All published articles of this journal are available on ScienceDirect.

Associations and Trends in Cause-Specific Rates of Death Among Persons Reported with HIV Infection, 23 U.S. Jurisdictions, Through 2011
Authors Info & Affiliations
Abstract
Background:
Published death rates for persons with HIV have not distinguished deaths due to HIV from deaths due to other causes. Cause-specific death rates would allow better assessment of care needs.
Methods:
Using data reported to the US national HIV surveillance system, we examined a) associations between selected decedent characteristics and causes of death during 2007-2011, b) trends in rates of death due to underlying causes among persons with AIDS during 1990-2011, and among all persons with diagnosed HIV infection (with or without AIDS) during 2000-2011.
Results:
During 2007-2011, non-HIV-attributable causes of death with the highest rates per 1,000 person-years were heart disease (2.0), non-AIDS cancers other than lung cancer (1.4), and accidents (0.8). During 1990-2011, among persons with AIDS, the annual rate of death due to HIV-attributable causes decreased by 89% (from 122.0 to 13.2), and the rate due to non-HIV-attributable-causes decreased by 57% (from 20.0 to 8.6), while the percentage of deaths caused by non-HIV-attributable causes increased from 11% to 43%. During 2000-2011, among persons with HIV infection, the rate of death due to HIV-attributable causes decreased by 69% (from 26.4 to 8.3), and the rate due to non-HIV-attributable causes decreased by 28% (from 10.5 to 7.6), while the percentage of deaths caused by non-HIV-attributable causes increased from 25% to 48%.
Conclusion:
Among HIV-infected persons, as rates of death due to HIV-attributable causes decreased, rates due to non-HIV-attributable causes also decreased, but the percentages of deaths due to non-HIV-attributable causes, such as heart disease and non-AIDS cancers increased.
INTRODUCTION
Widespread use of highly active antiretroviral therapy (HAART) after 1995 resulted in a marked reduction in deaths among persons with human immunodeficiency virus (HIV) infection, primarily because of reductions in deaths attributable to opportunistic illnesses (infections or cancers that meet the criteria for defining acquired immunodeficiency syndrome [AIDS], which is stage 3 of HIV infection) [1, 2]. The annual number of deaths among HIV-infected persons declined by more than 50% during 1996-2006 in the United States [3]. The benefits of HAART are suppression of the virus, restoration of immune function (measurable as CD4 T-lymphocyte counts), reduction in hospitalization rates among persons with diagnosed HIV infection, and prolonged survival [4-6]. As HIV-infected persons are surviving to older ages, the spectrum of causes of death among them is changing - the proportion of deaths with AIDS-defining causes has decreased while the proportion with diseases not specifically attributable to HIV has increased [2, 3, 7-12].
Examining the changes in causes of death can inform the clinical management of HIV-infected persons. Previous studies of trends of causes of death among HIV-infected persons are based on clinic-based cohorts of HIV-infected patients or vital statistics in the general population. Little information has been published on cause-specific rates of death in which the denominators consist of HIV-infected persons reported to population-based HIV surveillance programs [13]. Assessing mortality in only the HIV-infected population is more useful for detecting variation in the availability, utilization, timeliness, or quality of care for this population. Further to our knowledge, there are as yet no studies that have used national level data on HIV-infected persons to compare deaths due to HIV with deaths due to other causes. The goal of this analysis was to use such data reported to the U.S. national HIV surveillance system to investigate death rates among persons reported with HIV infection. We examined a) associations between selected demographic or clinical characteristics and the risk of death during 2007-2011 due to HIV-attributable and non-HIV-attributable causes, b) trends during 1990-2011 in cause-specific rates of death among persons with infection ever classified as stage 3 (AIDS), and during 2000-2011 among all persons with diagnosed HIV infection, including those without AIDS for which reporting was very incomplete before 2000.
METHODS
Using information from the national HIV surveillance system of the Centers for Disease Control and Prevention (CDC), we analyzed data on underlying causes of death among HIV-infected persons reported to CDC through December 2014 who resided in 23 jurisdictions when first diagnosed (20 states: Arizona, Colorado, Connecticut, Delaware, Florida, Indiana, Iowa, Maryland, Michigan, Minnesota, Missouri, New Jersey, New Mexico, Nevada, New York, Oregon, Rhode Island, South Carolina, Texas, Wisconsin, and 3 municipalities: Los Angeles County, San Francisco County, Philadelphia). These jurisdictions were selected because of the relative quality and completeness of their mortality data (at least 85% of the deaths they reported to CDC had data on underlying cause), which their health departments obtained by linking HIV surveillance data with either state/local vital records data or the National Death Index. The health departments reported the data to CDC without key personal identifiers (e.g., name, Social Security number) that they used to link HIV cases to death records. The data were subjected to deduplication processing at both the jurisdictional and national levels to ensure that each case was counted only once and was credited to the person’s state of residence at the time of diagnosis. Causes of death were identified by codes in the International Classification of Diseases, Ninth Revision and International Classification of Diseases Tenth Revision (ICD-9 [for deaths in 1990-1998] and ICD-10 for deaths in 1999-2011]) [14, 15]. For deaths before 1999, HIV infection, including AIDS, was identified by codes introduced by National Center for Health Statistics in 1987 to supplement the ICD-9 [16]. We classified deaths as “HIV-attributable” if the reported underlying cause was HIV infection, indicated either explicitly (by an ICD code for HIV infection itself) or implicitly (by an ICD code for an AIDS-indicative opportunistic illness or immunodeficiency [cell-mediated or unspecified type, not an antibody-mediated or congenital type]). We assumed HIV infection was underlying an AIDS-indicative opportunistic illness or immunodeficiency because all the decedents had HIV infection reported to the surveillance system, even if not mentioned on the death certificate. We classified deaths as “non-HIV-attributable” if they did not meet our criteria for being HIV-attributable. Persons missing information on underlying causes of death were excluded from the analysis. We grouped the non-HIV-attributable causes into 13 categories: viral hepatitis C, chronic liver disease, other non-AIDS infections, lung cancer, other non-AIDS cancers, heart disease, diabetes, stroke, kidney disease, unintentional injury or poisoning (accidents), assault (homicide), self-harm (suicide), and “other” (Appendix). Deaths in this analysis included those reported by health departments of the 23 jurisdictions among persons who resided in any of those jurisdictions when first diagnosed with HIV infection, regardless of whether the persons resided in the same jurisdiction at the time of death as when first diagnosed. We excluded deaths reported only by health departments outside the 23 jurisdictions, which constituted <1% of total deaths in this analysis.
We used SAS version 9.3 and Joinpoint version 4.2.0.2, a statistical software for the analysis of continuous linear trends with change points (i.e., joinpoints) [17].
Associations of Selected Patient Characteristics with HIV-Attributable and Non-HIV-Attributable Deaths
We examined the relationship between selected patient characteristics and the age-adjusted rate of death due to HIV-attributable and non-HIV-attributable causes among persons with diagnosed HIV infection in 2007-2011. We limited this particular analysis to no more than this 5-year period to investigate recent burden of disease. Death rates were calculated as the number of deaths per 1,000 person-years for persons living with HIV infection during 2007-2011, including persons diagnosed before this period and still alive at its beginning, as well as those diagnosed during this period. To control for changes in the age distribution of the study population of persons with diagnosed HIV, the death rates were age-adjusted based on the standard age distribution of the year-2000 U.S. population. Each person with diagnosed HIV infection before 2011 and not dead before 2007 contributed person-years to the denominator, based on the number of months alive after diagnosis during 2007-2011, divided by 12. The age-specific rates of death were based on the number of deaths and person-years observed in specific age groups. Therefore, each person could contribute person-years to the rate calculation in multiple age groups as he or she aged during the period. To compare rates in the demographic, transmission, and clinical groups, we calculated rate ratios (RR) by dividing the rate in a subgroup by the rate in a referent subgroup of corresponding groups. The rate in a sub group was considered significantly different from the rate in the referent group if the 95% confidence interval (CI) for the rate ratio did not include 1.0.
Trends in Underlying Causes of Death Among Persons with HIV Infection
We investigated trends in annual rates of death among persons with HIV infection. To determine changes from the pre-HAART era through the end of our study period, we assessed trends during 1990-2011 among persons with AIDS, rather than all persons reported with infection, because data for persons whose HIV infection had not progressed to AIDS were not uniformly collected over time and across all jurisdictions during the earlier part of that period. The denominator was the number of persons with infection ever classified as AIDS alive at the beginning of the year for which the rate was calculated, plus the number whose infection first met the criteria for AIDS later in that year. The numerator was the number of deaths due to a particular category of underlying causes among persons in the denominator. The rates were age-adjusted based on the standard age distribution of the year-2000 U.S. population. To assess trends in the rates of death among persons with AIDS during 1990-2011, we used joinpoint regression to calculate the annual percentage change (APC) in the rate during the various portions of the period that had different rates of change [18].
We also examined trends among persons with HIV infection (with or without AIDS) during 2000-2011. We limited this particular analysis to the shorter period, 2000-2011, because reporting was incomplete before 2000. We assessed a trend as significant if the 95% confidence interval (CI) for the APC did not include zero. During 2000-2011, trends by race/ethnicity did not change enough to require joinpoint analysis, so we used Poisson regression with a log link function to calculate an estimated percentage change (EAPC) during the period. We assessed a trend as significant if the 95% CI for the EAPC did not include zero.
RESULTS
Characteristics of HIV-infected Persons
Of 592,154 persons who received a diagnosis of HIV infection, resided in the 23 jurisdictions at diagnosis and were alive for some time during 2007-2011, 74% were male, 42% were black/African American (hereafter referred to as “blacks”), 29% were white, 24% were Hispanic/Latino, 1% were Asian/Native Hawaiian or other Pacific islander, less than 1% were American Indian/Alaska Native, 4% were persons of multiple races, and 26% had AIDS at (i.e., within 3 months of) diagnosis of HIV infection. Of these persons, 56,257 (9.5%) died during the study period. The median age at death was 50 years; of the persons who died, 73% were male, 48% were black, 27% were white, 20% were Hispanic/Latino, <1% were Asian/Native Hawaiian or Other Pacific Islander, <1% were American Indian/Alaska Native, and 35% had AIDS at diagnosis of HIV infection.
Associations of Selected Patient Characteristics with Death Due to HIV-attributable Causes
Of the 54,491 deaths during 2007-2011 for which we had data on the underlying cause, 31,404 (58%) were due to HIV-attributable causes. The age-adjusted rate of death per 1,000 person-years was lower among males (10.2) than females (12.0) (rate ratio [RR] 0.86 [95% CI, 0.82-0.89]). Compared with the rate among whites (7.6), the rate of death was higher among blacks (13.0) (RR 1.71 [95% CI, 1.62-1.80]), American Indians/Alaska Natives (11.6) (RR 1.52 [95% CI, 1.06-2.18]), Hispanics/Latinos (10.0) (RR 1.32 [95% CI, 1.24-1.40]), and persons of multiple races (14.3) (RR 1.88 [95% CI, 1.71-2.07). In comparison with men whose only known mode of exposure to HIV infection was male-to-male sexual contact, the rate of death due to HIV-attributable causes was higher among men and women with a history of injection drug use (IDU), men with a history of both male-to-male sexual contact and IDU, and men and women with a history of heterosexual contact with a partner who had HIV infection or a history of IDU (Table 1). Persons who had AIDS at diagnosis had twice the rate of death due to HIV-attributable causes as persons who did not (RR 2.24 [95% CI, 2.13-2.35]).
Age-adjusted rates* of death due to HIV-attributable and non-HIV-attributable causes among persons living with diagnosed HIV infection who died during 2007-2011 in 23 U.S. jurisdictions, and rate ratios comparing rates in demographic, transmission, and clinical groups.
| HIV-attributable deathsa | Non-HIV-attributable deathsb | Person-years at risk | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Rate | Rate ratio | (95% CI) | Rate | Rate ratio | (95% CI) | ||||||
| Total | 10.8 | N/A | N/A | 8.7 | N/A | N/A | 2,504,579.8 | ||||
| Age group | |||||||||||
| <25 | 4.2 | 0.39 | (0.36 - 0.43) | 2.0 | 0.36 | (0.32 - 0.41) | 113,941.1 | ||||
| 25-34 | 8.1 | 0.75 | (0.71 - 0.78) | 3.1 | 0.58 | (0.54 - 0.62) | 329,551.0 | ||||
| 35-44 | 10.8 | 1.0 (referent) | 5.3 | 1.0 (referent) | 726,494.5 | ||||||
| 45-54 | 13.5 | 1.25 | (1.21 - 1.28) | 9.7 | 1.83 | (1.76 - 1.90) | 873,554.3 | ||||
| 55-64 | 17.3 | 1.60 | (1.55 - 1.65) | 17.9 | 3.37 | (3.24 - 3.51) | 365,250.7 | ||||
| 65+ | 24.5 | 2.27 | (2.16 - 2.37) | 30.7 | 5.78 | (5.51 - 6.07) | 95,788.3 | ||||
| Sex | |||||||||||
| Male | 10.2 | 0.86 | (0.82 - 0.89) | 8.8 | 1.04 | (1.00 - 1.09) | 1,845,953.2 | ||||
| Female | 12.0 | 1.0 (referent) | 8.5 | 1.0 (referent) | 658,626.6 | ||||||
| Race/ethnicity | |||||||||||
| American Indian/Alaska Native | 11.6 | 1.52 | (1.06 - 2.18) | 10.6 | 1.25 | (0.70 - 2.61) | 5,057.6 | ||||
| Asian/Native Hawaiian & Other Pacific Islander | 6.2 | 0.82 | (0.62 - 1.07) | 5.4 | 0.64 | (0.44 - 0.93) | 24,877.7 | ||||
| Black/African American | 13.0 | 1.71 | (1.62 - 1.80) | 9.8 | 1.16 | (1.10 - 1.23) | 1,037,921.6 | ||||
| Hispanic/Latino | 10.0 | 1.32 | (1.24 - 1.40) | 7.1 | 0.84 | (0.79 - 0.90) | 594,810.9 | ||||
| White | 7.6 | 1.0 (referent) | 8.4 | 1.0 (referent) | 750,788.2 | ||||||
| Multiple races | 14.3 | 1.88 | (1.71 - 2.07) | 12.2 | 1.45 | (1.30 - 1.62) | 91,123.8 | ||||
| Transmission category | |||||||||||
| Male-to-male sexual contact | 7.8 | 1.0 (referent) | 6.8 | 1.0 (referent) | 1,035,123.2 | ||||||
| Injection drug use, male | 16.3 | 2.09 | (1.78 - 2.45) | 14.9 | 2.20 | (1.89 - 2.57) | 236,010.8 | ||||
| Injection drug use, female | 16.7 | 2.15 | (1.89 - 2.43) | 13.4 | 1.98 | (1.73 - 2.25) | 136,151.8 | ||||
| Male-to-male sexual contact and injection drug use | 12.3 | 1.59 | (1.41 - 1.78) | 11.2 | 1.65 | (1.46 - 1.87) | 130,740.8 | ||||
| Heterosexual contact, male | 13.0 | 1.66 | (1.52 - 1.83) | 10.6 | 1.57 | (1.41 - 1.75) | 173,412.6 | ||||
| Heterosexual contact, female | 10.5 | 1.34 | (1.26 - 1.43) | 7.1 | 1.05 | (0.97 - 1.13) | 344,705.0 | ||||
| Other | 11.9 | 1.53 | (1.46 - 1.61) | 9.1 | 1.34 | (1.27 - 1.42) | 448,435.5 | ||||
| Stage of infection at diagnosis | |||||||||||
| Stage 3 (AIDS) | 19.2 | 2.24 | (2.13 - 2.35) | 9.2 | 1.05 | (1.00 - 1.11) | 629,748.0 | ||||
| Not stage 3 | 8.6 | 1.0 (referent) | 8.7 | 1.0 (referent) | 1,627,209.7 | ||||||
| Missing | 10.6 | 1.24 | (1.12 - 1.37) | 8.1 | 0.93 | (0.87 - 0.99) | 247,622.1 | ||||
* Rate is age-adjusted (except for specific age group rates) per 1,000 person-years among those with diagnosed HIV infection.
aHIV attributable deaths were those for which HIV, AIDS-indicative opportunistic illness (AIDS OI), or immunodeficiency was the underlying cause of death.
bNon-HIV-attributable deaths were all other deaths for which the underlying cause was known.
Associations of Selected Patient Characteristics with Death Due to Non-HIV-Attributable Causes
Non-HIV-attributable underlying causes accounted for 23,087 (42%) of the deaths with known causes among persons with HIV infection during 2007-2011. Overall, the age-adjusted rate of death per 1,000 person-years due to non-HIV-attributable causes was lower than the rate due to HIV-attributable causes (8.7 and 10.8, respectively) (Table 1). Age-specific rates of death due to HIV-attributable and non-HIV-attributable causes were similar, increasing with age. The rates of death were similar among males and females. Compared with the rate among whites (8.4), the rate of death was higher among blacks (9.8) (RR 1.16 [95% CI, 1.10-1.23]) and persons of multiple races (12.2) (RR 1.45 [95% CI, 1.30-1.62]), and lower among Hispanics/Latinos (7.1) (RR 0.84 [95% CI, 0.79-0.90]) and Asians/Native Hawaiians and Other Pacific Islanders (5.4) (RR 0.64 [95% CI, 0.44-0.93]). In comparison with men who had a history of male-to-male sexual contact, the rate of death due to non-HIV-attributable causes was higher among men and women who had a history of IDU, men with a history of both male-to-male sexual contact and IDU, and men with a history of heterosexual contact with a woman who had HIV infection or a history of IDU (Table 1). The rates of death due to non-HIV-attributable causes among persons who had AIDS and those who did not were similar.
Specific Non-HIV-Attributable Causes of Deaths Among Persons with HIV Infection
During 2007-2011, among persons with HIV infection, heart disease, non-AIDS cancers, and accidents were the leading causes of death overall (Table 2). The age-adjusted rate of death per 1,000 person-years due to heart disease was highest among persons aged 65 years or older (9.0). The rate of death due to heart disease ranged from 1.6 among Hispanics/Latinos and whites to 2.4 among blacks. The rate of death due to non-AIDS cancers other than lung cancer ranged from 1.3 among Hispanics/Latinos to 1.6 among blacks. Men and women with a history of IDU also experienced high rates of death due to accidents (2.9 and 2.3, respectively). Of the deaths due to accidents, 62% were due to accidental poisoning by drugs (e.g., overdoses of narcotics or hallucinogens). We limited this analysis on specific non-HIV-attributable causes to blacks, Hispanic/Latinos, and whites because of small numbers in the other racial/ethnic groups.
Trends in Death Rates Among Persons with AIDS During 1990-2011
During 1990-2011, among persons with AIDS, the age-adjusted rate of death per 1,000 persons due to underlying HIV-attributable causes decreased by 89% (from 122.0 in 1990 to 13.2 in 2011). The corresponding rate due to non-HIV-attributable-causes also decreased, but not as much-by 57% (from 20.0 in 1990 to 8.6 in 2011). Because deaths due to HIV-attributable causes decreased more than deaths due to non-HIV-attributable causes, the percentage of deaths due to non-HIV-attributable causes increased from 11% in 1990 to 43% in 2011.
During 1990-1995, the age-adjusted annual rate of death due to HIV-attributable causes per 1,000 persons was relatively stable, ranging from 113.2 to 122.0. It then declined greatly, from 117.9 in 1995 to 35.7 in 1998 (Fig. 1, with an annual percentage change [APC] of −32.5% [95% CI = −37.9% to −26.6%]) during those 4 years. It then declined more slowly to 13.2 in 2011 (APC −7.6% [95% CI −8.1% to −7.1%]). The trends in the age-adjusted rate of death due to non-HIV-attributable causes (combined into a single category) followed a pattern parallel to that for death due to HIV, but with much slower decreases during 1995-2000 and 2000-2011. The rate of death due to non-HIV-attributable causes decreased from 20.0 in 1995 to 10.4 in 2000 (APC −10.5% [95% CI −12.9% to −8.1%]), and then declined much more slowly to 8.6 in 2011 (APC −2.2% [95% CI −2.6% to −1.8%]). Regarding specific non-HIV-attributable causes of death, the rate of death due to heart disease dropped from 5.0 in 1990 to 1.7 in 2011 (APC −3.8% [95%CI −4.4% to −3.1%]), the rate of death due to non-AIDS cancers declined from 2.7 in 1990 to 2.1 in 2011 (APC −2.1% [95% CI −2.8% to −1.4%]), and the rate of death due to selected other chronic diseases (chronic liver disease, hepatitis C, stroke, diabetes, and kidney disease) as a group had no significant trend during 1990-2000 (despite a drop from 2.3 in 1998 to 1.4 in 2000), and thereafter slightly decreased to 1.2 in 2011 (APC −2.3% [95% CI −3.5% to −1.2%]) (Fig. 2). However, trends in the rate of death due to non-AIDS-defining infections (bacterial or unspecified septicemia and other infections not specifically indicative of AIDS) followed a pattern more like the trends in the rate of death due to HIV-attributable causes, with an increase from 1.7 in 1990 to 2.2 in 1995 (APC 8.7% [95% CI 1.4% to 16.5%]), followed by a rapid decrease to 0.5 in 2000 (APC −23.9% [95% CI −32.3% to −14.4%]), and then a slow decline to 0.3 in 2011 (APC −5.7%[95% CI −8.5% to −2.9%)]. The rate of death due to external causes (injury or poisoning in the context of accident, homicide, or suicide) decreased from 1.5 in 1990 to 0.9 in 2002 (APC −3.4% [95% CI −6.0% to −0.7%]), and then increased to 1.2 in 2011 (APC 2.9% [95% CI 0.1% to 5.8%]).
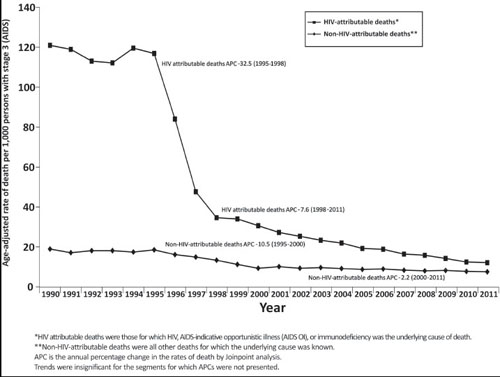
Trends in age-adjusted rates of death due to HIV-attributable and non-HIV-attributable causes among persons with stage 3 classification (AIDS), 23 U.S jurisdictions, 1990-2011.
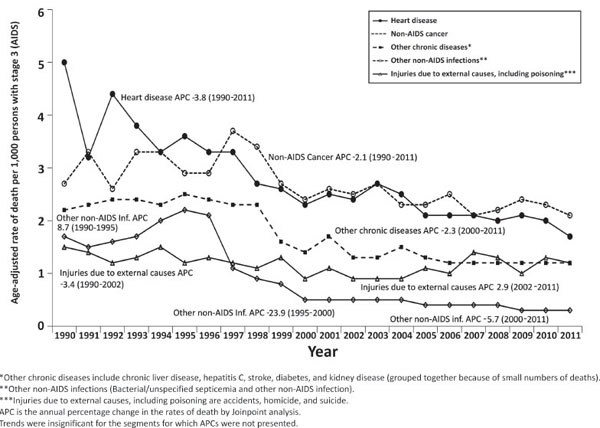
Trends in age-adjusted rates of death due to specific non-HIV-attributable causes among persons with stage 3 classification (AIDS), 23 U.S jurisdictions, 1990-2011.
Trends in Death Rates Among Persons with HIV Infection During 2000-2011
Among persons with HIV infection (with or without AIDS) during 2000-2011, the age-adjusted annual rate of death per 1,000 persons due to HIV-attributable causes decreased by 69% (from 26.4 in 2000 to 8.3 in 2011) (Fig. 3). The rate of death due to non-HIV-attributable-causes decreased by 28% (from 10.5 in 2000 to 7.6 in 2011) (Fig. 2). The percentage of deaths due to non-HIV-attributable causes increased from 25% in 2000 to 48% in 2011. Except injuries due to external causes, the rate of death due to specific non-HIV-attributable causes steadily decreased (Fig. 3). All racial/ethnic groups experienced declines in rates of death due to both HIV-attributable and non-HIV-attributable causes (Fig. 4).
DISCUSSION
Our analysis has revealed that among persons who died from either HIV-attributable or non-HIV-attributable causes, the rate of death was highest among blacks compared to the other racial/ethnic groups. Blacks with HIV infection might not seek, receive, or adhere to HIV care or achieve viral suppression because of lack of health insurance, poverty, drug use, or stigma [19]. The increase in the rate of death due to non-HIV-attributable causes with increasing age is to be expected, but the increase in the rate of death due to HIV-attributable causes with increasing age requires more explanation; it might result from the chronic diseases of advancing age contributing to the risk or severity of complications of HIV infection [19]. Among persons who died of HIV-attributable causes, women experienced a higher rate of death compared with men, consistent with other studies that suggested lower access and adherence to HAART among women [20].
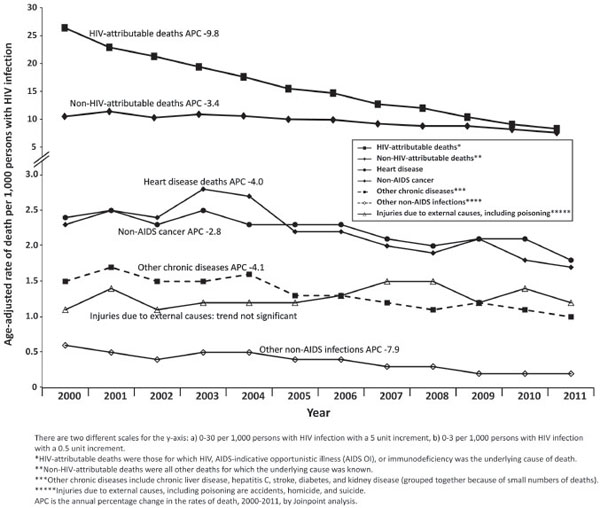
Trends in age-adjusted rates of death due to underlying causes among persons living with HIV infections, 23 U.S jurisdictions, 2000-2011.
Among HIV transmission categories, the highest death rates were among persons with a history of IDU. This is consistent with other reports that found that persons with a history of IDU were more likely to have co-morbid conditions, including viral hepatitis B and C and had a higher all-cause death rate than persons without IDU [21, 22].
The leading non-HIV-attributable causes of death among persons with HIV infection were heart disease, non-AIDS cancer, other chronic diseases (liver disease, stroke, diabetes, kidney disease), and injury due to external causes, including accidents, homicide, and poisoning – conditions that are also common in the general population. Some of these conditions (e.g., viral hepatitis C, homicide, suicide) are particularly prevalent in populations at increased risk for HIV infection, such as persons with a history of IDU and male-to-male sexual contact [23-25]. Studies have shown that factors that contribute to deaths due to heart disease among persons with HIV include higher prevalence of smoking, HAART-induced hyperlipidemia and chronic immune activation and upregulation of proinflamatory cytokines [9, 12, 26].
Among persons with AIDS during 1990-2011, the rates of death due to HIV-attributable causes and rates of death due to non-HIV-attributable causes both decreased, but to different extents; the decrease in the former was more pronounced than that in the latter. As a result, the percentage of deaths due to HIV-attributable causes decreased, while the percentage of deaths due to non-HIV-attributable causes increased. Although HIV-attributable causes still accounted for most deaths, the percentage of deaths caused by non-HIV-attributable causes among persons with AIDS increased from 11% in 1990 to 43% in 2011. Similarly, the rates of death due to HIV-attributable and non-HIV-attributable causes among persons with HIV infection (with or without AIDS) during 2000-2011 decreased and the percentage of deaths caused by non-HIV-attributable causes increased from 25% in 2000 to 48% in 2011.
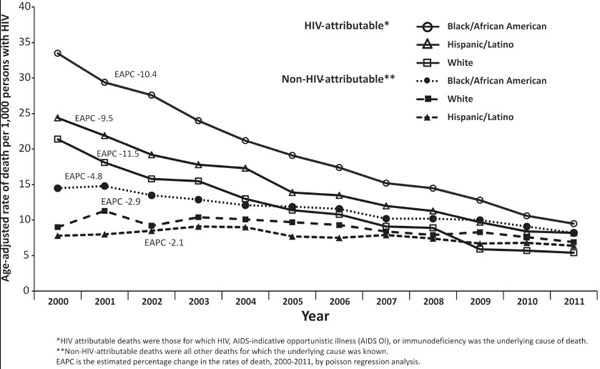
Trends in rates of death due to HIV-attributable and non-HIV-attributable causes by race/ethnicity, 23 U.S jurisdictions, 2000-2011.
These findings are consistent with other studies on causes of death among persons with HIV infection [8-11, 27].The rapid decrease in the rates of death due to HIV-attributable causes in 1996 and 1997 was largely due to the introduction of HAART in 1996. Prophylactic medications for opportunistic infections may also have contributed to this decrease. The continued, albeit slower decline in the rate of death after 1998 may be in part due to newer HAART regimens with better potency, dosing schedules, tolerability, as well as changes in treatment guidelines over the years emphasizing starting HAART at higher CD4 counts [1]. However, the slowing of the rate of decline may reflect obstacles to effective therapy among some persons, including people being unaware of their infection until late in their disease, and failure of others to be linked to care or continuously engaged in care despite being aware of their infection [19]. Of persons diagnosed with HIV infection during 2013 in the 28 jurisdictions with complete reporting of CD4 and viral test results to CDC, 73% and 82% were linked to HIV medical care ≤1 month and ≤3 months after diagnosis, respectively [28]. Of persons diagnosed with HIV infection through the end of 2011 and alive at year-end 2012 in the 28 jurisdictions, only 54% remained in care, and 50% achieved viral suppression [28]. Other barriers include poor access to health care, low educational attainment, social stigma [29], inadequate treatment after diagnosis, difficulty in adherence to medication regimens, and development of viral resistance to therapy. These problems are more common among groups that we found had higher rates of death due to HIV infection–blacks, Hispanics/Latinos, and persons with a history of IDU [30].
Our analyses were subject to some limitations. First, our analyses were based on data from 23 jurisdictions and, therefore, may not be representative of the entire United States as they reported only 59% (592,154) of all HIV diagnoses and 60% (56,257) of all deaths in the United States during 2007-2011. The prevalence of diagnosed HIV infection (persons living with diagnosed HIV per 100,000 population) at the end of 2011 in the study and non-study jurisdictions was 372.5 and 215.4, respectively. The distribution of diagnosis by race/ethnicity in 2007-2011 in the study and non-study jurisdictions was similar, except for Hispanics/Latinos (24% and 17%) and whites (29% and 34%), respectively. Second, there was the possibility of under-reporting of HIV infection because of its stigma and physicians’ desire to protect patient confidentiality [3]. Third, cause-specific death rates may be underestimated because we ascertained the cause of death for only 97% of the deaths in our study population. Fourth, information was not available on prescription of HAART or treatment adherence. Finally, the finding that decreases in the rate of death due to some non-HIV-attributable causes (especially infectious diseases other than AIDS-defining causes, such as septicemia) were parallel to decreases in the rate of death due to HIV-attributable causes in the first few years after the introduction of HAART suggests that some deaths classified as non-HIV-attributable might actually have been HIV-attributable.
CONCLUSION
In conclusion, because HAART has prolonged survival of HIV infected persons by reducing deaths due to HIV-attributable causes [31], more attention should be focused on preventing deaths not attributable to HIV (e.g., non-AIDS cancer, cardiovascular disease, other chronic conditions, accidents, suicide) in the clinical management of HIV-infected persons. For optimal care, and to further decrease mortality, HIV-infected persons should be aware of their infection through testing and obtain care as soon as possible to benefit from the medications that can reduce their risk of death due to HIV. This is in consonance with the recommendation by the Panel on Antiretroviral Guidelines for Adults and Adolescents that patients are diagnosed early in the course of HIV infection so as to initiate therapy early and at any CD4 count [32, 33]. Then, with HIV-attributable causes being less of a threat, HIV-infected persons and their health care providers should watch for and take action to prevent diseases unrelated to HIV that are common in populations at risk of HIV infection, including conditions resulting from smoking and substance use, as well as chronic diseases common in the general population. Finally, they should be alert for possible adverse effects of HAART, so that treatment regimens can be modified if necessary. In recognition of the shift in the distribution of the causes of death among surviving persons with HIV infection, the Infectious Diseases Society of America (IDSA) has emphasized the importance of managing all persons according to standard practices appropriate for their age and sex regardless of HIV status and pay additional attention to complications associated with antiretroviral therapy [25, 34]. In addition, effective programs for linkage and retention in care should address challenges and obstacles to accessing care. Such efforts include outreach, peer navigation, linkage to substance use treatment programs, availability of health insurance, and case management interventions to locate HIV-infected persons, who are unstable in care or not in care at all and form relationships with them and assist them to engage and remain in care [35-37].
APPENDIX
ICD-9/ICD-10 codes for underlying causes of death in persons with diagnosed HIV infection.
| Condition | ICD-9/ICD-10 codes |
|---|---|
| HIV related causes of death | |
| Human immunodeficiency virus (HIV) disease | B20-B24 |
| AIDS-indicative opportunistic illnesses (AIDS OI) | |
| Progressive multifocal leukoencephalopathy | 046.3, A81.2 |
| Cytomegalovirus disease | 078.5, B20.2, B25 |
| Herpes simplex | 054, A60, B00 |
| Various types of pneumonia | 480-486, J12-J18 |
| Tuberculosis | 010-018, A15-A19 |
| Non-tuberculous mycobacteriosis | 031, A31 |
| Candidiasis | 112, B37, B20.4 |
| Coccidioidomycosis | 114, B38 |
| Histoplasmosis | 115, B39 |
| Cryptococcosis | 117.5, B45 |
| Cryptosporidiosis or Isosporiasis | 007.2, A07.2, A07.3 |
| Pneumocystosis | 136.3, B59, B20.6 |
| Toxoplasmosis | 130, B58 |
| Kaposi sarcoma | 173, C46, B21.0 |
| Non-Hodgkin lymphoma, excluding follicular lymphoma | 200.0-200.8, 202.8, C83, C85, B21.1, B21.2 |
| Dementia | 043.1, 290.1, 294.9, 310.9, 323.9, 331.9, 341.9, 348.3, 348.9, 349.9, 049.8, 049.9, 436, B22.0, F02.4, FO6.7, G04.9, G31.8, G31.9, G37.9, G93.4, G93.9, A85.8, A88.8, F03, A86, A89 |
| Wasting | 799.4, 783.2, 783.4, 263.9, 261, B22.2, R63.4, E41, E46, R64, R62 |
| Immunodeficiency | 279.1, 279.3, D84.8, D84.9 |
| Non-HIV-related causes of death | |
| Viral hepatitis C | 070, B15-B19 |
| Chronic liver disease | 571, K70, K73, K74 |
| Other non-AIDS infections | 001-139, 003.1, A02.1, 022.3, A22.7, A26.7, A32.7, 038, A40, A41 |
| Lung cancer | 162, C33, C34 |
| Other non-AIDS cancers | 140-208, C97 |
| Hear disease | 390-398, 402, 404-429, I00-I09, I11, I13, I20-I51 |
| Diabetes | 250, E10-E14 |
| Stroke | 430-438, I60-I69 |
| Kidney disease | N00-N07, N17-N19, N25-N27 |
| Unintentional injury or poisoning (Accidents) | V01-V99, W00-W99, X01-X59, Y85-Y86, E800-E949 |
| Assault (Homicide) | E960-E978, U01-U02, X85-X99, Y00-Y09, Y87.1 |
| Self-harm (suicide) | E950-E959, U03, Y87.0 |
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

