patients were severely restricted in physically accessing the ART clinics, especially for ART refills. In Reach Out Mbuya, drugs were initially supplied to clients through Fast Track Drug Refills (FTDR), Community Client-Led ART Delivery (CCLAD), and Community Drug Distribution Points, in addition to facility-based ART refills (CDDPs). Depending on their level of adherence, clients were provided medications for one or three months. Recognizing that restrictions put in place to combat the spread of COVID-19 may obstruct access to ART, Reach Out Mbuya extended ART refill to up to six months for stable clients and actively followed up with clients via phone calls. The drugs were then transported using bicycles, motorcycles (Boda-boda), trucks, and buses to clients, including the truck drivers who were stacked at points of entry besides the ART clinics that remained operational. Clients who returned to their villages were connected to the nearest health center to receive medications and have their medical data recorded. Clients who could not be reached were physically traced.
There are concerns regarding the underutilization of ART treatment during the COVID-19 pandemic, which may accelerate opportunistic infections and compromise the patient’s immunity, further exacerbating poor treatment outcomes [3]. The interruption of planned appointments could affect HIV/AIDS treatment outcomes. For instance, HIV mortality can increase by 10% in high-burden settings, respectively due to disruptions in access to medication compared to pre-COVID-19 pandemic levels [8]. As a result, more than 500,000 additional deaths from AIDS-related illnesses, including tuberculosis, may occur in Sub-Saharan Africa in 2020–2021 [9]. HIV/AIDS care services in the context of COVID-19 have become increasingly complex and have resulted in several challenges, especially among HIV high-risk populations. Lack of clear information on the quantitative experiences such services utility may contribute to poor planning, management, and implementation of ART services in the event of epidemics and pandemics. Therefore, this study aimed to determine the factors associated with the utilization of ART during the COVID 19 pandemic lockdown period among people living with HIV.
2. MATERIALS AND METHODS
2.1. Study Design and Setting
A cross-sectional study was conducted in the Kampala district between the 24th of March and the 1st of June 2020, during which the government imposed a national lockdown that began on the 25th of March and ended on the 2nd of June 2020. More than 1000 patient encounters had been scheduled for daily ART routine refills. On average, at least 300 PLHIV are seen at Reach Out Mbuya Kampala sites of Mbuya, Kinawataka and Banda sites per week. An equal proportion of them is seen through the Differentiated Service Delivery (DSD) model.
The HIV clinic runs five days a week, even during the lockdown. Clients are given appointment days to come for refills and are reminded ahead of time, those who miss their appointments are followed up by phone call, and if they do not respond within a month, they are physically traced by the community support team.
Data was collected from the client’s files and information on scheduled ART clinic encounters, health system factors, individual factors, and clinical factors was abstracted. We employed a simple random sampling technique and enrolled 646 study participants.
In this study, ART utilization referred to the number of goal-oriented clinic visits made by PLHIV enrolled at Reach Out Mbuya ART sites in Kampala and received ART treatment between 24th March 2020 to 1st June 2021.
Leslie Kish's (1964) formula was used to estimate the sample size of 647 participants. Considering a design effect of 2 is recommended for unbiased estimates of the prevalence (Salganik, 2006).
The proportion of those who had good utilization of ART was determined as a percentage of those who fulfilled at least one planned goal-oriented clinic visit out of the total number of all planned goal-oriented clinic visits between 24th March 2020 to 1st June 2021, with no visit deemed to as poor utilization of ART.
To determine factors associated with poor ART utilization, bivariate and multivariate analyses were done using modified poison regression (generalized linear model with a poisoned family and a log link) and reported clustered robust standard errors. All factors with a p-value <0.2 at bivariate were considered for the multivariate analysis. Interactions were assessed by introducing combinations (covariates) of the non-significant dropped with the significant variables that had remained in the model to investigate their significance in the model. Confounding was assessed by at least a 10% change in the crude and adjusted odds ratios. Statistical significance was determined at a p-value <0.05.
3. RESULTS
We studied 9952 records of the patient from the open Medical Records System with ART refill appointments and obtained an analytical sample of 647 patients (Fig. 1).
The majority of the study participants (63%; 407/647) were females. At the time of the study, the median age group was 39 years. 617(97.9%) had suppressed viral loads, 391(85.2%) stayed within 5KM from the clinic site, and most of the PLHIV 262(42.2%) were obese (Table 1).
Of the 647 PLHIV studied, 95(14.71%) had inadequate ART utilization.
Results from the multivariate Poisson regression are shown in Table 2. WHO clinical staging and Body Mass Index were independently associated with inadequate ART utilization. PLHIV who were in WHO clinical stage 3 were 18.065 times more likely to have inadequate ART utilization (aPR=18.065, 95%CI=17.396 18.759, P- value = 0.001) as compared to those in WHO stage 1. PLHIV who were obese were 1.439 times more likely to have inadequate ART utilization (aPR=1.439, 95% CI=1.103 1.879, P-value =0.007) as compared to those with normal BMI.
| Variable | n | % | |
|---|---|---|---|
| ART utilization | |||
| Good | 551 | 85.29 | |
| Poor | 95 | 14.71 | |
| Gender | |||
| Female | 407 | 63 | |
| Male | 239 | 37 | |
| Age, median (IQR) | 39 [32, 47] | ||
| Viral load | |||
| Not suppressed | 13 | 2.1 | |
| Suppressed | 617 | 97.9 | |
| Telephone contact | |||
| Present | 123 | 19.0 | |
| Absent | 523 | 81.0 | |
| Distance | |||
| Less than 5KM | 391 | 85.2 | |
| More than 5Km | 68 | 14.8 | |
| BMI | |||
| Underweight | 41 | 6.6 | |
| normal weight | 216 | 34.8 | |
| overweight | 102 | 16.4 | |
| Obese | 262 | 42.2 | |
| WHO Clinical Staging | |||
| Treatment stage 1 | 637 | 98.6 | |
| Treatment stage 2 | 6 | 0.9 | |
| Treatment stage 3 | 3 | 0.5 | |
| Duration on ART | |||
| less than 5 years | 228 | 35.4 | |
| 5 to less than 10 years | 250 | 38.8 | |
| 10 and more years | 167 | 25.9 | |
| Underlying illness | |||
| No | 69 | 14.9 | |
| Yes | 388 | 85.1 | |
| ART adherence history | |||
| Poor | 2 | 0.3 | |
| Fair | 2 | 0.3 | |
| Good | 642 | 99.4 | |
| n frequency, % percentage | |||
| Variable | Bivariate | Multivariate | ||||||
|---|---|---|---|---|---|---|---|---|
| ART utilization n (%) | PR (95% CI) | p-value | aPR | (95% CI) | P-value | |||
| Poor | Good | |||||||
| Gender | Female | 60(14.74) | 347(85.26) | 1 | ||||
| Male | 35(14.54) | 204(85.36) | 1.009(0.782 1.303) | 0.941 | ||||
| Age | <25 years | 10(14.29) | 60(85.71) | 1 | ||||
| 25 to 34 years | 30(16.85) | 148(83.15) | 1.198(0.753 1.906) | 0.446 | ||||
| 35 to 44 years | 31(13.84) | 193(86.16) | 1.007(0.607 1.671) | 0.979 | ||||
| ≥45 years | 24(13.79) | 150(86.21) | 1.026(0.644 1.637) | 0.911 | ||||
| Viral load | Not suppressed | 2(15.38) | 11(84.62) | 1 | ||||
| Suppressed | 91(14.75) | 526(85.25) | 0.965(0.159 5.823) | 0.969 | ||||
| Distance | Less than 5KM | 40(10.23) | 351(89.77) | 1 | 1 | 1 | ||
| 5Km or more | 13(19.12) | 55(80.88) | 1.854(1.003 3.427) | 0.049** | 1.710 | (0.856 3.418) | 0.129 | |
| BMI | Normal weight | 4(9.76) | 37(90.24) | 1 | 1 | 1 | ||
| Underweight | 26 (12.04) | 190(87.96) | 0.811(0.243 2.706) | 0.733 | 0.656 | (0.374 1.150) | 0.141 | |
| Overweight | 13 (12.75) | 89 (87.25) | 1.059(1.048 1.069) | 0.001** | 1.131 | (0.912 1.403) | 0.262 | |
| Obese | 48(18.32) | 214(81.68) | 1.522(1.019 2.273) | 0.040** | 1.439 | (1.103 1.879) | 0.007* | |
| Duration on ART | less than 5 years | 33(14.47) | 195(85.53) | 1 | ||||
| 5 to less than 10 years | 35(14.00) | 215(86.00) | 1.009(0.588 1.730) | 0.974 | ||||
| 10 and more years | 27(16.17) | 140(83.83) | 1.212(0.677 2.170) | 0.517 | ||||
| WHO Clinical Staging | Treatment stage 1 | 91(14.29) | 547(85.71) | 1 | 1 | 1 | ||
| Treatment stage 2 | 2(33.33) | 4(66.67) | 2.158(0.547 8.511) | 0.272 | 2.683 | (0.637 11.309) | 0.178 | |
| Treatment stage 3 | 2(66.67) | 1(33.33) | 4.950(1.941 12.624) | 0.001** | 18.065 | (17.396 18.759) | 0.001* | |
| Underlying illness | No | 8(11.76) | 60(88.24) | 1 | ||||
| Yes | 52(13.40) | 336(86.60) | 1.216(0.627 2.359) | 0.563 | ||||
| ART adherence history | Poor | 0(00) | 2(100.00) | 1 | ||||
| Fair | 1(50.00) | 1(50.00) | 5.14e+(1.63e-1.62e+) | 0.785 | ||||
| Good | 94(14.64) | 548(85.36) | 1.67e+(2.9e- 9.55e+) | 0.678 | ||||
4. DISCUSSION
Although research on the impact of the COVID-19 pandemic on health services is rapidly growing, there is limited empirical evidence on the utilization of ART services among PLHIV during the lockdown. As a result, we record the proportion and factors associated with the utilization of ART services among PLHIV in Kampala district, Uganda.
This study found 85.29% ART utilization among PLHIV receiving care from Reach Out Mbuya HIV clinics in Kampala. These findings are in contrast to other studies conducted in two different areas of China [10, 11], which reported over one-third (35.1%, 1782/5084) of PLHIV have had a risk of ART treatment interruption during the COVID-19 outbreak and 64.15% PLHIV in Hubei province reported difficulty accessing ARV, respectively. This distinction can be explained by the fact that China was more affected by COVID 19 than the rest of the world, with more COVID 19 infections and also implemented stricter COVID-19 prevention and control measures, but it can also be explained by the fact that Reach Out Mbuya provides a holistic model of care to her HIV patients, with a strong community arm aspect that tracks patients, which ensured better ART utilization and continuity of care.
Our findings revealed that PLHIV who are in WHO stage III were 18.1 times more likely to have inadequate ART utilization during the COVID-19 pandemic as compared to those in WHO stage I.
This can be explained by the fact that WHO clinical stage III is associated with depression [12], which has a direct effect on ART adherence [13]; such patients may always be confined into isolation. This could have been fueled by the COVID-19 prevention measures such as movement restrictions and such patients could not come for their ART refills. Similarly, in other studies, depression was more than 3-fold higher during COVID-19 compared with before the COVID-19 pandemic in the USA [14], which negatively affected ART utilization. It is also possible that these patients died and were unable to come for ART refills, as data suggests that advanced HIV disease (WHO stage III/IV) is associated with a higher mortality rate [15], which could explain their low ART utilization.
Inadequate utilization of ART in our study was also associated with Body Mass Index. PLHIV who were obese were 1.439 times more likely to have inadequate ART utilization compared to those with normal Body Mass Index. This could be because HIV-infected obese people are more likely to develop COVID-19 and be hospitalized or confined [16], as there is a higher risk of comorbid diseases and mortality in HIV-infected obese people [17]. It is also possible that clients with a higher BMI tire easily [18] and that during a time when transportation was restricted as a measure to combat COVID-19, people had to walk long distances to reach health care facilities, and those who are obese may have found it impossible to walk long distances [18], resulting in low ART use.
5. LIMITATIONS OF THE STUDY
The study had some limitations, including the use of secondary data that lacked information on some key variables such as substance and drug abuse, education level, and occupation. Information bias may be inevitable in our study, considering that we did not incorporate qualitative findings to explore the observed factors associated with inadequate ART utilization.
CONCLUSION
The ART utilization during the COVID-19 pandemic in the Kampala district was inadequate (14.71%), which was lower than that reported in China. ART utilization was independently associated with body mass index and WHO clinical staging of the disease. This information is crucial for strengthening HIV programs and interventions in terms of access to ART services, with a focus on obese infected individuals and those with advanced HIV disease during pandemics that require lockdown measures.
LIST OF ABBREVIATIONS
| ART | = Antiretroviral Therapy |
| CCLAD | = Community Client-Led ART Delivery |
| FTDR | = Fast Track Drug Refills |
| DSD | = Differentiated Service Delivery |
RECOMMENDATIONS
Interventions targeting improvement of access to ART services during the COVID19 pandemic must be accelerated to target infected individuals who are obese and those with advanced HIV disease.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The ethical approval was provided by Mulago hospital's research and ethics committee.
HUMAN AND ANIMAL RIGHTS
No animals were used for studies that are the basis of this research. All the humans used were in accordance with the Helsinki Declaration of 1975.
CONSENT FOR PUBLICATION
Mulago hospital's research and ethics committee waived requirements for informed consent to review existing medical records. Identification codes were used instead of patients' names to maintain confidentiality and anonymity, and the information was kept under lock and key.
STANDARDS OF REPORTING
STROBE guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of this study are available within the article.
FUNDING
This research was funded by the Reach out Mbuya community health initiative. The funder played no role in conceptualizing the research, data analysis and writing of the manuscript.
CONFLICT OF INTEREST
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
ACKNOWLEDGEMENTS
The management of Reach Out Mbuya Community Health Initiative is appreciated for granting us support and permission to work within its facilities. We thank the M&E officers who palyed an important role in abstracting the data.

