All published articles of this journal are available on ScienceDirect.

Pre-Exposure Prophylaxis Uptake and Associated Factors Among Key Populations in the Nylon and New Bell Health Districts, Cameroon
Authors Info & Affiliations
Abstract
Introduction
Pre-Exposure Prophylaxis (PrEP) is an effective HIV prevention strategy for populations at high risk, including men who have Sex with men (MSM) and Female Sex Workers (FSW). Despite being a proven HIV prevention tool and its effectiveness, the uptake of PrEP remains low in many settings, including Cameroon, posing challenges to HIV control. This study assessed PrEP uptake and associated factors among key populations in Nylon and New Bell Health Districts of Cameroon.
Methods
A cross-sectional study was conducted among 284 participants (91 MSM and 193 FSW) between January and June 2024, recruited through purposive and snowball sampling. PrEP eligibility was assessed based on self-reported risk behaviors, as outlined in World Health Organization (WHO) guidelines. Data on demographic characteristics, PrEP awareness, and uptake were collected through structured questionnaires. Logistic regression analyses identified factors associated with PrEP uptake.
Results
Among the 220 participants eligible for PrEP, only 62 (28.2%) accepted and were initiated on the medication. Significant predictors of uptake included monthly income above 100,000 FCFA (aOR = 4.37, 95% CI: 1.76–11.5, p = 0.002), MSM status (aOR = 2.97, 95% CI: 1.24–7.30, p = 0.015). Conversely, engaging in condomless sex (aOR = 0.35, 95% CI: 0.15–0.75, p = 0.009), higher education (aOR = 0.36, 95% CI: 0.13–0.92, p = 0.034), and relying on sex as the primary source of income (OR = 0.10, 95% CI: 0.02–0.37, p < 0.001) were negatively associated with PrEP uptake.
Discussion
PrEP uptake in Nylon and New Bell remains suboptimal, reflecting persistent economic, behavioral, and structural barriers. Higher income and MSM status predicted uptake, while condomless sex, sex as a source of income, and higher education were negative factors. Addressing stigma, financial vulnerability, and risk perception through tailored, community-based interventions is essential to strengthen PrEP utilization and HIV prevention outcomes in Cameroon.
Conclusion
PrEP uptake remains suboptimal among key populations in the Nylon and New Bell Health Districts. Financial barriers, socio-demographic factors, and sexual behavior have a significant influence on uptake. Tailored public health interventions addressing these barriers are essential for enhancing PrEP utilization and reducing HIV transmission in these vulnerable groups.
1. INTRODUCTION
HIV remains an important public health issue, which has led to more than 40.1 million deaths to date, including 630,000 people in 2022 [1]. According to the World Health Organization (WHO), an estimated 38. 4 million worldwide are living with HIV, with over two-thirds (25. 6 million) in the WHO African Region [1]. Despite significant progress in reducing new HIV infections globally, some countries have recently experienced an increase in new cases [1, 2].
Key populations, who include People Who Inject Drugs (PWID), Female Sex Workers (FSW), Transgender people, men who have Sex with men (MSM), and prisoners, are disproportionately affected due to high-risk behaviors [3, 4]. HIV most impacts these groups, and they present higher rates of infection compared to the general population [3]. In West and Central Africa, which accounts for one-sixth of the world’s new HIV infections, 34% of new infections are among key population (KP) groups [1, 5].
Cameroon, with one of the highest HIV prevalence rates in West and Central Africa, has a mixed (generalized and concentrated) epidemic [1, 6]. Overall, the HIV infection rate among people aged 15-49 has been decreasing: 5.4% in 2004, 4.3% in 2011, and 2.7% in 2018. Moreover, it has concentrated on the Female Sex Workers (24.3%) and men who have Sex with men (20.6%) [6]. In the two large cities of Yaoundé and Douala, the prevalence rate is 2.4% each [7]. The Ministry of Public Health estimates the number of new infections attributed to Douala at 10.4%. The Minister of Public Health estimated the cumulative prevalence of HIV in the Nylon and NEW BELL Health Districts at 22,893 in 2021. The number of FSW infected is estimated at 5,334, and the number of MSM is 4,716, highlighting that these two districts remain hotspots [7]. These districts are densely populated, socioeconomically disadvantaged areas with vibrant markets and substantial concentration of key populations.
Expanding evidence-based interventions among key populations is an important component of the fight against HIV in Cameroon and across the region [7]. There is increasing evidence that PrEP may be an effective biomedical approach to HIV prevention, reducing HIV transmission risk by 90% when taken correctly [8, 9]. In Cameroon and other Sub-Saharan African countries, the President’s Emergency Plan for AIDS Relief (PEPFAR) has supported the implementation of PrEP programs targeting high-risk groups such as FSW, MSM, fathers in serodiscordant relationships, and People Who Inject Drugs (PWID). These services are not provided only through community-based organizations but have also been integrated into health facilities and hospitals, ensuring broader access to PrEP among the targeted populations [9, 10].
Despite this, PrEP uptake remains low in many settings, including Cameroon, because of issues such as stigma, discrimination, and lack of access to prevention [3]. Most importantly, there is a lack of detailed data on PrEP uptake and its determinants in socioeconomically disadvantaged urban settings, such as Nylon and New Bell, which host a large number of key populations.
This study aimed to measure the uptake of PrEP among key groups in the Nylon and New Bell health zones of Cameroon and to identify predictors of increase. Understanding these factors in the local context is essential for designing tailored interventions to prevent HIV among key populations.
2. MATERIALS AND METHODS
2.1. Study Design and Setting
A cross-sectional study was conducted between January and June 2024 to assess PrEP uptake and factors influencing PrEP use among key populations in Nylon and New Bell health districts located in the Douala Littoral region of Cameroon. The HIV prevalence rate in Douala is 2.4%. These regions were important for our study because they are the largest urban centers and major centers of economic and social activities. We selected these areas for our study due to their high concentration of key populations. All these aspects make them a good place to examine PrEP uptake and its predictors among this population at risk of infection. We followed the Sex and Gender Equity in Research (SAGER) guidelines to ensure appropriate consideration of sex and gender in the design, analysis, and reporting of findings [11].
2.2. Study Population
The study targeted key populations, specifically MSM and FSWs, aged 20 years or older who had resided in the Nylon and New Bell health districts for at least six months and had some knowledge of PrEP.
2.3. Sample Size and Sampling Procedures
A purposive non-probability sampling method was employed, as it focused on key populations that are typically difficult to reach [12]. Nylon and New Bell health districts were selected based on the high concentrations of key populations and ongoing Public Health efforts to prevent HIV in these areas. In these districts, the sample size was determined based on practical considerations, including resource availability, time constraints, and the expected willingness of individuals to participate. We aimed to recruit a sample size that would ensure reliable statistical analyses and sufficient representation of Key Populations (KPs), targeting 282 participants. Recruitment took place through health facilities that provided PrEP services (Nylon District Hospital, New Bell District Hospital, and Congo District Medical Center) and was facilitated by peer leaders who employed social network strategies to engage this population.
2.4. Data Collection
Data collection was conducted using structured questionnaires administered face-to-face by trained Research assistants and the principal investigator of this study. The questionnaire was written in English and then translated into French to ensure clarity and understanding by most French-speaking populations. The data collection tool was also pre-tested among the peer leaders we selected from these communities based on their consistent attendance and adherence to PrEP services at local healthcare facilities. The questionnaire included sections on sociodemographic characteristics, knowledge about PrEP, current and past use of PrEP, compliance behaviors, perceived risk of HIV, and access to health services. Confidentiality was maintained throughout.
2.5. Variables and Measurements
The primary outcome variable was PrEP uptake, defined as the proportion of participants who reported ever using PrEP among all the key populations to whom PrEP was proposed based on the risk assessment. Independent variables included sociodemographic characteristics (age, sex, education level, marital status, and monthly income), behavioral factors (substance use, sexual activity, and risk perception), and healthcare access-related factors (proximity to services).
2.6. Data Management and Quality Control
Completed questionnaires were reviewed daily for accuracy and completeness. The data was digitized using Kobo Collect software, facilitating efficient and secure entry into a centralized database. The data validation rules were introduced into the collection tool to minimize errors, and periodic quality checks were set. To maintain the confidentiality of our data, we encrypted and stored it on password-protected systems.
2.7. Statistical Analysis
Data analysis was performed using R version 4.4.1. Using descriptive statistics, we summarized participants' characteristics, including demographic information and PrEP uptake rates. Bivariate analyses and significance tests were performed to examine the association between predictor variables and PrEP uptake using Pearson's chi-square tests.
We included the multivariate logistic regression variables with p values < 0.2 in the bivariate analyses to identify independent predictors of PrEP initiation. We calculated Odds Ratios (ORs), their 95% Confidence Intervals (CIs), and p-values to determine the strength and direction of associations. Findings were presented in tables and figures, highlighting the relationships between predictors and outcomes.
2.8. Ethical Considerations
Ethical clearance was obtained from the Faculty of Health Sciences Institutional Review Board at the University of Buea (reference number: 2024/2374-01/ UB/SG/IRB/FHS). Administrative authorization was obtained from the Littoral Delegate of Public Health and the services of the Nylon and New Bell Health Districts. Written informed consent was obtained from each participant before their involvement in the study.
3. RESULTS
3.1. Socio-demographic Characteristics
Table 1 highlights the main trends in the socio-demographic characteristics of key populations in Nylon and New Bell health districts, where data were collected from 193 Female Sex Workers (FSW) and 91 men who have Sex with men (MSM). The majority of participants were female, comprising 193 (68%). Among the age group, the most significant proportion was those under 25 to 29 years, with 102 individuals in total, including 72 (70.6%) Female Sex Workers (FSW) and 30 (29.4%) men who have sex with men (MSM). Regarding monthly income, most participants (144) earned between 0 and 50,000 FCFA, including 83 (57.6%) FSW and 61 (42.4%) MSM. Regarding marital status, most participants were single, with 266 participants, a predominance of FSW at 68.4%. The largest occupational group was students, with 108 in total. Education levels revealed that 152 participants held a university degree or higher, comprising 99 (65.1%) Female Social Workers (FSW) and 53 (34.9%) males. Among religious affiliations, Catholics were the predominant group, accounting for 142 of the total.
3.2. Uptake of Pre-exposure Prophylaxis
The PrEP uptake cascade shows substantial gaps in uptake among Key Populations (KP). Out of the 284 KPs seen, only 220 (77.5%) were eligible for PrEP service after screening for eligibility according to WHO standards and were offered the service. Among these, only 62 (28.2%) accepted PrEP and were initiated on it Fig. (1).
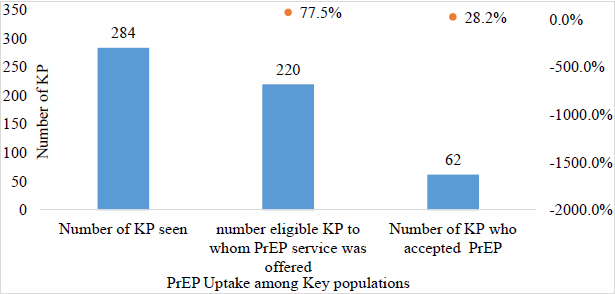
Proportion of PrEP uptake among HIV key populations in the nylon and new bell health districts in 2024.
| Variables | Overall | FSW | MSM |
|---|---|---|---|
| No | No (%) | No (%) | |
| Sex | |||
| Female | 193 | 193 (100.0) | 0 (0.0) |
| Male | 91 | 0 (0.0) | 91 (100.0) |
| Age | |||
| 20-24 | 98 | 59 (60.2) | 39 (39.8) |
| 25-29 | 102 | 72 (70.6) | 30 (29.4) |
| 30-34 | 31 | 29 (93.5) | 2 (6.5) |
| >35 | 53 | 33 (62.3) | 20 (37.7) |
| Monthly Income (FCFA) | |||
| <50,000 | 144 | 83 (57.6) | 61 (42.4) |
| 50,000-100,000 | 52 | 31 (59.6) | 21 (40.4) |
| > 100,000 | 88 | 79 (89.8) | 9 (10.2) |
| Marital Status | |||
| Married | 18 | 11 (61.1) | 7 (38.9) |
| Single | 266 | 182 (68.4) | 84 (31.6) |
| Occupation | |||
| Other (please specify) | 22 | 16 (72.7) | 6 (27.3) |
| Police officer/military personnel | 12 | 2 (16.7) | 10 (83.3) |
| Private sector employee | 60 | 31 (51.7) | 29 (48.3) |
| Sex worker | 82 | 77 (93.9) | 5 (6.1) |
| Student | 108 | 67 (62.0) | 41 (38.0) |
| Highest Level of Education | |||
| Completed primary | 69 | 47 (68.1) | 22 (31.9) |
| Completed secondary | 63 | 47 (74.6) | 16 (25.4) |
| University and higher | 152 | 99 (65.1) | 53 (34.9) |
| Religious Affiliation | |||
| Catholic | 142 | 82 (57.7) | 60 (42.3) |
| Muslim | 46 | 42 (91.3) | 4 (8.7) |
| Pentecostal | 74 | 64 (86.5) | 10 (13.5) |
| Presbyterian | 22 | 5 (22.7) | 17 (77.3) |
| Variables | PrEP uptake | cOR (95% CI) | p-value | aOR (95% CI) | p-value | |
|---|---|---|---|---|---|---|
|
No No (%) |
Yes No (%) |
|||||
| Age | ||||||
| 20-24 | 56 (35.4) | 18 (29.0) | 1 | - | 1 | - |
| 25-29 | 49 (31.0) | 34 (54.8) | 2.16(1.10 - 4.36) | 0.028 | 1.51(0.64, 3.63) | 0.352 |
| 30-34 | 20 (12.7) | 4 (6.5) | 0.62(0.16 - 1.91) | 0.400 | 0.28(0.06, 1.17) | 0.100 |
| > 35 | 33 (20.9) | 6 (9.7) | 0.57(0.19 - 1.50) | 0.325 | 0.42(0.11, 1.37) | 0.175 |
| Highest level of education | ||||||
| Primary | 33 (20.9) | 14 (22.6) | 1 | - | 1 | - |
| Secondary | 27 (17.1) | 26 (41.9) | 2.27(1.01 - 5.28) | 0.052 | 2.65(0.93, 7.87) | 0.072 |
| University | 98 (62.0) | 22 (35.5) | 0.53(0.24 - 1.17) | 0.112 | 0.36(0.13, 0.92) | 0.034 |
| Type of key population | ||||||
| FSW | 120 (75.9) | 34 (54.8) | 1 | - | 1 | - |
| MSM | 38 (24.1) | 28 (45.2) | 2.6(1.40 - 4.85) | 0.002 | 2.97(1.24, 7.30) | 0.015 |
| Sex without a condom in the last 3 days | ||||||
| No | 81 (51.3) | 44 (71.0) | 1 | - | 1 | - |
| Yes | 77 (48.7) | 18 (29.0) | 0.43(0.22 - 0.80) | 0.009 | 0.35(0.15, 0.75) | 0.009 |
| Sex as the primary source of income in the last 6 months | ||||||
| No | 6 (3.8) | 14 (22.6) | 1 | - | 1 | - |
| Yes | 152 (96.2) | 48 (77.4) | 0.14(0.05 - 0.36) | <0.001 | 0.1(0.02, 0.37) | <0.001 |
| Monthly income (FCFA) | ||||||
| <50,000 | 87 (55.1) | 25 (40.3) | 1 | - | 1 | - |
| 50,000-100,000 | 29 (18.4) | 10 (16.1) | 1.26(0.52 -2.91) | 0.701 | 2.28(0.77, 6.70) | 0.138 |
| > 100,000 | 42 (26.6) | 27 (43.5) | 2.35(1.21 - 4.61) | 0.016 | 4.37(1.76, 11.5) | 0.002 |
3.3. Factors Associated with PrEP Uptake Among HIV Key Populations
Table 2 below outlines the factors associated with PrEP uptake among key populations in the Nylon and New Bell health districts. This table shows us that the age range has an impact on the PrEP uptake by our respondents since the majority of individuals who adopted PREP are between 25 and 29 years old, with a rate of 54.8%, which indicates that the latter are more likely to adopt PREP compared to those in the age group between 20 and 24 years old. However, this association is not statistically significant (aOR = 1.51, 95% CI: 0.64 - 3.63, p-value = 0.352). The education level of our participants is also positively associated with the PrEP uptake. We note that the group of participants with a secondary education level had a higher rate of adoption compared to the others (41.9%), though this relationship is not statistically significant (aOR = 2.65, 95% CI: 0.93 - 7.87, p-value = 0.072) However, participants with a university education level have a rate of adoption to the PrEP of (35.5%) and the adjusted odds ratios show that they are significantly less likely to use the PrEP compared to those with only a primary level (aOR = 0.36, CI95%: 0.13 - 0.92, p-value = 0.034).
Key population types also strongly influenced PrEP uptake, particularly MSM, who have a PrEP uptake rate of 45.2% with a significantly higher adjusted odds ratio compared to FSW (aOR = 2.97, 95% CI: 1.24 - 7.30), highlighting that MSM are twice as likely to adopt PrEP as an HIV prevention method compared to FSW. On the other hand, sexual behavior, namely having had condomless Sex in the last three days, is associated with reduced PrEP use. Indeed, individuals who had not had condomless Sex observed a higher proportion (71.0%) of adoption than those who had a low odds ratio (aOR = 0.35, 95% CI: 0.15 - 0.75). Having Sex as a primary source of income in the last 6 months was also found to be a factor reducing PrEP adoption by our participants (aOR = 0.10, 95% CI: 0.02 - 0.37) with a p-value of less than 0.001. Finally, the monthly income of our participants was also found to be a factor associated with PrEP adoption, as individuals with a monthly income greater than 100,000 FCFA had a higher proportion of PrEP initiation (43.5%) (aOR = 0.10, 95% CI: 0.02 - 0.37). Multivariate analysis of the association between monthly income and PrEP uptake confirmed that individuals earning more than 100,000 FCFA per month were significantly more likely to adopt PrEP than the reference group (aOR = 4.37, 95% CI: 1.76 - 11.5). This trend suggests that individuals with higher incomes may have better access to PrEP due to financial constraints.
The multivariate analysis further clarifies the key predictors of PrEP uptake among the populations studied in the Nylon and New Bell health districts. Higher income is a strong positive predictor, with individuals earning more than 100,000 FCFA having substantially higher odds of PrEP uptake. Being MSM also significantly increases the likelihood of PrEP usage, whereas university education and reliance on income from sex work are associated with lower odds of uptake. Additionally, recent engagement in condomless sex is a negative predictor of PrEP usage. These findings underscore the importance of targeted interventions to address income disparities, risk behaviors, and access barriers, thereby improving PrEP uptake among these key populations.
4. DISCUSSION
This study's goal was to explore the various factors influencing PrEP uptake among key populations, aiming to address barriers and improve HIV prevention strategies among these high-risk populations. The research was conducted over 6 months on two key population groups in the health districts of Nylon and New Bell using a non-probability sampling method, which allowed us to collect data from more than 284 people. Among all the participants in our study, we had 65.1% Female Sex Workers (FSW) and 34.9% men who have sex with men (MSM). We selected based on risk assessment, and only 77.4% were eligible for PrEP.
4.1. PrEP Uptake Among KP in Nylon and New Bell Health Districts
Although PrEP as a means of HIV prevention was offered to all these eligible clients, only 28.2% of them accepted PrEP. This rate is significantly lower than the UNAIDS target of 80% by 2025 [13].
The uptake rate in our study aligns with a study conducted in rural areas of Kenya and Uganda by Koss et al. (2020), where they reported a 27% uptake despite awareness and willingness. Highlighting a large number of barriers that still hinder PrEP initiation, including stigma, healthcare accessibility, and structural inequities [14]. However, our proportion is relatively low compared to a study conducted in Cameroon in 2020 on key populations followed by CBOs with a PrEP uptake of 45% [10], which could be justified by certain factors that can influence PrEP initiation, including service delivery models, actors involved in initiating a person on PrEP, as well as structural barriers. The uptake obtained in this study is also comparable to that of a study conducted in the USA under the same conditions among high-risk groups, including MSM, but with clients who have a higher income level [15], which highlights that the significant gaps are not limited only to low-income countries but also to developed countries.
4.2. Factors Associated with PrEP Uptake Among KP in Nylon and New Bell Health Districts
In this study, we also aimed to understand the factors that influence the use of PrEP. To do this, we used bivariate and multivariate analyses. A higher monthly income was significantly associated with using PrEP; people earning more than 100,000 FCFA per month were over four times more likely to accept PrEP (aOR = 4.37, 95% CI: 1.76–11.5, p = 0.002), highlighting monthly income as a critical factor. This finding is consistent with recent studies in the East region of Cameroon in 2024 on ART initiation, which identified financial barriers as key determinants for patients to start treatment. In particular, low-income individuals are less likely to accept medication use as the costs of visits, transportation, and other indirect treatment-related expenses may limit their access to medical and PrEP services [16, 17]. Addressing these economic barriers is, therefore, essential to improving PrEP uptake among vulnerable populations.
Being MSM was another strong predictor of PrEP use in this study (aOR = 2.97, 95% CI: 1.24–7.30, p = 0.015), doubly influencing PrEP use. Our result is consistent with work by Hillis et al. in 2020, who reported that MSM were more likely to be aware of and use PrEP due to targeted public health interventions and increased awareness among this high-risk group [18, 19]. Similarly, a meta-analysis conducted in 2020 demonstrated that MSM had a higher rate of PrEP uptake than other at-risk populations; this work reflects the ongoing efforts of public health interventions to prioritize this group in HIV prevention strategies [20].
It is also interesting to note that our study revealed that the educational level of key populations is also one of the factors strongly influencing their acceptance of PrEP; according to the results, people with a university education level were less likely to accept PrEP than those with a primary education level, with an aOR of 0.36 (p-value = 0.034). This counterintuitive result may be explained by several factors. Educated individuals may have a lower perceived risk of HIV due to their awareness of HIV prevention methods, which could result in less urgency in adopting PrEP. Furthermore, educated individuals might have greater access to other HIV prevention strategies, such as condoms or ART, that they may perceive as more accessible or effective, leading to a decreased reliance on PrEP, as reported by a study conducted in New England [21]. Alternatively, stigma and misinformation also play a role. However, our results contrast with the findings of several studies, such as that of Huang et al., who found that higher education levels were generally associated with greater acceptance of PrEP [22].
Our results suggest that individuals reporting condomless Sex in the past 3 days may underestimate their HIV risk, which appears to be a factor significantly associated with lower odds of PrEP use (aOR = 0.35, 95% CI: 0.15-0.75, p = 0.009). This result is consistent with that of the work carried out by Brooks et al. in 2021 in the USA, where he highlighted that sexual behavior, in particular condom use, is positively associated with condom use; in other words, people who have sex without condoms are often less likely to perceive themselves as at risk for HIV and therefore less likely to use PrEP [23].
Finally, having sex as a primary source of income reduced the odds of using PrEP according to our results, with aOR = 0.10 (p-value < 0.001). This result is in line with the conclusions of a study conducted in Latin America in 2021, where it was noted that sex workers often faced significant barriers such as stigma, discrimination, and limited access to care, which hindered their ability to access PrEP service [24]. In addition, Escudero et al. (2021), in their work on youth therapy, highlighted that economic vulnerability and reliance on sex work would often limit the ability of the latter to prioritize preventive health care, in this case, PrEP, which requires more tailored interventions that respond to these structural challenges [25]. These results sufficiently underscore the importance of addressing specific demographic and socioeconomic barriers to improve PEP uptake among the most at-risk populations. Tailored interventions that focus on improving access, awareness, and financial support, particularly for low monthly income groups and people who have sex as their primary source of income, are essential to ensure broader coverage of PrEP and even reduce HIV incidence in these populations. Future research should consider longitudinal designs and include measures of adherence as well as barriers and facilitators to PrEP use.
5. LIMITATIONS OF THE STUDY
While this study provides important insights into PrEP uptake among key populations in the Nylon and New Bell health districts, it is subject to several limitations. One of the primary limitations is the relatively small sample size of 284 participants, which may not fully represent the broader key populations across Cameroon. The use of purposive and snowball sampling techniques, though useful for reaching hard-to-reach populations such as MSM and FSW, may have introduced selection bias, as participants with certain characteristics might be overrepresented.
CONCLUSION
This study highlights the various factors associated with PrEP uptake among the key population in the Nylon and New Bell health district, including age group, type of key population, socioeconomic status, education level, sexual behavior, and reliance on sex work as a primary income source. The findings emphasize the urgent need for targeted interventions to address barriers such as financial challenges, stigma, and structural inequities, ensuring greater accessibility and adoption of PrEP. Tailoring public health strategies, such as increasing awareness and providing financial support for patients, integrating PrEP services with existing health initiatives to reduce stigma barriers and streamline access, and incorporating advanced community strategies like service home propose home delivery models, can be essential to bridging the gap between current uptake and global HIV prevention targets. Further research should focus on a longitudinal approach to assess adherence to PrEP and explore the barriers and facilitators through a qualitative analysis, inquiring in depth into the factors associated with PrEP adherence.
AUTHORS’ CONTRIBUTIONS
The authors confirm contribution to the paper as follows: L.B.F.: Conceptualized and co-designed this study, conducted data analysis, and drafted the manuscript. E.A.T.: Contributed to the co-design and supervision of this study. F.A.O.A.: Supported the study methodology and provided critical revisions to the manuscript. B.M.Y.: Assisted with data validation and contributed to the writing and editing of the manuscript. P.T.: Supported the study's methodology and data collection and provided additional technical expertise. J.F.: Provided co-supervision, critical guidance, and final review of the manuscript. All authors read and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| PWID | = People Who Inject Drugs |
| FSW | = Female Sex Workers |
| MSM | = Men who have Sex with Men |
| KP | = Key Population |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical clearance was obtained from the Faculty of Health Sciences Institutional Review Board at the University of Buea, Cameroon (reference number: 2024/2374-01/UB/SG/IRB/FHS).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Written informed consent was obtained from each participant before their involvement in the study.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available in the Zenodo repository at https://zenodo.org, reference number 10.5281/zenodo.17419921.
ACKNOWLEDGEMENTS
The authors would like to sincerely thank all the participants from the health districts of Nylon and New Bell for their valuable contributions to this study. We would also like to thank the regional public health delegates for the coast, as well as the district chiefs of Nylon and New Bell, for their diligence, comments, and advice throughout the research process. We cannot end this phase of gratification without thanking the district professionals who participated directly or indirectly in facilitating the collection and dissemination of data for this research.

