All published articles of this journal are available on ScienceDirect.

HIV-Related Stigma and Serostatus in Homophobic and Serophobic Violence Within LGBTIQA+ Populations: A Systematic Review
Abstract
Introduction
This study synthesizes empirical evidence on how HIV-related content (serostatus, HIV risk indicators, and HIV-related stigma/serophobia) is associated with violence and exclusion within LGBTIQA+ relationships (friendships or romantic relationships) and within LGBTIQA+ contexts (e.g., bars/nightclubs, organizations, and digital platforms). It examines mechanisms of stigmatization linked to HIV-positive status and sexual orientation, manifestations of violence across multiple levels (interpersonal, community, institutional), and consequences for health and well-being.
Methods
A PRISMA 2020-guided systematic review was conducted in PubMed, Scopus, Web of Science, and SciELO (January 1, 2019–June 30, 2025). Only empirical studies published within this period constitute the systematic evidence base and are included in the PRISMA flow diagram and the NHLBI/NIH quality appraisal (empirical evidence set: n = 22). Separately, an integrative conceptual component (2003–2018) and one contemporary conceptual paper were used exclusively for contextualization and interpretive sensitization. These conceptual sources are reported independently, are not counted in the PRISMA totals, and are not assessed with the NIH tool.
Results
Across the empirical evidence base, HIV-related content (serostatus, risk indicators, or HIV-related stigma) was unevenly operationalized. In the subset of studies that explicitly addressed HIV-related variables, HIV-related stigma and serostatus were reported alongside relational tensions and intracommunity exclusion in LGBTIQA+ relationships and social/digital contexts. In parallel, consistent evidence indicates that heteronormative and cisnormative discourses, as well as hegemonic masculinity, permeate LGBTIQA+ relationships and settings, shaping hierarchies of desirability and belonging.
Discussion
Within the included empirical literature, HIV-related stigma and serostatus, when explicitly measured, are associated with patterns of intracommunity exclusion and relational violence, particularly when intersecting with other vulnerabilities (gender, race, poverty). Given that most studies are cross-sectional and HIV-related variables were inconsistently measured, these findings should be interpreted as associative and context-dependent rather than causal. The review challenges homogenizing notions of an LGBTIQA+ “community” and provides research directions for the design of interventions (evaluation, implementation, and assessment) that address heteronormative practices and discourses within LGBTIQA+ adult relationships and contexts.
Conclusion
HIV-related stigma and serostatus, when explicitly measured, are associated with intracommunity exclusion and relational violence, particularly at the intersection of other vulnerabilities. Future research should specifically examine serophobia within LGBTIQA+ populations, develop interventions grounded in the U=U principle, and adopt longitudinal designs to establish causal pathways. The exclusive use of Spanish and English, the restricted time frame (2019–2025), and reliance on indexed literature may have led to the exclusion of relevant studies (including grey literature).
1.. INTRODUCTION
LGBTIQA+ people continue to face widespread violence and discrimination driven by sexual prejudice and stigma, which are expressed through exclusion and physical and symbolic aggression [1, 2]. When these processes intersect with class, race, and gender, they can be understood as structural violence operating on a continuum ranging from everyday insults and threats to serious forms of harm [3, 4]. Alongside research focusing on perpetrators, such as external hegemonic (heterosexual) individuals and institutions, increasing attention has been paid to violence occurring between people who identify as LGBTIQA+ in intimate, friendship, community, or digital contexts [4, 5].
Within these LGBTIQA+ spaces and relationships, stigma and processes of violence related to HIV diagnosis and perception (serophobia) are relevant, as they operate as a historically moralized layer of guilt and perceived contagion, reactivating narratives of danger and deviance long associated with sexual and gender dissidence [6, 7, 8, 9]. Serophobia involves fear, rejection, and discrimination towards people living with HIV, often reproducing moral stereotypes about sexuality and guilt and interacting with pre-existing inequalities of gender, race, and class [7, 10, 11]. In practice, HIV status and diagnosis can become symbolic markers that reorganize intimacy, belonging, and desire within LGBTIQA+ spaces [12, 13], not only through risk frameworks but also through practices and discourses of heteronormativity and masculinity [4, 14, 15, 16, 17, 18].
Heteronormative and masculinizing practices and discourses [19, 20], which naturalize a narrow model of legitimate gender, embodiment, and intimacy, not only operate among hegemonic or heterosexual people but also permeate and reproduce themselves within the spaces and relationships of LGBTIQA+ people, shaping relational expectations, desirability, and the creation of boundaries [7, 21, 22, 23]. One avenue through which this occurs has been conceptualized as internalized homophobia, defined as the incorporation of stigmatizing beliefs about non-heterosexuality that can be directed toward oneself and other LGBTIQA+ people [24, 25, 26]. This has been linked to poorer mental health and increased vulnerability [27] and can intersect with HIV-related stigma when serostatus becomes a signal for moral judgment, fear, avoidance, and devaluation [9, 28, 29].
Despite increased attention to violence against LGBTIQA+ individuals and HIV-related stigma, these publications are often empirically disconnected. There are studies on violence against LGBTIQA+ people in LGBTIQA+ spaces and relationships and studies on HIV stigma, but few directly measure serostatus or serophobia as a mechanism operating in LGBTIQA+ spaces and relationships [12, 30, 31, 32].
1.1. Gap and Contribution
Although violence in LGBTIQA+ spaces and relationships and HIV-related stigma have received increasing attention, empirical work that directly operationalizes HIV serostatus, HIV risk indicators, or serophobia within intracommunity violence processes remains limited. Most studies in the systematic evidence set focus on heteronormative/cisnormative hierarchies, minority stress, and intraminority stigma without consistently measuring HIV-related variables. To address this gap without over-centering HIV as a “core explanatory variable,” this review adopts a conservative reporting rule: HIV-related findings are summarized only when primary studies explicitly measured and analyzed HIV-related content, and any broader interpretive propositions are presented as context-dependent and hypothesis-generating rather than causal.
1.2. Objectives
This article presents a systematic review of empirical studies (2019–2025) on processes of violence in LGBTIQA+ relationships and contexts, complemented by an integrative review of seminal works (2003–2018) to clarify key conceptual advances related to stigma, serophobia, and heterocisnormative violence. The study aims to: (1) describe the forms of LGBTIQA+ violence associated with HIV-related content (seropositivity, diagnosis, risk, or stigma); (2) identify the psychosocial mechanisms through which internalized homophobia and serophobia may operate in these contexts; and (3) synthesize the implications for prevention, clinical and community intervention, and policy, including U=U-based strategies.
2. METHODOLOGY
This manuscript follows a hybrid evidence-synthesis design comprising two analytically distinct components: (1) a PRISMA 2020-guided systematic review restricted to empirical studies published between January 1, 2019, and June 30, 2025 (systematic empirical evidence set: n = 22); and (2) an integrative conceptual component used exclusively for contextualization and interpretive sensitization (2003–2018 plus one contemporary conceptual paper). Throughout the manuscript, the term 'systematic review' refers only to the empirical evidence set (n = 22), which is the only dataset included in the PRISMA flow diagram and eligible for NIH appraisal. Conceptual sources are presented separately, are not included in the PRISMA totals, and do not contribute empirical findings to the Results section.
2.1. Inclusion and Exclusion Criteria
Inclusion criteria for the systematic review (empirical evidence set; included in PRISMA and eligible for appraisal) were: (1) empirical quantitative, qualitative, or mixed-methods studies published between January 1, 2019, and June 30, 2025; (2) examination of violence, exclusion, or intraminority stigma occurring within LGBTIQA+ groups, relationships, or contexts (e.g., intimate, friendship, community, or digital settings); (3) sufficient methodological description to support appraisal and thematic synthesis; and (4) publication in English or Spanish.
Within this empirical evidence set, HIV-related content (serostatus, HIV risk indicators, or HIV-related stigma/serophobia) was treated as a focused analytic dimension during extraction and synthesis. Accordingly, HIV-related findings are reported conservatively and only when primary studies explicitly measured and/or analyzed HIV-related variables.
Criteria for the integrative conceptual component (not included in PRISMA; not part of the empirical evidence set) were: (a) key theoretical and earlier empirical works (2003–2018) identified via snowballing to support the conceptual grounding of stigma, serophobia, heterocisnormativity, and intracommunity violence; and (b) one contemporary conceptual paper [33] retained to strengthen interpretive sensitization given the scarcity of empirical studies explicitly measuring serophobia. These sources were not counted as systematic evidence, were not included in the PRISMA flow diagram, and were not subjected to the NIH quality appraisal.
Exclusion criteria for the systematic review were: (1) reviews, editorials/commentaries, conceptual/theoretical papers, and other non-empirical reports; (2) studies lacking a methodological description; (3) studies addressing prejudice or attitudes without examining violence, exclusion, or intraminority stigma processes; and (4) studies focusing exclusively on heterosexual/cisgender perpetrators without analyzing violence occurring within LGBTIQA+ relationships or contexts.
2.2. Bibliographic Search
An exhaustive search was conducted in the following databases: Scopus, Web of Science (WOS), PubMed, and SciELO. The search strategy combined keywords related to violence, the LGBTIQA+ community, and intracommunity contexts. The search was carried out between January and March 2025, with the last update on June 30, 2025. Combinations of descriptors and free-text terms in English and Spanish were used, for example: ('HIV' OR 'HIV-positive' OR 'serostatus') AND ('LGBTIQA+' OR 'sexual minorities' OR 'gender minorities') AND ('intimate partner violence' OR 'violence' OR 'stigma' OR 'discrimination') AND ('community' OR 'intracommunity').
Scopus, Web of Science, SciELO, and PubMed were selected to balance coverage across the health and social sciences and to increase the likelihood of identifying Latin American literature alongside clinical and epidemiological studies. Embase, PsycINFO, and CINAHL were not included because of substantial overlap with Scopus and Web of Science and because preliminary scoping searches indicated minimal additional retrieval relevant to the review focus. This decision is acknowledged as a methodological limitation, and future reviews may benefit from incorporating these databases to expand disciplinary coverage.
2.3. Study Selection
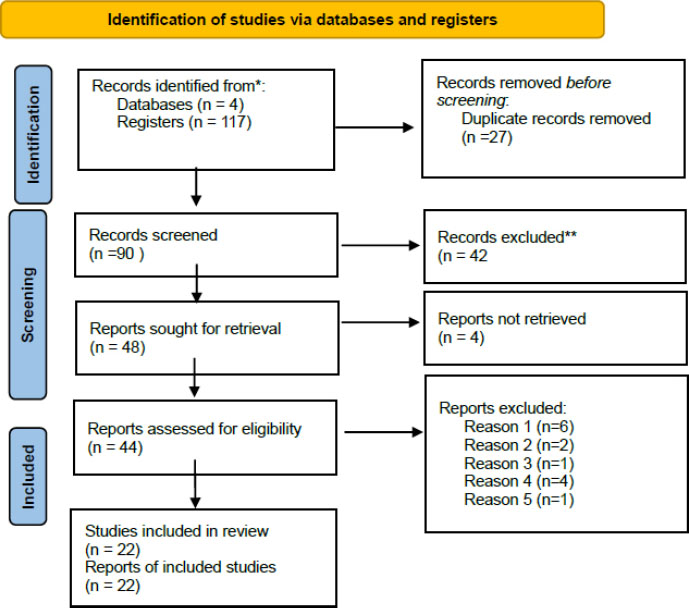
A systematic search of Scopus, Web of Science, PubMed, and SciELO yielded 117 records. After removing 27 duplicates, 90 records were screened by title and abstract, and 42 were excluded. Full texts were sought for 48 reports; 4 could not be retrieved. The remaining 44 full-text reports were assessed for eligibility; 22 were excluded based on predefined criteria, leaving 22 empirical studies included in the systematic review (Figure 1). For full PRISMA 2020 compliance and to avoid misinterpretation of this hybrid design, Figure 1 reports only the identification, screening, and inclusion counts for the empirical systematic evidence set (2019–2025; n = 22). The integrative conceptual sources (2003–2018) and the additional contemporary conceptual paper are reported separately and are not included in the PRISMA totals.
The PRISMA flow diagram and the 22 included records refer exclusively to the empirical studies (2019–2025) that make up the systematic empirical evidence base. In addition, one contemporary conceptual article [33] was retained as part of the integrative conceptual component to support interpretive sensitization, but it was not included in the PRISMA diagram, counted within the systematic evidence set, or evaluated with the NIH tool. For transparency, the integrative conceptual sources are presented separately in the Results section.
2.4. Assessment
Quality assessment was conducted using a two-tiered strategy aligned with the evidence status and study design. First, the NHLBI (NIH) quality assessment tool for observational cohort and cross-sectional studies [34] was applied exclusively to the subset of included empirical studies with quantitative observational designs for which this instrument is methodologically appropriate. Each item was rated as Yes (1), Partially Met (0.5), No (0), or Not Applicable (NA). Items rated as “partially met” were operationalized as 0.5 to increase discriminatory sensitivity at the cutoff points. This pragmatic fractional score was applied only within the quantitative observational subset, was prespecified for this review, and was resolved by consensus to avoid inflation of fully met criteria. Total scores were calculated as the sum of applicable items (excluding NA), and studies were classified as Good, Acceptable, or Poor using the predefined cut-offs indicated in Table 1.
| ID | Authors and Year | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | Q13 | Q14 | TOTAL | SCORE |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 01 | Beam & Wellman (2024) [40] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 12 | GOOD |
| 02 | Convertino et al. (2021) [41] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 11 | GOOD |
| 03 | Frederick et al. (2022) [42] | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 0.5 | 10.5 | GOOD |
| 04 | González & Sönmez (2021) [43] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 12 | GOOD |
| 05 | Henn et al. (2019) [44] | 1 | 1 | 0 | 1 | 0 | NA | NA | 1 | 1 | 0 | 1 | 0 | 1 | 0.5 | 8.5 | GOOD |
| 06 | Mijas et al. (2020) [45] | 1 | 1 | 0 | 1 | 0 | NA | NA | 1 | 1 | 0 | 1 | 0 | 1 | 0.5 | 8.5 | GOOD |
| 07 | Mijas et al. (2024) [46] | 1 | 1 | 0 | 1 | 0 | NA | NA | 0 | 1 | 0 | 1 | 0 | 1 | 0.5 | 7.5 | GOOD |
| 08 | Rustagi et al. (2023) | 1 | 1 | 0.5 | 1 | 0 | NA | NA | 1 | 1 | 0 | 0.5 | NA | NA | 1 | 7.0 | GOOD |
| 09 | Schmidt et al. (2022) [47] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | NA | 0.5 | 6.5 | FAIR |
| 10 | Shepherd et al. (2024) | 1 | 1 | 1 | 1 | 0 | NA | NA | 1 | 1 | 0 | 1 | NA | NA | 1 | 8.0 | GOOD |
| 11 | Sommantico et al. (2023) [48] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | NA | NA | 0 | 6.0 | FAIR |
| 12 | Stephenson et al. (2022) | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | NA | NA | 1 | 7.0 | GOOD |
| 13 | Teschlade et al. (2023) [49] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | NA | 1 | 0 | 1 | NA | NA | 0 | 5.0 | FAIR |
| 14 | Whitehead et al. (2020) [50] | 1 | 1 | 1 | 1 | 0 | NA | 1 | 0 | 1 | 0 | 1 | 0 | NA | 0 | 7.0 | GOOD |
Second, qualitative, mixed-methods, experimental, and conceptual records were not eligible for the NHLBI observational tool. These records were therefore appraised using a structured complementary rubric focused on methodological transparency and credibility (sampling and recruitment, data generation, analytic procedure, reflexivity/positionality, ethics where applicable, and traceability of claims to data). The complementary rubric used the same 0/0.5/1 scoring logic and produced a normalized percentage score based on applicable items only. Importantly, these complementary appraisals were used solely as a sensitivity check to contextualize confidence in the thematic synthesis; they did not affect PRISMA counts, were not pooled with NIH scores, and were not used to exclude studies from the empirical evidence base.
The contemporary conceptual paper [33] was therefore excluded from the NIH appraisal and was instead reviewed using a narrative relevance-and-rigour check focused on: (a) conceptual relevance to the phenomenon under review (stigma/violence mechanisms), (b) clarity and coherence of the analytic argument, and (c) interpretive contribution to sensitizing concepts used in the thematic synthesis. This ensured methodological coherence while preserving transparency regarding the distinct evidentiary status of conceptual sources.
Items rated as partially met were scored as 0.5 to increase discriminative sensitivity across heterogeneous reporting. This conservative fractional scoring was applied only to the observational quantitative subset for which the NIH tool is appropriate and was discussed between reviewers to ensure consistency. Fractional scoring (0.5) for “partially met” items is not specified in the original NHLBI/NIH instrument; it was adopted as a transparent, conservative operational decision to differentiate borderline compliance while avoiding inflation of fully met criteria (for examples of similar pragmatic scoring decisions in evidence syntheses). Fractional scoring was applied only within the observational quantitative subset for which the NIH tool is methodologically appropriate, and scoring decisions were resolved by consensus.
Based on the total score, studies were classified as: (1) high quality: 7.0 points or more; (2) moderate quality: 5.0 to 6.5 points; and (3) low quality: less than 5.0 points (Table 1).
Two reviewers independently assessed the methodological quality of each study. Discrepancies were resolved through discussion and consensus and, when necessary, by consultation with a third reviewer. This process ensured consistency in scoring and minimized subjectivity in quality evaluation.
The theoretical/conceptual article [33] was not submitted to the NHLBI/NIH tool, as it is designed for empirical observational studies and its application to conceptual texts would be methodologically inappropriate [35, 36]. Instead, the paper was evaluated through a narrative verification of relevance and conceptual rigour, applied independently by two members of the team and resolved by consensus, focusing on: (a) its direct relevance to the phenomenon under review (mechanisms of stigma/serophobia and their articulation with violence in LGBTIQA+ contexts); (b) the clarity, internal coherence, and argumentative traceability of its analytical proposal; (c) the explicitness of concepts, assumptions, and delimitations (scope, conditions of applicability, and limits); and (d) its interpretive contribution as a source of “sensitizing concepts” to refine the delimitation of themes in the thematic synthesis. To preserve the coherence of the evidence status, this evaluation did not generate scores or quality ratings, and the conceptual text was used exclusively to strengthen interpretative coherence and the definition of mechanisms when the empirical operationalization of serophobia was scarce, without supporting statements presented as empirical findings in the results section.
2.5. Data Extraction
Data extraction followed the PRISMA protocol [37, 38]. Extracted information from each study included: authors, year, country, study design, sample characteristics, conceptual framework, methodology used, types of violence examined, and key findings.
2.6. Data Analysis
A Reflexive Thematic Analysis (RTA) was implemented to analyze the selected articles, following the methodological guidelines of Braun and Clarke (2006) [39], using a deductive and semantic approach. This methodological approach was grounded in social constructionist epistemology, recognizing that themes emerge from both pre-existing theoretical frameworks and inductive patterns identified in the data.
2.7. Research Team and Positionality
The analysis was led by the principal investigator, with expertise in LGBTIQA+ research and qualitative methodologies. The team also included two additional researchers. This multidisciplinary configuration aimed to minimize interpretative bias and strengthen analytical credibility.
2.8. Systematic Analysis Process
Reflexive Thematic Analysis (RTA) [39] was conducted as an interpretive synthesis across two analytically distinct textual datasets: (1) the empirical systematic evidence set (n = 22), from which findings, analytic claims, and reported mechanisms were coded; and (2) the integrative conceptual component, including one contemporary conceptual paper [33], which was coded separately for sensitizing concepts and interpretive propositions rather than empirical associations. To avoid interpretive inflation, conceptual material was used to refine theme boundaries, clarify mechanisms as interpretive models, and strengthen conceptual coherence, but empirical claims in the Results are grounded only in the systematic evidence set. This two-stream analytic strategy preserves the integrity of the PRISMA/NIH procedures while allowing the thematic synthesis to remain conceptually robust in a field where direct empirical operationalization of serophobia remains scarce.
The RTA was conducted in five stages, as proposed by Braun and Clarke (2006) [39]:
- Familiarization with the data: reading and re-reading the empirical evidence set (n=22) and the integrative conceptual material (n=1, reported separately).
- Generation of initial codes: identifying patterns in how the studies conceptualized and measured violence.
- Theme identification: grouping similar methodological and conceptual approaches across studies.
- Theme definition and naming: refining themes to capture key patterns in the literature.
- Final report: synthesizing findings into coherent themes presented in this review.
2.9. Rigor and Triangulation Strategies
Open coding was employed to identify emerging patterns in the conceptual frameworks and methodological approaches of the studies, which were subsequently grouped into categories and subcategories based on conceptual similarities. For data triangulation, a research team composed of the principal investigator and three additional researchers was assembled. The analytical process was conducted using Atlas.ti, which was selected for its capacity to manage academic texts, build categories, and create coding networks, essential for capturing thematic patterns in the reviewed literature.
2.10. Epistemological Considerations
The analysis was positioned from a critical social constructionist perspective, recognizing that the concepts of violence, gender, and the LGBTIQA+ community are contextually situated social constructions. This perspective informed the interpretation of findings with sensitivity to the diversity of experiences within LGBTIQA+ populations, while avoiding essentialist generalizations.
2.11. Methodological Limitations
Given the heterogeneity of study designs, populations, and operationalizations of violence and HIV-related variables, the synthesis is subject to high methodological variability and potential interpretive bias. The absence of preregistered protocols (PROSPERO/OSF) also represents a limitation that future research should address.
For transparency, observational quantitative studies eligible for NIH appraisal are summarized in the methodological evaluation table (Table 1). Empirical studies included in the PRISMA evidence set are reported in the characteristics table (Table 2). Integrative conceptual sources are reported separately (Table 3) and were not subjected to NIH scoring.
| Author/Year | Country(ies) | Study Design | Sample Type | Type of violence/stigma | HIV / serological status/health |
|---|---|---|---|---|---|
| Beam et al. (2022) [40] | United States | Experimental quantitative | Gay men (MSM) | Intracommunity prejudice | No HIV/health data |
| Convertino et al. (2021) [41] | United States | Observational quantitative | LGB individuals (sexual minorities) | Body stigma | Mental/body health |
| del Río et al. (2023) [51] | Spain | Qualitative | LGBTIQA+ individuals using social networks and dating apps | Sissyphobia and exclusion | Indirect health (no HIV) |
| Henn et al. (2019) [44] | Germany | Observational quantitative | Heterosexual, lesbian, and bisexual women | Body-related discrimination | Mental/body health |
| Shepherd et al. (2024) | United States, England, Canada, Australia, South Africa, Philippines, Mexico | Observational quantitative | Gay men and other sexual minorities who use dating apps | Intraminority stigma | Well-being (no HIV data) |
| Øverlien (2020) [52] | Norway and Sweden | Qualitative | LGBTQ+ youth in same-sex relationships | Intimate partner violence | Physical/mental health |
| Montaño et al. (2022) [53] | Philippines | Qualitative | Same-sex couples (LGBTQ+) | Intimate partner violence | Mental health |
| Reis et al. (2023) [54] | Portugal | Qualitative | Men in same-sex relationships who have experienced IPV | Intimate partner violence | Physical/mental health |
| Mayeza (2024) [55] | South Africa | Qualitative | LGBTIQA+ youth in same-sex relationships | Sexual violence | Sexual/mental health |
| Teschlade et al. (2023) [49] | Germany | Exploratory qualitative | Families with LGBTQ+ members | Family discrimination | Indirect health |
| Rustagi et al. (2023) | United States | Observational quantitative | Gay and bisexual men (sexual minority men) | Intimate partner violence | HIV risk (no serostatus) |
| Mijas et al. (2020) [45] | Poland | Observational quantitative | Gay and bisexual men in the bear subculture | Weight stigma | Mental/physical health |
| Mijas et al. (2024) [46] | Poland | Observational quantitative | Men in the bear subculture | Weight stigma | Body/mental health |
| Sommantico et al. (2023) [48] | Italy | Observational quantitative | Lesbian and gay couples | Internalized sexual stigma | Mental health risk |
| Odoi (2021) [56] | Ghana | Qualitative | Men who have sex with men / local dissident identities | Homophobic violence | Contextual HIV risk |
| Moodley et al. (2021) [57] | South Africa | Qualitative | Gay men in same-sex relationships | Intimate partner violence | Physical/mental health |
| González et al. (2021) [43] | Spain | Observational quantitative | Same-sex couples (men and women) | Labour-market discrimination | Structural health determinants |
| Whitehead et al. (2020) [50] | Canada | Observational quantitative | People in same-sex and different-sex relationships (UCR cases) | Intimate partner violence | Physical health |
| Frederick et al. (2022) [42] | United States | Mixed-methods | LGBTQ+ college students | Body/gender stigma | Physical/mental health |
| Schmidt et al. (2022) [47] | Germany | Observational quantitative | Gay and heterosexual men | Body image pressure | Mental/body health |
| Stephenson et al. (2022) | South Africa and Namibia | Observational quantitative | 220 couples of men who have sex with men (MSM) | Intimate partner violence | HIV serostatus and risk |
| Atuk (2020) [13] | Turkey | Qualitative | LGBTIQA+ individuals using apps and geosocial networks | Homonormative exclusion | HIV/STI sexual health |
| del Río et al. (2023) [51] | Spain | Qualitative | LGBTIQA+ individuals using social networks and dating apps | Sissyphobia and exclusion | Indirect health (no HIV) |
| Øverlien (2020) [52] | Norway and Sweden | Qualitative | LGBTQ+ youth in same-sex relationships | Intimate partner violence | Physical/mental health |
| Montaño et al. (2022) [53] | Philippines | Qualitative | Same-sex couples (LGBTQ+) | Intimate partner violence | Mental health |
| Reis et al. (2023) [54] | Portugal | Qualitative | Men in same-sex relationships who have experienced IPV | Intimate partner violence | Physical/mental health |
| Mayeza (2024) [55] | South Africa | Qualitative | LGBTIQA+ youth in same-sex relationships | Sexual violence | Sexual/mental health |
| Teschlade et al. (2023) [49] | Germany | Exploratory qualitative | Families with LGBTQ+ members | Family discrimination | Indirect health |
| Odoi (2021) [56] | Ghana | Qualitative | Men who have sex with men / local dissident identities | Homophobic violence | Contextual HIV risk |
| Moodley et al. (2021) [57] | South Africa | Qualitative | Gay men in same-sex relationships | Intimate partner violence | Physical/mental health |
| Atuk (2020) [13] | Turkey | Qualitative | LGBTIQA+ individuals using apps and geosocial networks | Homonormative exclusion | HIV/STI sexual health |
| Author/Year | Country(ies) | Study Design | Sample Type | Type of violence/stigma | HIV / serological status/health |
|---|---|---|---|---|---|
| Westman (2024) [33] | South Africa | Theoretical | Conceptual analysis | Corrective sexual violence | Sexual/reproductive health |
3. RESULTS
3.1. Analytic Corpus and Evidentiary Status
The Results report findings grounded in the systematic empirical evidence base included in the PRISMA flow diagram (n = 22). Given the limited number of studies explicitly operationalizing serophobia and HIV-related mechanisms within LGBTIQA+ relationships and contexts, we additionally incorporated one contemporary conceptual paper [33] as part of the integrative conceptual component. This article was coded separately within the reflexive thematic synthesis to provide sensitizing concepts and support interpretive coherence when empirical operationalization was sparse. Importantly, it was not treated as empirical evidence, was not counted within the PRISMA totals, and was not subjected to NIH quality appraisal. Accordingly, any claims presented as empirical findings in this section are derived from the systematic evidence set, while the conceptual paper is used only to refine theme boundaries and interpretive models.
3.2. Descriptive Results
Only a small subset of studies explicitly incorporated HIV serostatus and/or HIV-related variables into their analyses, and only one examined serophobia directly [12, 13, 58, 59]. In the remaining studies, HIV appeared indirectly (e.g., as contextual prevalence, as part of sexual health framing, or as an unstated background factor within minority stress narratives). During data extraction, all mentions of HIV, serostatus, risk, or stigma were coded deductively to ensure consistent identification of relevant content across studies. To minimize interpretive bias, coding decisions were discussed among team members and cross-checked against the original constructs reported in each study.
3.3. HIV-related Content: Empirical Coverage and Reporting Rules
Across the empirical evidence set (n = 22) and one additional conceptual source used only for sensitization (n = 1; Tables 2 and 3), three studies incorporated HIV variables directly into their design or outcomes (HIV serostatus and/or HIV risk/sexual health indicators) [13, 58, 59]. In addition, one qualitative study referenced HIV risk contextually without reporting serostatus or a dedicated HIV stigma measure [56]. In the remaining studies, health appeared mainly as mental and physical well-being outcomes, structural health determinants, or indirect health references without explicit HIV measurement.
To minimize interpretive inflation in this review, HIV-related findings in the Results are reported only when (a) HIV serostatus, HIV risk, or sexual health indicators were explicitly measured and analyzed, or (b) HIV risk was explicitly discussed in the primary study's findings. When HIV was absent or only implicit, it was not treated as an explanatory mechanism.
3.4. Descriptive Synthesis of Included Studies
3.4.1. Geographic Distribution and Knowledge Location
The included literature is geographically concentrated in the Global North, with multiple studies conducted in the United States and Canada, and a substantial cluster in Western/Central Europe (Germany, Spain, Italy, Portugal, Norway/Sweden, Poland) [40, 41, 43, 45, 47, 50, 51, 52, 54, 60]. A smaller set of studies was conducted in the Global South (South Africa, Ghana, Namibia, the Philippines, Turkey) [51, 52, 56, 60]. One multi-country study included sites spanning both the Global North and Global South [60]. Overall, this distribution indicates that empirical knowledge about LGBTIQA+ violence processes, and especially about HIV-related mechanisms within them, is produced unevenly across different regions.
3.5. Study Designs
Of the 22 included records (Table 2), observational quantitative designs predominated, followed by qualitative studies. However, the complete set (n = 23) also included one experimental quantitative study [40], one mixed-methods study [42], and one theoretical/conceptual record [33]. Consistent with the systematic review design profile, the empirical evidence base contained no longitudinal studies and no evaluated interventions. In addition to the empirical set, one contemporary conceptual paper [33] was included in the integrative conceptual component and analyzed separately for interpretive sensitization; it is therefore not counted as part of the systematic evidence base.
3.6. Populations and Sampling Focus
Most studies focused on gay men and/or MSM, including men in couples [54, 57, 59], sexual minority men [40, 58], and men in specific sub-communities (e.g., the bear subculture) [45, 46]. Several studies examined same-sex couples more broadly [43, 48, 53] or included mixed same-sex/different-sex relationship samples in administrative or case-based designs [50]. LGBTQ+ youth were represented in qualitative studies [52, 55]. Trans and non-binary experiences were not foregrounded as distinct analytic strata in Table 2 and tended to be subsumed within broader LGBTQ+ categories, limiting specificity for gender-diverse populations.
3.7. Contexts and Types of Violence/Stigma Examined
The included studies operationalized violence and stigma in the relationships and contexts of LGBTIQA+ individuals across multiple contexts: (a) intimate partner violence (IPV) in same-sex relationships and couples [50, 52, 53, 54, 55, 57, 58, 59]; (b) digital/social network and dating-app contexts, emphasizing exclusion, intraminority stigma, and homonormative filtering [13, 51, 60]; (c) body- and aesthetics-related symbolic violence, including weight stigma, body image pressure, and body-related discrimination [41, 42, 44, 45, 46, 47]; and (d) internalized sexual stigma and related intracommunity tensions [48], discrimination within families [49], and broader structural discrimination relevant to well-being and health determinants [43].
3.8. Reflexive Thematic Analysis
Drawing on the primary studies, four relevant themes emerge: (1) intimate partner violence in the context of heterocisnormativity, (2) stigma on social networks and dating apps, (3) internal tensions within the community, and (4) symbolic violence related to bodies and aesthetic standards [48, 50, 55, 59]. This thematic approach makes it possible to render visible both overt and covert forms of violence. The following section develops each of these themes. However, one additional, hypothesis-generating interpretive theme emerged in relation to the review focus: within the small subset of studies that explicitly measured HIV serostatus, HIV risk, and/or HIV-related stigma, HIV-related content was described as being associated with the co-occurrence or perceived intensification of intracommunity exclusion and relational tensions in LGBTIQA+ contexts and relationships [13, 56, 58, 59]. Given the predominance of cross-sectional designs and the uneven operationalization of HIV-related variables, this pattern should be interpreted as associative, context-dependent, and not causal.
3.8.1. Hierarchies of Desirability and Serophobic Exclusion
First, serophobia and hierarchies of desirability emerge as key factors structuring discrimination within the community. Multiple qualitative and quantitative studies converge in indicating that HIV-positive status was described as reshaping, and being associated with shifts in, sexual desirability and affective legitimacy within some queer couples and social circles, particularly in qualitative accounts and in studies focusing on dating-app contexts. As noted by Shepherd et al. (2024) [60]:
“Intraminority stigma can manifest in forms, from blatant rejection or aggression to microaggressions such as expressing ‘preferences’ on profiles or blocking users based on identity”. (Shepherd et al., 2024, p. 5)
This redefinition is not neutral; rather, it generates explicit dynamics of rejection, humiliation, and exclusion, particularly visible in digital social spaces such as dating apps. The explicit distinction between “healthy/clean” profiles and those labeled as “poz/unhealthy” illustrates how seropositivity is discursively constructed as both a symbolic and a health-related threat. In Atuk’s (2020) study [13], the author describes how Hornet suggests hashtags such as “#nofem, #notrans, #masculineonly, #masc” to filter out undesired bodies and expressions.
This form of discrimination may co-occur with and be experienced as more severe when intersecting with other stigmas, such as internalized homophobia, policing of masculinity, and prejudices related to age, race, and body size. Thus, serophobia becomes inscribed in a moral economy that values “bodily purity” and equates viral undetectability with sexual and affective legitimacy. Ethnographic studies conducted in contexts as diverse as Istanbul and Latinx communities in the United States have confirmed that these exclusionary practices severely erode intracommunity cohesion, contributing to experiences of exclusion and internalized stigma.
3.8.2. Minority Stress, Couple Conflict, and Violence
Second, research focused on minority stress shows how an HIV diagnosis and its associated stigma are associated with heightened interpersonal conflict within same-sex couples. A key study conducted with 440 male couples in South Africa and Namibia found that dyadic differences in internalized homophobia and experiences of stigma were associated with higher odds of reported physical, sexual, and emotional violence. Specifically, the study identified that when one partner experiences higher levels of discrimination than the other, the probability of bidirectional violence rises significantly (OR = 1.78). In this context, serostatus and HIV-related stigma were discussed as potentially contributing to fears of transmission, suspicions of infidelity, and guilt-related dynamics, which in turn may co-occur with, or be reported alongside, relationship conflict in the subset of studies that explicitly examined HIV-related variables. These negative emotions may manifest in dynamics of control and aggression, undermining effective communication and increasing the risk of violent conflict. Stephenson et al. (2022) [59] note:
“Among this sample of male couples, IPV was associated with differences in the experiences of internalized homonegativity and enacted stigma.”
Moreover, recent studies highlight that in contexts with high HIV prevalence, such as several regions of sub-Saharan Africa, intracommunity serophobia may be more appropriately understood as a contextual correlate that can co-occur with other minority stress processes and may be implicated in the perceived escalation of tensions in specific settings where HIV is epidemiologically salient and/or explicitly measured. In these settings, serological stigma may function as a contextual amplifier of other minority stress processes where HIV-related variables are explicitly measured.
3.8.3. Synergies between HIV, Substance use, Risk Practices, and Legal Frameworks
A third dimension concerns the co-occurrence of HIV-related vulnerability, substance use, and relationship violence within the empirical literature, particularly in settings where HIV is epidemiologically salient [55, 57, 59, 61]. Within these contexts, authors discuss how coping strategies, relationship stressors, and barriers to care may interact with violence-related risk, underscoring the practical importance of integrating violence assessment into prevention and care pathways. As Rustagi et al. (2023) [58] state:
“The negative outcomes of IPV in MSM, such as increased HIV risk due to an increase in condomless anal sex, have not been fully examined.”
Finally, it is essential to recognize how criminalizing legal environments may contribute to heightened concealment concerns and may be associated with stronger stigma-related stressors and intracommunity serological stigma. In more than sixty countries where these relationships remain criminalized, serophobia deepens due to fear of rejection and institutional persecution. Recent observations from the Committee on the Elimination of Discrimination against Women (CEDAW) highlight that repressive laws create a hostile environment that encourages concealment of HIV status even within LGBTIQA+ communities, increasing vulnerability to violence and significantly reducing access to basic health and justice services.
Conversely, in countries where decriminalization policies and anti-discrimination laws have advanced, comparative accounts suggest that more protective legal environments may be linked to lower reported stigma; however, the included evidence base does not allow causal inference regarding either community stigma or intracommunity violence. This contrast underscores the importance of promoting legal reforms and inclusive policies as a crucial strategy for reducing serophobia and comprehensively preventing violence within LGBTIQA+ communities.
3.9. Interpretive Synthesis
Taken together, the empirical evidence suggests that HIV-related stigma, when explicitly measured, and the attributed meanings of serostatus may be implicated in the way boundaries of desirability and belonging are negotiated within some LGBTIQA+ contexts. Importantly, the reviewed literature does not establish temporal ordering or causal pathways. Rather, the available findings support an associative interpretation in which stigma, concealment concerns, relationship stressors, and conflict may co-occur, particularly in settings where HIV is epidemiologically salient and/or where HIV-related variables were directly assessed [13, 58, 59].
Accordingly, the practical implications of this review should be framed as prevention-oriented and hypothesis-informed. Interventions may benefit from integrating U=U-informed education, stigma-reduction strategies, and couples- or community-focused support, while recognizing that the current evidence base is predominantly cross-sectional and methodologically heterogeneous. In parallel, peer-led initiatives on digital platforms and in physical spaces may be useful for challenging moralized “clean/dirty” logics and promoting inclusion, but intervention effectiveness remains an empirical question that requires evaluation studies.
Ultimately, the effective integration of education, health services, legal reform, and community participation emerges as a viable path to decouple serophobia from violence, thereby building truly inclusive and safe spaces for LGBTIQA+ people living with HIV.
4. DISCUSSION
The results presented here suggest that HIV-related stigma and the attributed meaning of serostatus may co-occur with relational tensions and exclusionary practices in some LGBTIQA+ contexts, particularly in studies conducted in high-prevalence settings or those that explicitly assessed HIV-related variables [12, 16, 57]. However, it is essential to clarify from the outset that HIV was not a variable measured systematically throughout the reviewed literature. HIV-related variables appeared unevenly, and only a small subset of studies directly incorporated serostatus, HIV risk, or serophobia. For this reason, in this review, HIV should be understood as an emerging cross-cutting interpretive theme rather than a central axis operationalized consistently across the included studies. However, the findings show that HIV status is articulated within the contexts and relationships of LGBTIQA+ individuals.
The results show a fundamental finding: LGBTIQA+ violence in LGBTIQA+ relationships and contexts is consistently described as being structured by, and associated with, the permeability of heteronormative and masculinizing discourses within LGBTIQA+ relationships and spaces [61, 62, 63, 64]. Across the included studies, violence and exclusion in LGBTIQA+ spaces and relationships were repeatedly organized through hierarchies of desirability, gender expression, and embodiment based on heteronormative and masculinizing discourses and practices (control of femininity, “acceptable” masculinity, body regulation), which also align with racialized and class-based norms of value and belonging [65, 66, 67]. This demonstrates how LGBTIQA+ spaces, although they function as a refuge from external stigma, can also reproduce internal stratifications and new forms of control and aggression [25, 68, 69]. In this sense, the review raises an initial tension regarding the notion of the “LGBTIQA+ community” as a homogeneous group [64]. However, the review shows that it is instead a field of social relations structured by internal differences that can translate into symbolic, digital, and relational violence. This is in line with current research in gender and LGBTIQA+ studies, which questions the notion of an “LGBTIQA+ community” and proposes the concept of an LGBTIQA+ population, given its heterogeneity [3].
In relation to these dynamics of violence in LGBTIQA+ relationships and spaces, HIV emerges in a more localized and indirect way. In the subset of studies that included HIV serostatus, the risk of contracting HIV, or that were conducted in contexts where HIV is epidemiologically relevant, serostatus appears to be related to psychosocial and relational tensions in couple dynamics and in spaces culturally defined as LGBTIQA+ (clubs, organizations, marches) [12, 57, 59]. Therefore, the findings suggest that serological stigma may intersect with existing hierarchies of gender expression, body size, race, and class and may be implicated in the perceived intensification of vulnerability among those already positioned at the margins of “desirable” queer subjectivities [14, 22, 67]. However, given the limited number of studies explicitly measuring serophobia, this pattern should be interpreted cautiously and as associative rather than causal. Nevertheless, the findings show that the symbolic and cultural framework, body regulation, surveillance of masculinity, and exclusion based on LGBTIQA+ stigma provide a context in which serological stigma can be reproduced, even when it is not directly named or enacted.
This dynamic is especially visible in digital social spaces, as several studies show how serophobia is integrated into platform practices: profiles explicitly marked as “clean only,” blocks, filters, and the circulation of warnings or rumours [12, 13, 51, 60]. Even when serophobia is not the primary outcome, the logic of “bodily purity” and “responsible sexuality” appears as a recurring moral language through which people are classified as safe/desirable versus risky/undesirable [12, 13, 51, 60, 65, 66]. In this context, HIV-positive status can be interpreted as a stigmatizing label that reorganizes access to intimacy, recognition, and belonging. It is important to note that the review also confirms a critical empirical gap: there is very little quantitative evidence directly comparing exposure to violence among HIV-positive and HIV-negative LGBTIQA+ individuals or examining how HIV status influences exclusion and the escalation of violence in relationships and social interactions. This absence limits what can be concluded about the magnitude or causal direction, but it reinforces the argument that serophobia remains understudied in research on violence arising in social spaces and relationships among LGBTIQA+ individuals.
From a theoretical standpoint, these findings support the refinement of minority stress and stigma frameworks by emphasizing that serostigma, when present, can accumulate with pre-existing stressors related to sexual and gender minorities and translate into relational dynamics such as concealment, fear of disclosure, and control within intimate relationships [8, 9, 12, 70]. In the context of couples, this accumulation may contribute to communication breakdown, health status-related power asymmetries, and threats linked to disclosure or moral blame, especially in conditions of social vulnerability and limited access to supportive care [12, 70]. However, given the predominance of cross-sectional designs, these pathways are more appropriately interpreted as an interpretive model than as a longitudinally demonstrated sequence.
Although only a small subset of the included studies directly measured HIV-related variables or examined serophobia, the available evidence suggests that an HIV-positive diagnosis (or the attributed meaning of serostatus) may operate as a hierarchical marker that reorganizes intimacy, belonging, and desirability within LGBTIQA+ networks, potentially amplifying pre-existing intracommunity tensions structured by heteronormative and masculinizing hierarchies (e.g., “acceptable” masculinity, body regulation, and moralized notions of “purity”). Consistent with the reporting rules adopted in this review, this pattern should be understood as a cross-cutting interpretive theme grounded in limited empirical coverage, rather than as a consistently operationalized causal variable.
Therefore, the practical implications of this review can be expressed concisely. First, it is necessary to strengthen public health and community interventions that integrate the “undetectable = untransmittable” (U=U) principle into testing, counselling, and treatment services and translate it into accessible messages in LGBTIQA+ spaces, including digital platforms [71]. When U=U is absent or communicated in a fragmented way, fear of transmission tends to be filled with moralizing narratives and discourses of “self-protection” that often legitimize exclusion [72, 73, 74, 75]. Second, although intervention evidence remains limited, the reviewed literature supports the need for psychosocial strategies that address minority stress, stigma management, and relational dynamics in couples, along with peer-led community work that challenges hierarchies of desirability and the “clean/dirty” dichotomy in apps and in-person settings [50, 59, 76, 77]. Finally, in Chile and Latin America, where structural inequality, health systems, and conservative moral discourses converge, the intersection between heteronormative violence and stigma reproduced in spaces and contexts defined as LGBTIQA+ reinforces the urgency of policies that address stigma both outside and within LGBTIQA+ spaces, including the explicit recognition of serophobia as a relevant form of discrimination [13, 17, 18, 61].
5. LIMITATIONS
A critical limitation is that HIV-related variables were not measured consistently across the empirical evidence base. Therefore, HIV-related stigma/serostatus can only be discussed as a limited-coverage, hypothesis-generating interpretive pattern grounded in a small subset of studies, and it should not be interpreted as a demonstrated causal mechanism.
This review has limitations associated with the methodological process. It includes only indexed literature published in English and Spanish, which may have excluded relevant evidence (including grey literature and works in Portuguese or other languages), thereby reducing its representativeness [20, 27, 29, 37, 67]. Methodological heterogeneity among predominantly cross-sectional designs, varied measures, and uneven quality limited comparability and prevented formal assessments of publication bias and meta-analytic synthesis [39, 41, 78, 79]. Finally, the lack of longitudinal and evaluated intervention studies limits the ability to examine trajectories before and after diagnosis and to assess how stigma and violence change over time in relation to treatment access and U=U dissemination [13, 57, 58, 59].
Figure 1 presents a PRISMA 2020 flow diagram adapted from the diagrams proposed by Boers [ 81 ], Mayo-Wilson et al. [ 82 ], and Stovold et al. [ 83 ]. Reason 1: Studies older than five years. Reason 2: Accessibility to full-text. Reason 3: No methodology. Reason 4: Legibility. No thematic relationship; this was assessed by a research assistant and a co-investigator. Reason 5: Theoretical article. This last excluded article was added during the analysis process.
CONCLUSION
This review shows that violence emerging in LGBTIQA+ relationships and contexts is consistently shaped by the permeability of heteronormative and masculinizing discourses, producing hierarchies of desirability, belonging, and legitimacy within spaces that are often considered cohesive or uniformly protective [3, 63, 80]. HIV-related stigma emerged as a cross-cutting interpretive theme in the literature, but empirical evidence remains limited, as few studies directly measured serostatus or serophobia [12, 56, 59].
A clear empirical gap persists: future studies should specifically examine serophobia within LGBTIQA+ populations, measure how serological stigma shapes exclusion and violence across offline and digital settings, and develop and evaluate interventions grounded in the U=U principle alongside community- and couples-based strategies to reduce stigma and harm [50, 75, 77, 80]. Strengthening these lines of research and intervention is essential for building safer and more equitable environments for LGBTIQA+ people living with HIV.
AUTHOR’S CONTRIBUTION
The author conceived and designed the study, conducted the literature search, performed the analysis, and wrote the manuscript.
LIST OF ABBREVIATIONS
| VIH | = Virus de la inmunodeficiencia humana |
| HIV | = Human Immunodeficiency Virus |
| LGBTIQA+ | = Lesbian, Gay, Bisexual, Trans, Intersex, Queer/Questioning, Asexual and other identities |
| IPV | = Intimate Partner Violence |
| PRISMA | = Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| NIH | = National Institutes of Health |
| RTA | = Reflexive Thematic Analysis |
| MSM | = Men who have sex with men |
| SPD | = Subsecretaría de Prevención del Delito |
| MOVILH | = Movimiento de Integración y Liberación Homosexual |
| U | = U = Undetectable = Untransmittable |
| WOS | = Web of Science |
| OECD | = Organisation for Economic Co-operation and Development |
| UNDP | = United Nations Development Programme |
| USAID | = United States Agency for International Development |
AVAILABILITY OF DATA AND MATERIALS
All the data and supportive information is provided within the article.
FUNDING
This work was supported by the Chilean National Agency for Research and Development (Agencia Nacional de Investigación y Desarrollo, ANID), FONDECYT Project No. 11251504.
ACKNOWLEDGEMENTS
The authors would like to thank the individuals and organizations that contributed to the development of this review, as well as the communities and activists working to combat serophobia and homophobic violence.

