All published articles of this journal are available on ScienceDirect.

Characterizing Cis and Trans Women’s HIV Risk and Access to HIV Prophylaxis in Ontario, Canada
Authors Info & Affiliations
Abstract
Introduction
Despite the availability of HIV prevention medications (PrEP, PEP, and PIP), HIV rates among women continue to increase in Canada. This cross-sectional, survey-based study aimed to characterize women’s assessment of their HIV risk, along with their awareness of and access to medication-based HIV prophylaxis.
Methods
A 52-question survey was distributed at 15 community-based organizations in Ontario, Canada, including shelters, addiction treatment and recovery centres, and women’s drop-in programs, from June 2023 to February 2024. Eligible participants were self-identified women who were prophylaxis-naïve and sexually active and/or using drugs.
Results
Of the 318 participants recruited, self-reported knowledge of HIV transmission, risk, prevention, and testing was high, with multiple strategies to decrease risk reported. Of the 302 who responded, 93.7% assessed their HIV risk as low or average; 48.7% were not aware of PrEP or PEP; 73.3% were not aware of PIP; and 89.0% and 87.8% had never been offered PrEP or PEP, respectively, although interest in both oral and injectable medications was high. Nearly half (48.4%) believed they would not qualify for PrEP, with barriers cited including perceived lack of risk (40.9%), concerns about side effects (33.6%), affordability (26.1%), and potential adherence challenges (17.0%).
Discussion
Women’s self-perceived HIV risk was not congruent with objective HIV risk. Most women were unaware of HIV prevention medications and believed they would not be eligible; among those who perceived themselves as eligible, fewer than one-third had been offered HIV prevention options.
Conclusion
Additional clinical, public health, and policy efforts are needed to effectively engage women in HIV prevention care.
1. INTRODUCTION
Pre-exposure prophylaxis (PrEP) for HIV has been shown to be highly effective across populations [1-6]. Similarly, post-exposure prophylaxis (PEP) is effective in preventing HIV infection, if a 28-day course is started within 72 hours of moderate- or high-risk exposure [7]. Since approval, PrEP has become a cornerstone in reducing new HIV infections in at-risk populations in Canada and globally, with current guidelines recommending its use in at-risk men who have sex with men (MSM), heterosexual individuals, and people who inject drugs (PWID) [7]. Compared to PrEP, options for PEP, including “PEP-In-Pocket” (PIP), are less well studied. While there is evidence to support the use of PrEP, there is less evidence related to awareness, acceptability, and interest in PEP/PIP as a prevention option.
Despite the availability of these medication-based prevention strategies, HIV infection rates are increasing among Canadian women, while rates are decreasing among men [8], yet offerings and access among women in Canada are not well described. Importantly, while there is limited Canadian data, international studies indicate that women may not be fully aware of their own HIV risk [9-14]. Additionally, research from the United States has shown that women have lower rates of PrEP use compared to men, and the PrEP-to-need ratio among women was five times lower than that among men [15]. Several studies have investigated awareness as a likely cause of this discrepancy, with women’s awareness of PrEP ranging from virtually zero awareness in studies conducted in San Francisco and Washington [9, 16] to 31.6% of women in a survey conducted in Connecticut [17]; and overall, PrEP awareness among women has been found to be lower than among men [10]. Beyond lower levels of awareness, numerous studies have also shown that women’s interest in learning about PrEP is high, with particularly strong interest among young women, women in serodiscordant couples, those engaged in sex work, and transgender women [9-14, 18-21]. PrEP interest and intentions are also associated with women’s personal perception of HIV risk due to sexual risk behaviours, sharing injection drug equipment, or environmental exposures [9, 11-13, 17, 22]. With respect to PEP, a single study among those engaged in sex work and their clients indicated that awareness was low, but willingness to use PEP was high, with nearly all participants supporting increased efforts to promote PEP [23].
At present, there is a comparative lack of evidence regarding women and HIV prevention medications in Canada. This cross-sectional survey-based study aimed to assess women’s self-assessed HIV risk in comparison to their endorsed risk factors in Ontario, Canada. In addition, we aimed to understand women’s awareness, interest, values, and preferences regarding PrEP, PEP, and PIP.
2. METHODS
2.1. Design and Population
This study used a cross-sectional survey that was administered at community sites across Ontario, Canada, between June 2023 and February 2024. Participants self-identified as women at least 18 years old, who were sexually active or/and using substances. Additional inclusion criteria were willingness and capacity to provide informed consent (as determined by the study staff conducting recruitment and consent), and English proficiency sufficient to understand and complete the survey. Exclusion criteria included known HIV positivity or current/previous use of HIV prophylaxis medications. Study team members were trained to assist with reading and interpreting a question but were not involved in obtaining responses.
2.2. Survey Instrument and Recruitment
The primary instrument was an exploratory paper-based, 52-question questionnaire. The survey was co-developed and refined based on feedback from community stakeholders, but was not pilot tested. The survey assessed demographic factors; HIV risk, including sexual health history and drug use history; subjective HIV risk and knowledge, including prior knowledge of PrEP, PEP, and PIP; interest and attitudes towards PrEP and PEP/PIP; and preferences regarding health information and services (Table S1). The survey included whether participants were born in Canada, their racial/ethnic group, and family income using modified instruments developed by the Mount Sinai Health System [24]. The sexual health and drug use history sections included several sexual and drug-related HIV risk factors, respectively. Subjective HIV risk was assessed by asking participants to assess their own risk on a 5-point Likert scale. Recruitment for this study took place in partnership with 15 community-based organizations in Southern Ontario, including shelters, addiction treatment and recovery centres, women’s drop-ins, and women’s programming. Data was entered by team members not involved in the recruitment of collection.
2.3. Study Definitions
Self-assessed HIV risk was categorized as “low-average self-assessed risk” if the participant’s response was “very low”, “low”, or “average”, and as “high self-assessed risk” if the participant’s response was “high” or “very high”. Sexual risk factors included sex work/transactional sex, concurrent/multiple partners, sexual violence, sexually transmitted infections, and if the participant reported having had sex while intoxicated. Drug use risk factors included sharing injection equipment, being injected by someone else, and taking drugs from someone else. Responses were grouped based on whether they reported none versus at least one risk factor.
2.4. Statistical Analysis
Characteristics were reported as mean and standard deviation, median and interquartile range (IQR), and numbers and percentages, as appropriate. Chi-squared testing was used to examine factors associated with self-assessed HIV risk. Complete case analysis was used for all analyses. A two-tailed p-value <0.05 was considered statistically significant. Statistical analyses utilized STATA Version 15.1 (StataCorp, College Station, TX). This study was designed as a descriptive study, and therefore was not powered for sample size based on a primary outcome. However, by recruiting 318, with 302 participants completing the survey, we were able to determine whether women with higher self-assessed risk were more likely to have reported at least one sexual or drug use risk factor.
3. RESULTS
3.1. Study Population
In total, 318 participants completed the survey. Overall, 7% (n=22) were aged 18-22, 12% (n=39) were 23-26, 27% (n=87) were 27-35, 23% (n=73) were 36-45, 15% (n=47) were 46-55, 12% (n=37) were 56-65, and 4% (n=13) were 66 or older. These categorical age groups were chosen based on life stage. Most of the participants were born in Canada (n=228, 71.7%) and had completed secondary school or more (n=261, 82.1%). Nearly all participants reported that they were assigned female at birth (n=314, 98.7%). With respect to publicly funded medication coverage, 80.8% (n=257) reported some form of publicly funded medication coverage, in the form of Ontario Drug Benefit, Interim Federal Health (federal coverage for refugees who do not yet have provincial coverage), and Non-insured Health Benefit (federal coverage for Indigenous Peoples). Income level was also considered, with 46.5% (n=148) reporting an income of less than $30,000 (n=148, 46.5%), with another 30.5% (n=97) reporting an income of at least $30,000 (n=97, 30.5%); the remainder did not answer or indicated that they did not know their income. Participant demographics are summarized in Table 1. In terms of existing social and health care supports, 75.8% (n=241) reported having a primary care provider, 31.8% (n=101) had a routine pharmacist, 31.4% (n=100) had a case worker, and 28.0% (n=89) had a mental health worker. While 25.8% (n=82) and 25.2% (n=80) had supportive family and friends, respectively, 6.3% (n=20) reported having none of these supports.
| Variable | Number (%) |
|---|---|
| Age | - |
| 18-22 | 22 (6.9) |
| 23-26 | 39 (12.3) |
| 27-35 | 87 (27.4) |
| 36-45 | 73 (23.0) |
| 46-55 | 47 (14.8) |
| 56-65 | 37 (11.6) |
| >66 | 13 (4.1) |
| Sex Assigned at Birth | - |
| Female | 314 (98.7) |
| Male | 3 (0.9) |
| Other/did not answer/unknown | 1 (0.4) |
| Born in Canada | - |
| No | 83 (26.1) |
| Yes | 228 (71.7) |
| Other/did not answer/unknown | 7 (2.2) |
| Income, CAD | - |
| <30,000 | 148 (46.5) |
| >30,000 | 97 (30.5) |
| Other/did not answer/unknown | 73 (23.0) |
| Experiencing homelessness | - |
| No | 214 (67.3) |
| Yes | 104 (32.7) |
| Other/did not answer/unknown | 0 (0) |
| Medication Coverage | - |
| No | 52 (16.4) |
| Yes | 257 (80.8) |
| Other/did not answer/unknown | 9 (2.8) |
3.2. Baseline HIV Knowledge and Risk Management
Participants were asked to rate their knowledge of HIV transmission, testing, and treatment on a five-point Likert scale ranging from “Not at all knowledgeable” to “Very knowledgeable”. 65.0% (201/309) stated they were “fairly knowledgeable” or “very knowledgeable” about how HIV is transmitted, and 59.1% (182/308) said they were fairly or very knowledgeable about HIV risk factors. When asked about prevention, 61.3% (190/310) said they were somewhat or very knowledgeable about HIV prevention strategies, and a similar number (65.2%, 199/305) were somewhat or very knowledgeable about HIV testing. By comparison, a much lower proportion (34.9%, 107/307) were somewhat or very knowledgeable about HIV treatment options (Fig. 1).
When asked about their last time being tested for HIV, 17.6% (56/318) said they had never been tested; 9.1% (29/318) said they did not remember; and 50.6% (161/318) had been tested within the last 2 years (Fig. 2). Testing occurred in a variety of settings, and 151/318 identified these locations which included 35.8% (54/151) in primary care; 28.5% (43/151) in hospital settings; 13.9% (21/151) in a walk-in clinic; 7.3% (11/151) in sexual health; and 2.0% (3/151) self-tested.
In terms of existing HIV risk reduction strategies, the most reported strategy was sexual monogamy (41.1%, n=131), followed by barrier methods (36.2%, n=115). Other reported risk reduction strategies included regular self-testing (27.4%, n=87), partner testing (21.1%, n=67), refraining from sharing drug injection equipment (11.9%, n=38), or other methods to reduce their risk (13.2%, n=42). 14.2% (n=45) did not use any strategies to reduce their risk.
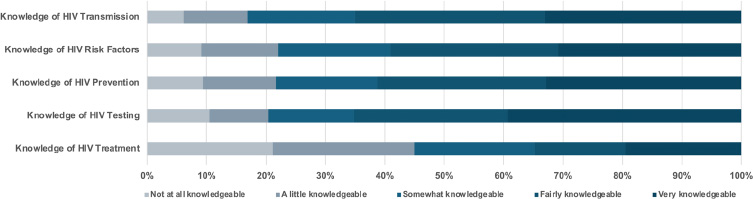
Self-Reported Knowledge of HIV Risk and Care. Participants’ self-reported knowledge as rated on a 5-point descriptive scale for knowledge of transmission, risk factors, prevention, testing, and treatment (% of those who completed the question).
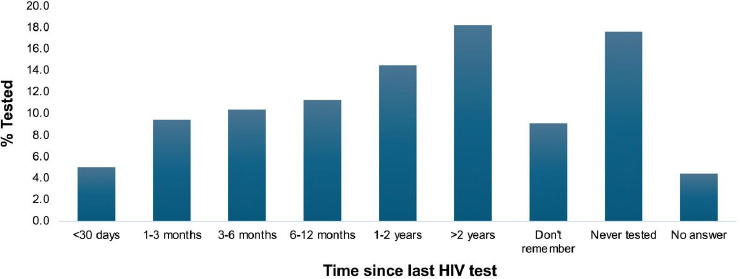
Most Recent HIV Test. Timing of participants’ most recent HIV test based on self-report.
| Characteristic |
Total N = 318 (100%) |
Self-assessed HIV risk n = 302 |
||
|---|---|---|---|---|
|
Low-Average n = 283(93.7%) |
High N = 19 (6.3%) |
p-value | ||
| Sexual risk factors, n (%) | - | - | - | - |
| Self-reported no risk factors | 155 (48.7) | 142 (50.2) | 2 (10.5) | 0.001 |
| Self-reported ≥1 risk factors | 163 (51.3) | 141 (49.8) | 17 (89.5) | |
| HIV positive partner, n (%) | - | - | - | - |
| No | 110 (34.6) | 104 (36.8) | 5 (26.3) | 0.83 |
| Yes | 1 (0.3) | 1 (0.4) | 0 (0) | |
| Other/did not answer/unknown | 207 (65.1) | 178 (62.9) | 14 (73.7) | - |
| Exchanged sex, n (%) | - | - | - | - |
| No | 210 (66.0) | 197 (69.6) | 7 (36.8) | <0.001 |
| Yes | 37 (11.6) | 25 (8.8) | 10 (52.6) | |
| Other/did not answer/unknown | 71 (22.3) | 61 (21.6) | 2 (10.5) | - |
| Condomless anal sex, n (%) | - | - | - | - |
| No | 197 (62.0) | 181 (64.0) | 11 (57.9) | 0.10 |
| Yes | 51 (16.0) | 42 (14.8) | 6 (31.6) | |
| Other/did not answer/unknown | 70 (22.0) | 60 (21.2) | 2 (10.5) | - |
| Concurrency, n (%) | - | - | - | - |
| No | 188 (59.1) | 173 (61.1) | 9 (47.4) | 0.02 |
| Yes | 60 (18.9) | 50 (17.7) | 8 (42.1) | |
| Other/did not answer/unknown | 70 (22.0) | 60 (21.2) | 2 (10.5) | - |
| Experienced sexual violence, n (%) | - | - | - | - |
| No | 203 (63.8) | 191 (67.5) | 5 (26.3) | <0.001 |
| Yes | 45 (14.2) | 32 (11.3) | 12 (63.2) | |
| Other/did not answer/unknown | 70 (22.0) | 60 (21.2) | 2 (10.5) | - |
| STI positive, n (%) | - | - | - | - |
| Not in the last 12 months | 293 (92.1) | 261 (92.2) | 16 (84.2) | 0.22 |
| At least once | 25 (7.9) | 22 (7.7) | 3 (15.8) | |
| Sex while intoxicated, n (%) | - | - | - | - |
| No | 203 (63.8) | 185 (63.4) | 6 (31.6) | 0.02 |
| Yes | 107 (33.7) | 92 (32.5) | 13 (68.4) | |
| Other/did not answer/unknown | 8 (2.5) | 6 (2.1) | 0 (0) | - |
| Drug use risk factors, n (%) | - | - | - | - |
| Self-reported no risk factors | 219 (68.9) | 200 (70.7) | 6 (31.6) | <0.001 |
| Self-reported ≥1 risk factors | 99 (31.1) | 83 (29.3) | 13 (68.4) | |
| Shared injection equipment, n (%) | - | - | - | - |
| No | 241 (75.8) | 220 (77.7) | 14 (73.7) | 0.007 |
| Yes | 12 (3.8) | 8 (2.8) | 3 (15.8) | |
| Other/did not answer/unknown | 65 (20.4) | 55 (19.4) | 2 (10.5) | - |
| Injected by someone else, n (%) | - | - | - | - |
| No | 224 (70.4) | 204 (72.1) | 12 (63.2) | 0.02 |
| Yes | 29 (9.1) | 24 (8.5) | 5 (26.3) | |
| Other/did not answer/unknown | 65 (20.4) | 55 (19.4) | 2 (10.5) | - |
| Taken drugs from others, n (%) | - | - | - | - |
| No | 169 (53.1) | 156 (55.1) | 7 (36.8) | 0.02 |
| Yes | 84 (26.4) | 72 (25.4) | 10 (52.6) | |
| Other/did not answer/unknown | 65 (20.4) | 55 (19.4) | 2 (10.5) | - |
3.3. Reported Risk Factors Compared to Self-Assessed Risk
56.6% of the sample reported HIV risk factors (n=180), including 51.3% (n=163) who reported one or more sexual risk factors and 31.1% (n=99) who reported at least one drug use risk factor. The most reported sexual risk factor was having sex while significantly intoxicated (33.7%, n=107), and the most common drug risk factor was taking drugs from another person (26.4%, n=84). 302 participants provided a response regarding self-assessed HIV risk and were included in the analysis of correlates. Of these, 93.7% (n=283) assessed their HIV risk as low or average. The self-assessed high-risk group had a greater proportion of women <26 years old compared to the self-assessed low/average risk group. Women with higher self-assessed risk were more likely to have reported at least one sexual risk factor (49.8% vs. 89.5%) and at least one drug use risk factor (29.3% vs. 68.4%). Reported risk factors associated with self-assessed risk are listed in Table 2.
3.4. HIV Prophylaxis Knowledge, Experiences, Preferences, and Perceived Access
When asked to rate their awareness of various prophylaxis formulations, of the 318 total participants, 48.7% (n=155) were not aware of PrEP or PEP; and a greater majority were not aware of PIP (73.3%, n=233). Most had never been offered either PrEP (89.0%, n=291) or PEP (87.8%, n=287). Of those who had been offered prophylaxis medications, primary care providers were the most frequently reported type of provider to have offered PrEP (39.1%, 9/23) or PEP (42.9%, 9/21). Respondents indicated whether the gender of their health care provider impacted their comfort discussing sexual health, and 53.5% (n=170) reported it did not impact on their comfort, and 33.0% (n=105) indicated they were most comfortable with a cisgender woman, 3.8% (n=12) were most comfortable with a cisgender man, and 1.3% (n=4) were most comfortable with a transgender or nonbinary provider. Participants were asked to comment on their preferences for injectable as compared to oral PrEP. Overall, 17.9% (n=57) were interested in oral but not injectable PrEP, whereas 7.9% (n=25) were interested in injectable but not oral PrEP. A large number would consider injectable PrEP (39.9%, n=127), and of these, 43.3% (n=55) indicated they preferred injectable PrEP compared to oral PrEP.
Perceived access to HIV prevention medication could impact health-seeking behaviour. In our sample, 48.4% believed they would not qualify for PrEP (n=154), however, 10.4% (n=33) and 3.5% (n=11) believed they would qualify based on sexual or drug risk, respectively. Of the remaining participants, 32.4% (n=103) were unsure if they would qualify, and 0.3% (n=1) did not answer the question. Of the 33 participants who believed they would meet indications based on sexual risk, 84.8% (n=28) had reported at least one sexual risk factor. Similarly, of the 11 who believed they were eligible based on drug risk, 81.8% (n=9) reported at least one drug risk factor. Of those who thought they met indications based on sexual risk factors, 6/33 had been offered PrEP, and 4/33 had been offered PEP/PIP. Of those who thought they met indications based on drugs, 2/11 had been offered PrEP, and 1/11 had been offered PEP/PIP. Of the 48.4% who believed they are not eligible (n=154), 48.7% (n=75) reported sexual risk factors, and 20.1% (n=31) reported drug risk factors.
3.5. Prophylaxis Facilitators and Barriers
Excluding those who indicated they are not interested in PrEP, the most frequently cited reason for being interested in PrEP was feeling safer (32.7%, n=104). Other motivating factors for PrEP are summarized in (Fig. 3A). By comparison, the most reported reason not to use PrEP was that participants did not feel they were at risk (40.9%, n=130). Other barriers included side effects (33.6%, n=107), affordability (26.1%, n=83), and difficulty with adherence (17.0%, n=54). PrEP barriers are summarized in (Fig. 3B).
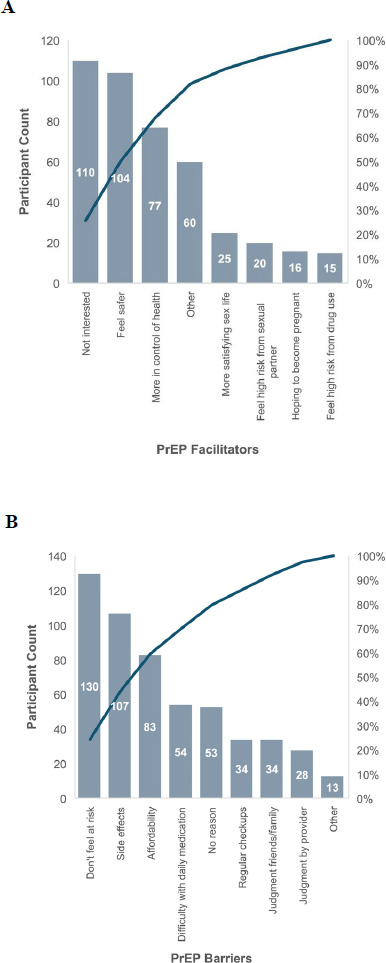
PrEP A) Facilitators and B) Barriers.
Regarding PEP, 33.6% (n=107) reported they would not use PEP for HIV prevention. However, 50.9% (n=162) reported they would use PEP in the event of a hypothetical future exposure to HIV, and 9.1% (n=29) reported they would be interested in a prescription in advance of an exposure (PEP-In-Pocket modality). Barriers to PEP included concerns about side effects (37.1%, n=118), cost (33.0%, n=105), and adherence for a full 28-day course (18.9%, n=60). PEP barriers are summarized in Table 3.
| Factors | Number (%) |
|---|---|
| Concerns about side effects | 118 (37.1) |
| Affordability concerns | 105 (33.0) |
| Worried I would forget to take the pills on time for the full 28 days | 60 (18.9) |
| Having to wait in an emergency room | 49 (15.4) |
| Difficulty getting a prescription within 72 hours of an exposure | 47 (14.8) |
| Fear of judgment by friends/family | 45 (14.2) |
| Fear of judgment by providers | 43 (13.5) |
3.6. Health Information and Accessibility Preferences
The participants’ preferred source of health information was from a health care provider, 50.3% (n=160); while 36.5% (n=116) indicated they preferred to learn about options online or from social media; 1.9% (n=6) through word of mouth; and 1.6% (n=5) from physical advertisements such as billboards and signs.
4. DISCUSSION
This study describes women’s HIV testing history, assessment of their risk factors, and variables related to decision-making for HIV prophylaxis. Our findings add to a growing body of research evaluating women’s HIV risk, demonstrating that women are increasingly at risk of HIV infection, both in Canada and in comparator countries [25], but have low awareness of their risk and prevention options. Specifically, self-perceived HIV risk is not congruent with objective HIV risk based on sexual activity or drug use. Additionally, women did not believe they were eligible for medication, and even among those who thought they might be, they had not been offered medication. Despite this, there was significant interest in HIV prevention medication-based interventions. Our findings, which we highlight along various steps of the prophylaxis care continuum, signify the urgency of addressing persistent gender gaps and opportunities to improve uptake in this population.
In our study sample, the rate of HIV testing was fair, with half of the participants indicating they had been tested in the last two years, and around one in five participants indicating they had never been tested. With respect to risk assessment, only 6% assessed their risk as elevated. This overall perception of low risk runs contrary to the set of risk factors reported by the sample, with 51% and 31% having reported one or more sexual and drug risk factors, respectively. While some reported risk factors were associated with an increased likelihood of high self-assessed risk, there were still many “low subjective risk” women reporting each risk factor. Neither condomless anal sex nor previously testing positive for an STI was associated with higher self-assessed risk. These findings are like existing literature, which is largely from sub-Saharan Africa. For example, a 2017 study found that HIV risk perception was associated with condom use, having multiple lifetime partners, knowledge of partner HIV status, and age-disparate relationships but not with STI history [26].
Historically, testing rates among Ontario women have been characterized as high, peaking at 325,318 tests in 2019 before dropping in 2020; a change attributed to the COVID-19 pandemic [27, 28]. While our study is not representative of women in Ontario, many reported risk factors but had not been tested recently. This is concerning in the context of recent increases in HIV infection among Canadian women [29]. Previous studies have also indicated that public perceptions of HIV as affecting primarily gbMSM has impaired accurate risk assessment among heterosexual women [20, 30, 31]. Testing is often the first step in the HIV cascade of care as well as in HIV prevention; therefore, shifting these perceptions is critical. Universal testing approaches, as adopted in British Columbia, Canada [32, 33], are promising and may facilitate routine testing as the first step in linkage to HIV prevention care.
Our results indicate that awareness of prophylaxis is low, and despite reporting risk factors, many participants believed they would not be eligible for PrEP. Previous studies have shown a clear gender gap in PrEP awareness [10, 30]. In Ontario, this gap is clear at the level of PrEP uptake; in 2022, 97% of all PrEP users in the province were men [34]. The literature suggests that women’s uptake of prophylaxis is limited by poor knowledge and poor HIV risk self-assessment, which is in turn driven by perceptions that HIV and prophylaxis pertain mostly or exclusively to men [19, 31]. Nevertheless, our study and findings within the literature show that women’s motivations for and against prophylaxis use relate to perceived risk; therefore, improving health information about HIV risk and prophylaxis availability may improve uptake of prophylaxis in this population [12].
In general, much of the literature around PrEP suggests that women face individual and systemic barriers to PrEP use [10, 18, 19, 30]. Other barriers include financial issues, provider-related concerns, inability or unwillingness to commit to the PrEP protocol within the context of a trial, and women’s low self-perceived HIV risk. Many of these were borne out in our study; in particular, low self-perceived HIV risk was a key factor in our sample’s decision-making for prophylaxis. Additionally, one-third of women identified cost as a barrier to accessing HIV prevention. While financial barriers remain a concern, many individuals who perceive cost as a hurdle already have access to programs that reduce or eliminate medication expenses, but may be unaware of their eligibility. Enhancing education targeted towards women regarding available HIV prevention options and support programs could help address these misconceptions and improve access.
Conversely, our sample indicated a high level of trust in health care providers to receive health information, with no predominant gender preference for the provider. This study did not assess provider-related issues with prophylaxis in this population, but previous studies have found additional barriers, including perceived stigma from providers, knowledge gap among providers themselves, lack of screening women for PrEP indications, and reluctance to prescribe PrEP [9, 10, 22, 35]. Guideline updates in the United States reflect this changing landscape, with the United States Centers for Disease Control and Prevention (CDC) releasing updated HIV Prevention Guidance in 2021 to further emphasize the importance of offering HIV prevention medication to women [36], noting that only 10% of women who may benefit in 2019 were accessing PrEP [37]. Similarly, the American College of Obstetricians and Gynaecologists released a practice advisory in June 2022 recommending that Obstetrician-Gynaecologists discuss PrEP with all sexually active adolescent and adult patients, rather than providing this information to only those considered at substantial risk of HIV infection [38]. These and other initiatives are aimed at bridging the gap between providers and women, and to encourage appropriate screening and prevention. In Canada, clinical criteria for prophylaxis use in women have been described as less well developed compared to those for men, pointing to a deficit in providing HIV prevention offerings for women [34, 39].
Compared to PrEP, women’s awareness and use of PEP is less studied. While there is evidence to support the use of PEP [7], there is less evidence related to awareness, acceptability, and interest in PEP as a prevention option [40]. Our study showed that roughly half of participants would use PEP if they had an exposure to HIV, and 9% would be interested in a prescription in advance of exposure (PIP). Barriers to PEP were like those for PrEP, with financial factors, side effects, and access issues predominating. In a previous study in China barriers to PEP use were similar those described in the literature for PrEP: side effects, price, efficacy, privacy, and adherence [23]. Our study adds Canadian data to support these well-described barriers.
5. LIMITATIONS
While recruitment of participants was from a diverse group of community-based organisations and services, a random sample was not feasible, and therefore our results are not generalizable to the entire population of self-identified women in Ontario, especially because by way of being at these settings, participants were able to navigate some aspect of social services. Our sample also had low representation of transgender women (those assigned male at birth) and women born outside of Canada. These issues of representation may also limit generalizability, and future research should prioritize these two groups. Similarly, smaller numbers in certain groups may lead to spurious associations, and given that this is largely a descriptive study, less emphasis should be placed on the statistical significance of between-group comparisons involving such groups. Second, our conclusions are drawn entirely from self-reported data, which may introduce bias. Participants were informed that the results would be de-identified; however, response bias due to recall issues, stigma, or survey comprehension may limit the validity of results. Finally, the cross-sectional design limits our ability to determine a causal relationship between variables. For example, while our analysis assumed self-assessed HIV risk to be at least partially informed by risk behaviours, this causal relationship cannot be concluded due to the nature of our design.
CONCLUSION
This study highlights women’s self-assessed risk and HIV prophylaxis decision-making, and further characterise the previously known gender gap in both awareness and uptake of HIV prevention measures, highlighting the need to address these disparities. The relatively lower rates of HIV testing and the disconnect between perceived risk and actual risk (as approximated by reported risk factors) suggest a concerning trend to be addressed through increased patient education. Our findings suggest that women’s awareness of their own HIV risk and prevention options available to them limits uptake of HIV prophylaxis; consequently, improvements in awareness may reduce the incidence of HIV in this population. Finally, the study demonstrates women are often poorly informed but trust their providers for health advice, providing an opportunity for clinicians to have discussions about HIV risk and prevention with women, including while providing other types of care, and offer both testing and prophylaxis as indicated.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: R.V.U., K.M., M.J.B.: Study Concept or Design; R.V.U., M.J.B, G.H: Data analysis or interpretation; R.V.U., M.J.B, P.E.M, C.M, G.H, I.B: Writing - reviewing and editing; P.E.M, F.C.,C.M.: Retrieved the data; M.J.B: Resources were provided; P.E.M., F.C., C.M., Y.J., S.R.: Data curation and supervised.
LIST OF ABBREVIATIONS
| PrEP | = Pre-exposure prophylaxis |
| PEP | = Post-exposure prophylaxis |
| PIP | = PEP-in-Pocket |
| MSM | = Men who have sex with men |
| PWID | = People who inject drugs |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the York University, Canada office of Research Ethics, through the Human Participants Review Committee (certificate e2023-054).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The data of current study are available from corresponding author, [M.J.B], on a reasonable request.
FUNDING
This study was funding by the York University, Canada Faculty of Health Junior Faculty Funds and Minor Research Grant (NPA MJB, no grant number) and by a CIHR Project Grant (NPA IIB 202010).
ACKNOWLEDGEMENTS
We would like to thank the organizations that collaborated in order to ensure diverse representation of participants across Southern Ontario, as well as the participants for their time.

