All published articles of this journal are available on ScienceDirect.

Pre-exposure Prophylaxis Outcomes During the COVID-19 Lockdown Period among Women in the North-West Province, South Africa: A Retrospective Analysis
Authors Info & Affiliations
Abstract
Background
Oral Pre-Exposure Prophylaxis (PrEP) is a proven method for preventing HIV among women, including adolescent girls and young women who are categorised as priority populations due to a higher risk of HIV acquisition. However, the COVID-19 lockdown disrupted access to healthcare services, including those for HIV prevention and treatment. This study aimed to assess changes in PrEP outcomes before and during the COVID-19 lockdown period among women in the North-West Province, South Africa.
Methods
We conducted a retrospective analysis of programme data collected by TB HIV Care from December 2018 to December 2021 in the Dr Kenneth Kaunda District to assess changes in PrEP initiation, uptake, and adherence before (December 2018 - February 2020) and during (March 2020 - December 2021) the COVID-19 pandemic among women aged 16 years and above. The Department of Health electronic (Excel) register was used to collect data. The overdispersion tests conducted on three datasets, PrEP initiation, uptake, and adherence, showed significant overdispersion (with p-values less than 0.05). This indicates that the Negative Binomial regression model is more appropriate for these datasets. Additionally, the adherence dataset contained a high percentage of zero outcomes, underscoring the need for a zero-inflated model to address the excess zeros. Consequently, we implemented Bayesian negative binomial regression models for both the PrEP initiation and uptake datasets and a Bayesian Zero-Inflated Negative Binomial (ZINB) regression model for the adherence dataset.
Results
A total of 1339 women involved in transactional sex were counselled and offered PrEP services. Out of these, 776 were initiated on PrEP with a mean age of 33 years. PrEP initiation demonstrated a significant trend before the lockdown, an immediate effect during the lockdown, and a shift in trends afterwards, with all 95% credible intervals excluding zero. This suggests that the pandemic both disrupted and altered PrEP initiation patterns. The intervention did not lead to a significant increase in PrEP uptake among clients who returned for HIV testing within one month, as the 95% credible intervals included the value of 1. Nonetheless, there was a slight positive trend over time that was statistically significant, indicating a modest increase in uptake. Additionally, none of the estimated parameters for adherence achieved statistical significance, suggesting that the intervention did not have a meaningful impact on adherence levels.
Conclusion
The study revealed a decline in the initiation, uptake, and adherence to PrEP during the COVID-19 lockdown, although services were maintained through innovative interventions. These findings underscore the necessity for more innovative strategies to enhance PrEP outcomes, ensure effective HIV control, and prepare for potential future pandemics.
1. INTRODUCTION
South Africa bears the highest prevalence of HIV, with close to 8 million South Africans living with HIV [1]. According to the Sixth South African HIV Prevalence, Incidence, and Behaviour Survey (SABSSM VI), in 2022, North-West Province was recorded as the fifth highest in terms of HIV prevalence rate in the country, standing at 12.3% [2]. Additionally, new HIV infections continue to increase in this Province. For instance, in 2022, the infection rate was at 4.5% among adolescents aged 15-19, which was higher than in 2017 (3.2%) [2]. Oral Pre-Exposure Prophylaxis (PrEP), a single pill containing tenofovir disoproxil fumarate and emtricitabine, is proven to reduce the risk of HIV transmission during sexual intercourse by about 99% when taken as required [3]. Nevertheless, maintaining consistent and effective use of PrEP among women remains a significant challenge [4]. Previous literature studies on PrEP implementation among young African women showed higher levels of PrEP initiation but rapid declines in adherence levels within the first six to twelve months [5-8]. Additionally, another South African study carried out in KwaZulu-Natal Province among women, focused on PrEP initiation and adherence, found that of the 262 participants who started oral PrEP, 67 had stopped using it within three months, and 94 had discontinued by the sixth month [9].
Several factors serve as barriers to sustained PrEP outcomes among women, as highlighted in previous studies. For example, it is believed that women, especially young women, often discontinue the use of PrEP due to being shamed by their partners and family members who may not comprehend their higher risk of HIV acquisition [10-12]. Other factors resulting in PrEP secrecy and low adherence are the anticipation of negative reactions from partners, like mistrust, stigma, and relationship dissolution [13]. Highlighting significant challenges faced by women in adhering to oral PrEP. The onset of the Coronavirus disease 2019 (COVID-19) in South Africa also played a pivotal role in reducing healthcare services among key and priority population groups, particularly during the lockdown period, which was imposed in March 2020 [14]. During these times, essential services, including the provision of oral PrEP among women, were severely impacted. To illustrate these impacts, one study was carried out in the Western Cape Province, South Africa, on PrEP prescription refill visits during COVID-19 among pregnant women. The study revealed that during the lockdown period, missed PrEP visits rose sharply, with a 63% increase at the one-month visit and a 55% increase at the three-month visit, resulting in 57% of women missing their PrEP appointments overall during this time [15]. Another study conducted in Eswatini assessed the impact of COVID-19 on PrEP uptake and initiation among young women [16]. The study found that more women initiated PrEP after Covid-19 (n=55%) than during the pandemic (45%) [16]. Moreover, the number of clients who were on retention was also lower, especially among the younger group aged 15-29 years old [16]. This was similar to a systematic review, which reported that the majority of studies included reported a decline in discontinuation in PrEP uptake during the pandemic [17].
The World Health Organization (WHO) published guidelines for continuing with essential services like HIV and other health services via innovative approaches in the quest to mitigate the COVID-19 impacts on healthcare service delivery [18]. As with other vital HIV prevention services, the provision of PrEP was continued during the lockdown period in countries, including South Africa, by the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) [19]. Innovative approaches like implementing virtual options for client initiations, refills, and check-ins, decentralising PrEP through community delivery, and moving to multi-month dispensing were utilised during the pandemic [20]. However, significant evidence on the effects of COVID-19 on HIV care, treatment, and prevention services from both observational and randomised controlled trial studies is still lacking [21]. Thus, we aimed to assess the changes in PrEP outcomes before and during the COVID-19 lockdown period among women in the North-West Province of South Africa. Additionally, the objective was to evaluate the impact of the COVID-19 lockdown period on HIV PrEP services to prepare for potential future pandemics.
2. METHODS
2.1. Study Population and Setting
This study retrospectively collected and analyzed routine program data collected by TB HIV Care from December 2018 to December 2021 among women in the Dr Kenneth Kaunda District. The TB HIV Care program was pioneered in offering PrEP to HIV-negative female sex workers as part of a government-led programme, and also to provide life-saving ART, adherence support, and comprehensive sexual and reproductive health services [22]. Data was collected via the PrEP clinical form obtained from the Department of Health, South Africa. The study population included 1339 women involved in transactional sex who were counselled and offered PrEP services; however, only a total of 776 were initiated on PrEP. Participants were all females aged 16 years and above from the three sub-districts (Matlosana, Maquasi Hills, and JB Marks) of the Dr Kenneth Kaunda District [23]. The HIV prevalence in the mentioned District is 11.9% among all ages [2].
2.2. Data Measurements
We assessed changes in PrEP initiation, uptake, and adherence before (Dec 2018 - Feb 2020) and during (Mar 2020—Dec 2021) the COVID-19 lockdown period. Initiation was defined as the number of people commencing PrEP; uptake as the proportion of clients receiving HIV testing services and offered PrEP for a one-month return; and adherence as the number of people remaining between months two and four, as it has been recorded. The mentioned data was already de-identified from the TB HIV Care program and included other variables like HIV testing, STI screening and treatment, and ART initiations, but the current study focused on PrEP outcomes.
2.3. Description of the PrEP Innovation Interventions
Before the emergence of COVID-19, the TB HIV Care programme utilised a mobile clinic vehicle to provide sexual reproductive health services, including PrEP, to women involved in transactional sex in the Dr Kenneth Kaunda District, North-West Province [23]. These services were provided to the service users within communities in different hotspots by multiple healthcare providers, including professional nurses, case managers, and peer educators from TB HIV Care [23]. During the COVID-19 lockdown period, the normal service provisions were disrupted due to the implemented measures to reduce the spread of the virus [24]. However, TB HIV Care continued with service provisions through the mobile clinic and innovations like social media platforms, including WhatsApp applications and Facebook pages [23]. These platforms were utilized for HIV services, including the scheduling of PrEP appointments, follow-ups, tracings, and the provision of psychosocial support to service users [23].
2.4. Statistical Analysis
The Poisson and negative binomial models are the two most widely employed methods for analysing count data. Furthermore, the Zero-Inflated Poisson (ZIP) model, first introduced by Lambert [25], has gained significant popularity for analysing count data with a substantial number of zeros. However, the ZIP model may encounter challenges when non-zero counts are over-dispersed relative to the Poisson distribution. Overdispersion occurs when the observed variance of the response variable (the count data) exceeds the mean. This situation violates a fundamental assumption of the Poisson distribution, where the mean and variance are expected to be equal. In these cases, Zero-Inflated Negative Binomial (ZINB) models can be more effective, providing more reliable parameter estimates when non-zero counts show overdispersion, unlike the ZIP model [26]. For example, ZINB models have been utilised to analyse spatiotemporal patterns in inpatient hospitalizations and COVID-19 death counts, highlighting the relationship between social vulnerability and health outcomes [27].
2.5. Bayesian Analysis
Using Bayesian negative binomial regression models and ZINB regression models allows for incorporating prior information and using Markov Chain Monte Carlo (MCMC) methods for parameter estimation. This methodology is particularly advantageous for addressing complex data structures [28].
We employed the No-U-Turn Sampler (NUTS) and a Hamiltonian Monte Carlo algorithm to fit all models using the brms package (version 2.18.0). Our analysis involved running NUTS with four chains, each consisting of 8,000 iterations. The initial 3,000 iterations of each chain were designated as the warm-up phase and subsequently discarded. As a result, we effectively utilized four parallel chains, with 8,000 iterations per chain, ensuring that the first 3,000 iterations were only used for warming up. Additionally, we reported important metrics for each parameter, including posterior estimates of Incidence Rate Ratio [IRR], corresponding 95% credible intervals, and Effective Sample Sizes (ESS). All analyses were conducted using R version 4.4.2 [29] with the brms package version 2.22 for Bayesian ZINB regression.
2.6. Model Specification
The overdispersion tests performed on three datasets, PrEP initiation, uptake, and adherence, revealed significant overdispersion, with p-values considerably below 0.05. This finding indicates that the Negative Binomial regression model is more suitable than the Poisson regression model for analysing these datasets. Moreover, the adherence dataset shows a high percentage of zero outcomes (51.35%), indicating excess zeros. This suggests the need for a zero-inflated model to address the data's excess zeros and the overdispersion effectively. As a result, we employed Bayesian negative binomial regression models to analyse the initiation and uptake of PrEP. Additionally, we utilised a Bayesian ZINB regression model to examine adherence to PrEP.
2.7. Ethical Considerations
As this study was retrospective, written informed consent from participants was not required. However, ethical approval for the study (REC-2435-2023) was granted by the University of Johannesburg Research Ethics Committee (UJREC). In addition, permission letters were obtained from both the North-West Department of Health (NWDoH) and the TB HIV Care program to access and utilize the program data [23].
3. RESULTS
3.1. Characteristics of the Population
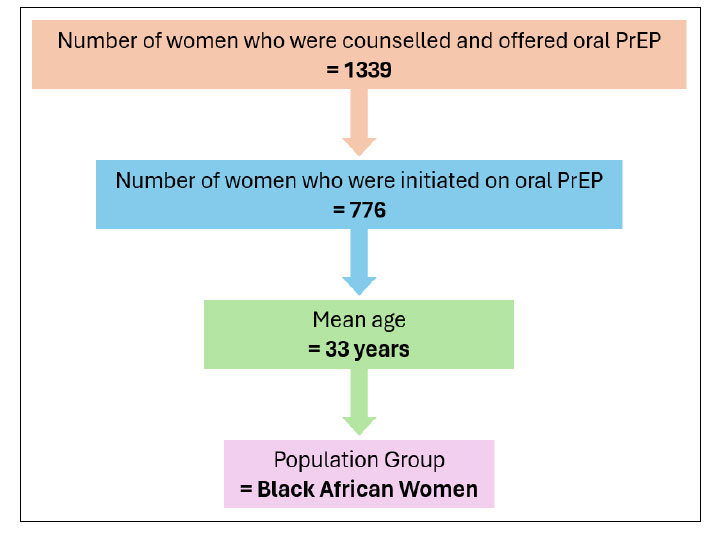
The flow diagram (Fig. 1) below shows the characteristics of the included sample, as well as Table 1 below. A total of 1339 women involved in transactional sex were counselled and offered PrEP services. Out of these, 776 were initiated on PrEP (42%; n=326 before Covid-19 and 58%; n=450 during Covid-19), with a mean age of 33 years (Fig. 1, Table 1).
| Dec 2018-Dec 2021 | Before the COVID-19 Period (Dec 2018 – Feb 2020) | During the COVID-19 Period (Mar 2020 – Dec 2021) | |
|---|---|---|---|
| n (%) | n (%) | ||
| PrEP initiation | 776 | 326 (42) | 450 (58) |
| PrEP uptake | 236 | 68 (29) | 168 (71) |
| PrEP Adherence | 52 | 15 (29) | 37 (71) |
| Age in Years | - | - | - |
| 16-18 | 28 | 8 (29) | 20 (71) |
| 19-24 | 230 | 95 (41) | 135 (59) |
| 25-34 | 363 | 144 (40) | 219 (60) |
| 35+ | 155 | 69 (45) | 86 (55) |
Characteristics of the included sample.
Moreover, Figure 2 below displays the three time series plots with a red dashed vertical line indicating the point where social media interventions were implemented for service continuity, which was around March 2020. Looking at the first plot, which indicates the commencement of PrEP, a stable number of women who have agreed to be enrolled in a programme is observed, with slight fluctuations from December 2018 – January 2020. However, during the lockdown period, there was a noticeable decrease in specifying the impact of COVID-19 restrictions on HIV Prep services.
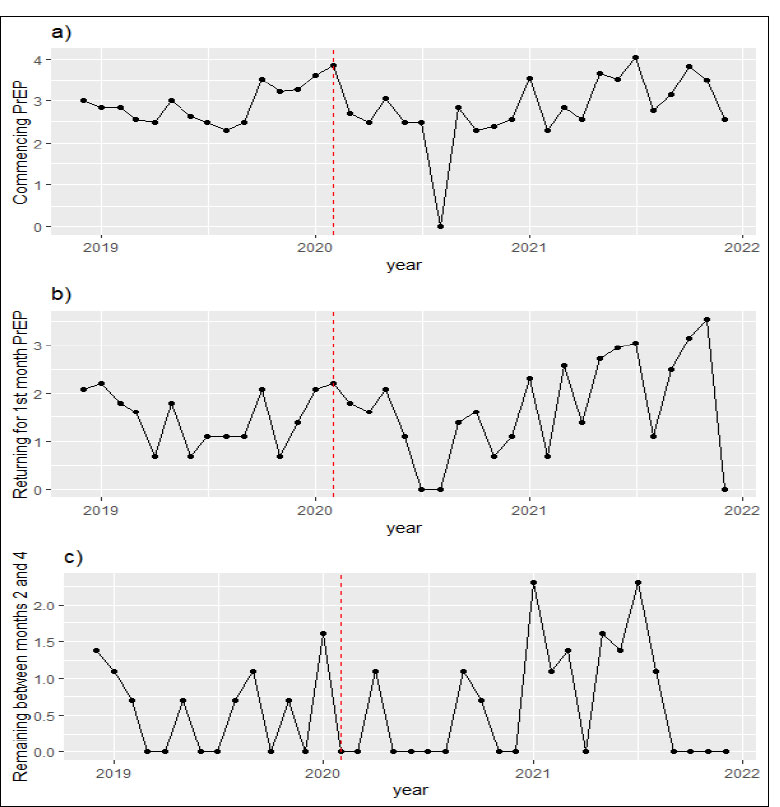
Changes in PrEP outcomes during the COVID-19 lockdown period. All three outcome variables were log-transformed.
The second plot shows no clear increase or decrease in the PrEP uptake, suggesting what has been highlighted in previous literature regarding the low uptake rates. Moreover, after the lockdown measures, the number of women returning for 1st month was gradually increasing, illustrating a positive effect following a sharp decrease during COVID-19. Furthermore, the last plot shows very low and consistent values, with minimal difference. However, there was a slight increase in the number of women remaining between months 2 and 4 during the implementation of social media platforms, which was followed by substantial fluctuations.
3.2. Bayesian Negative Binomial and ZINB Regression Model Results
This section presents the results from the Bayesian negative binomial regression models and the Bayesian ZINB regression model presented in Tables 2, 3, and 4.
| Variable | Estimate (SE) | IRR (95% CI) | ESS (Bulk/Tail) |
|---|---|---|---|
| Intercept | -32.39 (8.63) | 8.60 × 10−15 (2.16 × 10−22, 1.37 × 10−7) | 8530 / 5401 |
| Time | 0.00 (0.00) | 1.002 (1.001, 1.003) | 8543 / 5387 |
| Intervention | 0.06 (2.01) | 1.061 (0.020, 53.571) | 4306 / 4460 |
| Time × Intervention | -0.00 (0.00) | 0.9999 (0.9997, 1.0002) | 4420 / 4700 |
| Shape Parameter | 5.62 (1.82) | - | 4174 / 4389 |
| Variable | Estimate (SE) | IRR (95% CI) | ESS (Bulk/Tail) |
|---|---|---|---|
| Intercept | -40.87 (15.18) | 1.77 × 10−18 (1.22 × 10−31, 2.43 × 10−5) | 15604 / 9706 |
| Time | 0.00 (0.00) | 1.002 (1.001, 1.004) | 15655 / 9709 |
| Intervention | -0.21 (1.99) | 0.811 (0.017, 41.065) | 7622 / 8137 |
| Time × Intervention | -0.00 (0.00) | 0.9999 (0.9997, 1.0002) | 7870 / 8433 |
| Shape Parameter | 1.83 (0.60) | - | 7288 / 7306 |
| Variable | Estimate (SE) | IRR (95% CI) | ESS (Bulk/Tail) |
|---|---|---|---|
| Intercept | -31.54 (32.16) | 2.01 × 10−14 (1.94 × 10−41, 7.21 × 1014) | 11869 / 10105 |
| Zi Intercept | -0.86 (0.96) | 0.422 (0.030, 1.364) | 5659 / 4444 |
| Time | 0.00 (0.00) | 1.002 (0.998, 1.005) | 11831 / 10247 |
| Intervention | -0.01 (1.00) | 0.992 (0.143, 7.022) | 9074 / 10369 |
| Time × Intervention | -0.00 (0.00) | 0.9999 (0.9998, 1.0001) | 11088 / 12275 |
| Shape Parameter | 6.81 (18.93) | - | 5008 / 6280 |
Table 2 demonstrates that all estimated parameters, intercept, time, intervention, and the interaction between time and intervention, are significant at the alpha level of 0.05, as their 95% credible intervals do not contain zero.
The results presented in Table 3 demonstrate that the intervention did not have a significant effect on the uptake of PrEP among clients returning for HIV testing services within one month. The credible intervals for the intervention and the interaction term (time × intervention) include 1, indicating no significant change. Nevertheless, the time variable reveals a small yet statistically significant positive effect, suggesting a modest increase in PrEP uptake over time.
Table 4 displays the Bayesian model for adherence, focusing on individuals engaged between months two and four. The results show that none of the estimated parameters are statistically significant at the 0.05 alpha level, as the credible intervals for the intercept, zero-inflation intercept, time, intervention, and their interaction include the value of 1. Overall, the intervention did not significantly impact adherence.
Lastly, the credible interval for the intervention parameter in the PrEP initiation and uptake datasets is notably wide. This is primarily due to the relatively small sample size in our study, which contributes to increased uncertainty in the parameter estimates. Nonetheless, it is important to recognize that Bayesian analysis effectively captures this uncertainty, highlighting one of its key advantages.
In all three tables (Tables 2-4), we assessed the R-hat values to evaluate convergence, and all values were below 1.01, indicating successful convergence of the models. Furthermore, the ESS for all key parameters surpassed 1,000, providing confidence in the reliability of our estimates.
4. DISCUSSION
This study aimed to evaluate the changes in PrEP outcomes, specifically initiation, uptake, and adherence, following the implementation of innovative interventions during the lockdown period. Several authors have conjectured on how the lockdown restrictions have brought new opportunities to implement novel initiatives that were previously thought to be unfeasible. We found a substantial decrease in PrEP initiation, uptake, and adherence during the implementation of the COVID-19 restriction measures, which highlights the adjustment difficulties faced by the South African healthcare system. Challenges such as staff shortages and increased workload for the community healthcare workers, including additional responsibilities like COVID-19 screening, testing, medication delivery, and administrative duties, impacted the overall healthcare services [30].
In response to the aforementioned challenges, innovative initiatives, including the adaptation of social media platforms, were employed to facilitate the provision of PrEP services. Nonetheless, the findings of this study indicate that these innovative interventions did not yield a statistically significant impact on PrEP outcomes, particularly in terms of adherence. In line with the study findings, Rosen et al. 2020 also reported high rates of PrEP discontinuation and loss to follow-up among existing cohorts within the first year of the pandemic [31]. This suggests a need to employ interventions to support PrEP adherence and continuation, particularly during the first two months of initiation [32]. On the other hand, a Zimbabwean study by Matambanadzo et al. 2021 reported that the COVID-19 lockdown measures did not affect the PrEP services [33]. The study reveals that the adaptations of the differentiated service delivery among female sex workers led to a large increase in PrEP initiation compared to before the pandemic [33].
The mentioned discrepancies might be from contextual factors like organizational, community, participants’ demographics, and socio-economic factors, which play a crucial role in the success or failure of implementing innovative interventions [34]. Concerning the PrEP uptake, this study revealed that the employed innovative interventions had no statistically significant effect on the individuals returning for month one. These findings are corroborated by a cross-sectional study in Eswatini by Ginindza et al. 2024 on the impact of COVID-19 on PrEP uptake and retention [16]. In that study, they found that the PrEP uptake was primarily low during the lockdown period due to the implemented mitigation measures [16]. Another, uptake decelerations were also observed in a modelling study where they assessed the changes in PrEP use and coverage during the COVID-19 pandemic in Germany [35]. In this study, the authors have identified significant (p<0.01) decelerating effects of the first- and second COVID-19 lockdowns on PrEP uptake in April 2020 and December 2020 [35], which highlights the negative impact of the pandemic.
Interestingly, the current study found time to have a small yet statistically significant positive effect, suggesting a modest increase in PrEP uptake over time. This could have resulted from the easing of the lockdown restrictions. Similar results were found where the interrupted time series analysis was used to assess the impact of COVID-19 lockdowns on the HIV prevention and treatment services among key populations [36]. The study indicated that as the programs started to adjust and adapt to the restrictions, there was a steady recovery in service engagement, especially among men who have sex with men and female sex workers [36]. With these illustrations, we aim to offer invaluable lessons from the underprepared healthcare systems during the pandemic, which can be considered to prepare for future outbreaks.
5. STRENGTHS AND LIMITATIONS
This study has a few limitations; for example, secondary data depends on the accuracy of the original data collected, which may be compromised during the gathering or compilation process. Also, the strain of the pandemic may have led to less rigorous data collection, resulting in missing, inaccurate, or underreported information. The study findings have shown the need to improve crisis resilience in South Africa by expanding mobile clinics and telehealth services, partnering with local organizations to reduce stigma, ensuring ongoing funding for PrEP during emergencies, and implementing real-time data systems to identify service gaps. Moreover, the outcomes have revealed that future preparedness for HIV prevention must focus on pandemic-ready strategies like PrEP stockpiles and improved telehealth infrastructure. While current research has limitations, including small sample sizes, it is essential to urge policymakers to integrate PrEP into Universal Health Coverage (UHC) and emergency response frameworks to enhance public health resilience.
CONCLUSION
The study concludes that PrEP initiation, uptake, and adherence significantly decreased during the COVID-19 lockdown despite efforts to maintain services through social media. While the parameters for PrEP initiation showed statistical significance, the intervention had no significant effect on adherence. The modest increase in PrEP uptake over time highlights a need for more innovative strategies to improve outcomes. Overall, the findings emphasize the importance of developing effective interventions to enhance PrEP services to achieve better HIV control and prepare for future public health challenges.
AUTHORS’ CONTRIBUTIONS
The authors confirm contribution to the paper as follows: L.L.O., R.N.P.M., and E.P.: Conceptualised and designed the study and reviewed the literature; L.L.O. and H.M.: Prepared and cleaned the data for analysis under the supervision of YAS; Y.A.S.: Analysed the data with LT; L.L.O.: Wrote the first draft of the manuscript; R.N.P.M., E.P., Y.A.S., and L.T.: Supervised and reviewed the paper. All authors have read and agreed to the submission of the manuscript for possible publication.
LIST OF ABBREVIATIONS
| ART | = Antiretroviral Therapy/Treatment |
| COVID-19 | = Coronavirus Disease 2019 |
| ESS | = Effective Sample Sizes |
| HIV | = Human Immunodeficiency Virus |
| MCMC | = Markov Chain Monte Carlo |
| NUTS | = No-U-Turn Sampler |
| NWDoH | = North-West Department of Health |
| PACER | = Pan-African Centre for Epidemics Research |
| PEPFAR | = U.S. President’s Emergency Plan for AIDS Relief |
| PrEP | = Pre-exposure Prophylaxis |
| SABSSM VI | = Sixth South African HIV Prevalence, Incidence, and Behaviour Survey |
| SAMRC/UJ | = South African Medical Research Council/University of Johannesburg |
| STI | = Sexually Transmitted Infection |
| UJREC | = University of Johannesburg Research Ethics Committee |
| WHO | = World Health Organisation |
| ZINB | = Zero-Inflated Negative Binomial |
| ZIP | = Zero-inflated Poisson |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval for the study (REC-2435-2023) was granted by the University of Johannesburg Research Ethics Committee (UJREC).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
As this study was retrospective, written informed consent from participants was not required.
AVAILABILITY OF DATA AND MATERIALS
All data generated or analysed during this study are included in this published article.
FUNDING
The work reported herein was made possible through funding by the South African Medical Research Council (SAMRC) through its Division of Research Capacity Development under the Mid-Career Scientist Program using funding received from the South African National Treasury (Project Code number: 57035 [SAMRC File ref no: HDID8528/KR/202]). The authors, Refilwe Nancy Phaswana-Mafuya and Edith Phalane, are supported by the above-mentioned grant. This work was conducted under the guidance of the SAMRC/University of Johannesburg (UJ) Pan African Centre for Epidemics Research (PACER) Extramural Unit. The content herein is the authors’ sole responsibility and does not necessarily represent the official views of SAMRC or UJ. This paper also forms part of a PhD study by Lerato Lucia Olifant, whose studies are funded by the Global Excellence Stature 4.0 Scholarship at UJ.
ACKNOWLEDGEMENTS
We thank the TB HIV Care stakeholders for allowing us to access the Organisation and for allowing us to utilise the de-identified program data.

