All published articles of this journal are available on ScienceDirect.

Virological Effectiveness of Dolutegravir-based Second-line ART in the Context of NRTI Resistance Among HIV-Positive Patients in India
Authors Info & Affiliations
Abstract
Introduction
In India, approximately 4.7% of the 1.5 million people living with HIV (PLH) are on second-line (2L)-ART, highlighting the need for effective treatment strategies addressing ART-switches in the background of HIV drug resistance (HIVDR) following first-line (1L)-ART failure.
Methods
This single-arm, prospective pragmatic study was conducted at a tertiary care hospital in northern India from January 2020 to December 2022. Participants aged ≥13 years with documented 1L-ART failure (HIV RNA ≥ 1000 cp/mL) were enrolled. Eligible patients were grouped into four cohorts based on their prior ART and HIVDR profiles. The study regimen included a 2L-ART regimen comprising tenofovir (TDF/TAF), lamivudine (3TC)/emtricitabine (FTC), and dolutegravir (DTG). The primary endpoint was virological suppression (VS), defined as HIV RNA < 1000 cp/mL at 24 and 48 weeks.
Results
A total of 64 patients were included. At 24 weeks, the overall VS rate in the on-treatment analysis (OTT) was 94.6% (53/56), with 92.8% (52/56) achieving HIV RNA < 200 cp/mL. Among those with full TFV susceptibility, 97.1% (34/35) attained VS, while 90.5% (19/21) without predicted susceptibility achieved the same. For reccycled TFV, the OTT showed that 96.9% (31/32) attained VS, with 93.8% achieving HIV RNA level of < 200 cp/mL, compared to 91.7% (22/24) of first-time TFV users attaining HIV RNA level of < 200 cp/mL.
At 48 weeks, the OTT indicated 100% VS among 52 patients, with 96.2% (50/52) attaining HIV RNA level of < 200 cp/mL. This included 93.8% (30/32) of patients with full TFV susceptibility and 93.8% (30/32) of those who received recycled TFV.
Discussion
Our findings demonstrate that DTG-based 2L-ART remains virologically effective even in patients with prior tenofovir (TFV) or zidovudine (AZT) exposure and in those lacking predicted TFV susceptibility based on drug resistance testing at 1L-ART failure. These results are consistent with findings from the ARTIST and NADIA trials and add novel Indian data to the growing body of evidence supporting TFV recycling in 2L-ART regimens. In resource-limited settings where resistance testing is often unavailable and AZT poses challenges related to toxicity, pill burden, and monitoring, this simplified once-daily regimen offers a practical alternative.
Conclusion
This study reinforces the viability of DTG-based second-line regimens with a TFV backbone as an effective and practical option, even in the presence of prior nucleoside reverse transcriptase inhibitor exposure or resistance. These findings support the use of simplified, once-daily fixed-dose combinations of TFV + 3TC/FTC + DTG as a durable and scalable 2L-ART strategy in resource-limited settings.
1. INTRODUCTION
Combination Antiretroviral Therapy (ART) has significantly improved the management of HIV/AIDS, reducing associated morbidity and mortality. However, up to 80% of people living with HIV (PLH) require second-line (2L) ART due to first-line (1L) treatment failure [1-3]. In India, 4.7% of the 1.5 million PLH on ART, totalling 0.65 million, are on 2L-ART, emphasising the need for effective, safe, and well-tolerated 2L-ART regimens [4]. While the World Health Organization (WHO) provides comprehensive guidelines for 1L-ART [5], uncertainties persist regarding viable 2L-ART alternatives [6, 7].
Historically, 2L-ART involved a backbone of two nucleoside reverse transcriptase inhibitors (NRTI) with a ritonavir-boosted protease inhibitor (b/PI), but the advent of dolutegravir (DTG) has reshaped this landscape [5, 8-10]. With DTG becoming the standard for 2L-ART, the approach to optimizing the NRTI-backbone depends on prior NRTI use, often requiring a switch to a previously unused NRTI [11].
While this approach, shaped by the impracticality and limitations of resistance testing and sparse viral load (VL) monitoring, particularly in resource-limited settings, seems to provide a practical solution, it comes with inherent challenges. Patients exposed to tenofovir (TFV) in 1L-ART must switch to zidovudine (AZT), which has drawbacks including increased pill burden with its twice-daily dosing, and side-effects that require intricate monitoring [5, 12]. For PLH exposed to AZT in 1L-ART, using a TFV-backbone in 2L-ART may seem favourable, but it does not address the potential impact of thymidine-analogue mutations (TAMs), which accumulate as a result of long term exposure to AZT and older thymidine-analogues, and potentially impact TFV-susceptibility. This complexity is further heightened for patients with unclear ART histories or multiple NRTI switches in 1L-ART, where it is often difficult to determine the exact point of 1L-ART failure or the specific first-line NRTI backbone that failed.
Moreover, the virological effectiveness of DTG-based 2L-ART in the Indian population, especially concerning specific ART switch strategies and HIV drug resistance (HIVDR) at 1L-ART failure, remains understudied. With this background, the present study-with its primary objective of assessing the virological effectiveness of a three-drug DTG-based 2L-ART regimen with a TFV backbone-reports 48 week follow-up results for 64 PLH. The cohort includes individuals with recycled TFV, first-time TFV exposure in 2L-ART, and TFV use in the context of significant resistance predicted at 1L-ART failure.
2. METHODS
2.1. Design and Participants
A single-arm prospective pragmatic study at a tertiary hospital and immunodeficiency centre in northern India, aiming to assess virological outcomes of 2L-ART comprising TFV (either tenofovir disoproxil fumarate (TDF) or tenofovir alafenamide (TAF) + lamivudine (3TC)/emtricitabine (FTC) + DTG, particularly in relation to baseline HIVDR.
Enrolment spanned from January 2020 to December 2022, with consecutive cases meeting the inclusion criteria being enrolled. Eligible participants, aged ≥ 13 years and who had a minimum 12 month history of 1L-ART (dual-NRTI + NNRTI). Inclusion criteria involved confirmation of 1L-ART failure with two consecutive plasma HIV RNA measurements ≥ 1000 cp/mL, either at enrolment or a historical record of 1L-ART failure (meeting the virological criteria for 1L-ART failure), who, prior to enrolment, were receiving stable 2L-ART, comprising dual-NRTI + b/PI or integrase strand transfer inhibitor (INSTI) based regimens other than the study regimen of TFV + 3TC/FTC + DTG. Additionally, access to HIV-1 genotyping and drug resistance testing (DRT) or prior DRT at 1L-ART failure was required.
Exclusions encompassed (i) estimated glomerular filtration rate (GFR) < 50 mL/min/1.73 m2, (ii) abnormal liver function at baseline (aspartate or alanine transaminases > 2-times the upper limit of normal), (iii) known hypersensitivity or intolerance to the study-regimen, (iv) conditions likely to impact drug adherence and follow-up, (v) baseline INSTI DRMs, and (vi) those who declined consent.
Participants virologically suppressed on other standard or non-standard 2L-ART regimens before enrolment and undergoing substitution to the study regimen were not excluded, provided that historical DRT results at 1L-ART failure were available. Participants with INSTI-resistance or those meeting criteria for treatment failure on a prior 2L-ART regimen were excluded.
A sample size of 60 achieved 80.490% power to detect a difference (P1-P0) of 0.10 using a one-sided Z-test that used S (P0) to estimate the standard deviation with a significance level (alpha) of 0.0500. These results assumed that the population proportion under the null hypothesis (P0) was 0.85 [based on an estimated VS rate of 83% for the TLD regimen in 2L-ART] [13]. The study adhered to the principles outlined in the Declaration of Helsinki (1964) and its subsequent amendments. Informed consent was obtained from all participants, and the study was approved by the Institutional Ethics Committee.
2.2. Baseline Assessment
Patients underwent a comprehensive clinical examination, laboratory tests (VL, CD4 cell-count, blood-counts, liver and kidney function, blood sugar, and lipid profile), and assessment for opportunistic infections (OIs). Demographic, ART history, and adverse-event (AE) data were collected, adherence was assessed, and counselling was provided. The baseline DRT was based on assessments of 1L-ART failure.
2.3. Intervention and Follow-up
The study regimen comprised TFV (either TDF or TAF) + 3TC/FTC + DTG as a 2L-ART regimen. The protocol involved follow-up at 24 weeks (closest to the 24 week interval in the week 20-28 window) and extended follow-up at 48 weeks (closest to the 48 week interval in the week 44-52 window). Each visit included clinical examination, anthropometry, VL estimation, adherence assessment, counselling, and evaluation of AEs. Adherence was assessed using the pill-count method, pharmacy refill data, and/or patient interviews. Screening and clinically-guided investigations for OIs were conducted. CD4 cell count was estimated at 24 weeks. Further details on the study protocol can be found in Tables S1-S3.
2.4. Definitions
Virological failure (VF) was defined as the presence of two consecutive VL measurements ≥ 1000 copies/mL, with an intervening 8-12 week period of enhanced adherence support.
DRT utilized population-based Sanger sequencing, covering RT-Codons 1-240, PR-Codons 1-99, and IN-encoding regions using the ViroseqTM HIV-1 Genotyping System (Celera Diagnostics, USA and Thermo Scientific, CA). Drug resistance mutations (DRMs) were classified into four categories: Potential low-level resistance (POT-LLR), Low-level resistance (LLR), Intermediate resistance (IR), and High-level resistance (HLR), based on DRM scores sourced from the Stanford HIV database (HIVDB.Stanford.edu ver. 9.4 as of December 7, 2022) [14].
In this study, an NRTI agent was considered fully active if the sequence indicated either drug Susceptibility (SUS) or POT-LLR, whereas an ART agent was categorized as having no predicted activity if DRT revealed either IR or HLR. To assess the overall susceptibility of antiretroviral (ARV) drugs in the regimen, the Stanford genotypic susceptibility scoring (GSS) was calculated. This score was derived by summing the Stanford Genetic Susceptibility Rating (GSR) assigned to each drug (SUS: 1, POT-LLR: 0.75, LLR: 0.5, IR: 0.25, and HLR: 0.0) [15]. GSS < 2 indicated that there were fewer than 2 fully active drugs in the regimen.
Adverse Events (AEs) were categorized by severity, ranging from mild to potentially life-threatening, and classified according to the Division of AIDS (DAIDS) grading system for adult and paediatric AEs, including Grades 1 through 4 [16].
2.5. Outcomes
Virological outcomes were assessed at both 24 and 48 weeks. The primary outcome was achieving VS to HIV RNA levels < 1000 cp/mL and to < 200 cp/mL at 24 and 48 weeks. Secondary outcomes included immunological reconstitution and drug discontinuation, and death (Table S2).
2.6. Data Collection and Statistical Analysis
Retrospective data from patients' medical records at the institute included baseline demographics (age, sex, hepatitis C, and hepatitis B status, presence of OIs, time since starting 1L-ART, time to 1L-ART failure, exposure to specific ART agents, and adverse events related to 1L-ART). Follow-up data were collected using a semi-structured proforma. Statistical analysis was performed using Microsoft Excel (Microsoft Corporation, Redmond, WA, SA) and IBM SPSS Statistics (IBM SPSS for Windows, Version 23.0, Armonk, NY) for measures of central tendency (mean ± standard deviation or median and interquartile range, depending on sample distribution). Proportions were estimated within 95% confidence intervals (CI) using the One-sample binomial test (Clopper-Pearson 'exact' method) and were compared with a 5% type 1 error. Differences in proportions (ΔPr) with 95% CI were calculated using Stata Statistical Software: release 15 (StataCorp LLC, College Station, TX, USA), employing the default wald method for two-sample proportion tests. Graphs were created using Prism GraphPad 8.1 (GraphPad Software, SD, CA, www.graphpad.com).
3. RESULTS
3.1. Baseline Characteristics
A total of 64 patients were included in the study, with a median age of 42 (IQR: 14, range: 19-62) years, 29.7% (n = 19) female, and a median duration on 1L-ART of 92 (IQR: 91, range: 12–199) months. The majority [62.5% (n = 40)] of patients were switched to the study regimen upon developing 1L-ART failure. The remaining 24 PLH who started 2L-ART prior to the study regimen [dual NRTI + b/PI (n = 14), dual NRTI + b/PI + raltegravir (RAL) (n = 5), AZT + 3TC + DTG (n = 3), PI + DTG (n = 2)], were stable and VS for median 27 (IQR: 20, range: 12-65) months. Table 1 summarizes baseline characteristics and ART histories.
| Baseline Characteristics | N = 64 | Cohort A (n = 17) | Cohort B (n = 24) | Cohort C (n = 11) | Cohort D (n = 12) |
|---|---|---|---|---|---|
| Demography | |||||
| Median age (± IQR, range) years | 42.0 (14, 19-62) | 46 (15, 17-62) | 35.5 (11, 26-55) | 49.0 (13, 16-62) | 45.9 (9, 35-53) |
| Male [% (n)] | 69.2 (45) | 52.9 (9) | 75.0 (18) | 66.7 (8) | 83.3 (10) |
| Female [% (n)] | 29.7 (19) | 47.1 (8) | 25.0 (6) | 27.3 (3) | 16.7 (2) |
| Co-infection | |||||
| HBV [% (n)] | 1.5 (1) | Not detected | Not detected | Not detected | 8.3 (1) |
| HCV and VDRL % [(n)] | Not detected | ||||
| ART history | |||||
| Median duration of first-line ART (± IQR, range) months | 92.0 (91, 12-199) | 118.8 (82.9, 19.4-198.7) | 56.4 (78.0, 12.0-143.63) | 136.8 (60.6, 86.5-194.6) | 92.5 (37.9, 8.0-126.1) |
| Received TFV only in 1L-ART [% (n)] | 38.4 (23) | 0.0 | 70.8 (17) | 0.0 | 50.0 (6) |
| Received both TFV and AZT in 1L-ART [% (n)] | 20.0 (13) | 0.0 | 29.2 (7) | 0.0 | 50.0 (6) |
| Received AZT only in 1L-ART [% (n)] | 43.8 (28) | 100.0 (17) | 0.0 | 100.0 (11) | 0.0 |
| Prior exposure to INSTI in 2L-ART [% (n)] | 13.8 (9) | 5.9 (1) | 0.0 | 36.3 (4) | 33.3 (4) |
| Prior exposure to PIs in 2L-ART [% (n)] | 32.3 (21) | 35.3 (6) | 16.7 (4) | 54.5 (6) | 41.7 (5) |
| Baseline immuno-virological status | |||||
| Virologically suppressed (HIV RNA < 1000 copies/ mL) prior to switch [% (n)] | 34.4 (22) | 41.2 (7) | 16.7 (4) | 45.5 (5) | 50.0 (6) |
| HIV RNA ≥ 1000 prior to switch [% (n)] | 64.6 (42) | 58.8 (10) | 83.3 (20) | 54.5 (6) | 50.0 (6) |
| Baseline Log HIV RNA (median ± IQR, range) Log 10 cp/mL | 4.3 (3.01, 1.3-7.5) | 3.7 (3.2, 1.3-6.1) | 4.9 (1.4, 1.6-6.8) | 3.9 (3.8, 1.3-7.5) | 3.5 (3.7, 1.3-5.8) |
| Baseline CD4 cell count (median ±IQR, range) cells/µL | 239.5 (464.5, 11-871) | 300.0 (333, 16-840) | 87.0 (193.5, 11-871) | 180.0 (434, 56-795) | 327.0 (354.5, 19-674) |
| Baseline CD4 cell count < 200 cells/µL [% (n)] | 46.8 (30) | 29.4 (5) | 58.3 (14) | 54.5 (6) | 41.7 (5) |
| Baseline CD4 cell count ≥ 200 cells/µL [% (n)] | 53.1 (34) | 70.6 (12) | 41.6 (10) | 45.5 (5) | 58.3 (7) |
Switch to the study regimen was done in accordance with guidelines recommendations [5], and available evidence on ART switch strategies [17], and HIVDR as follows: Cohort A (n = 17) received AZT in failing 1L-ART, eligible for the study regimen following the WHO public health approach of optimized second-line NRTI-backbone, while also having full DRT-predicted TFV susceptibility. Cohort B (n = 24) received TFV in a failing 1L-ART regimen, being eligible based on full TFV predicted susceptibility on DRT, but not following the WHO approach, i.e., involving TFV recycling in 2L-ART. Cohort C (n = 11) received AZT in failing 1L-ART, being eligible based on the WHO public health approach despite having no DRT-predicted TFV susceptibility at the time of 1L-ART failure. Subsequently, a fourth group (Cohort D, n = 12) was included, wherein participants who failed on 1L-ART with a TFV backbone and no predicted TFV susceptibility at failure received recycled TFV due to TFV indications or AZT contraindications. Consequently, participants inherently clustered into two main groups for comparison: (i) those receiving the study regimen with full predicted TFV susceptibility (Cohorts A + B), and (ii) those with no predicted TFV susceptibility (Cohorts C + D). Fig. (1) summarizes the study enrolment and switch strategies employed.
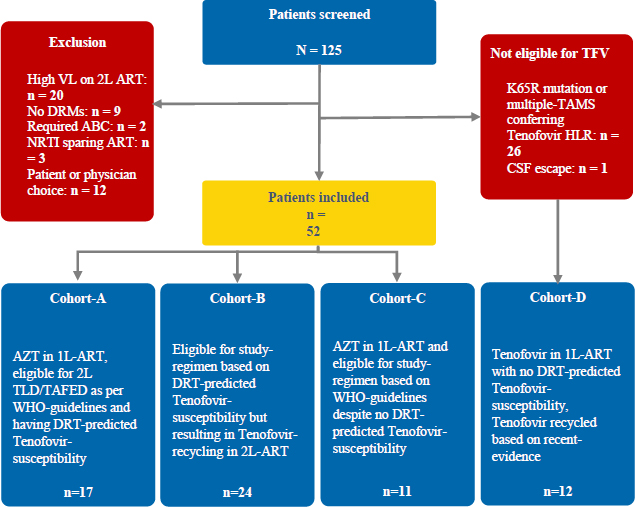
Patient flow chart.
3.2. Drug resistance Profile at First-line ART Failure
HIV-1 genotyping revealed subtype C in all but two patients (subtype A). Overall, 62.5% (n = 40) PLH had GSS < 2 for TFV + 3TC/FTC + DTG regimen, and 35.9% (n = 23) PLH had no predicted TFV susceptibility (IR or HLR to TFV) based on DRT at 1L-ART failure, which included 8 PLH with K65R-DRM, 14 PLH with multiple TAMs compromising TFV, and one patient with coexisting K65R-DRM and multiple TAMs. Four PLH were not detected with NRTI-DRMs, two had PI-DRMs (no PI compromise), and no INSTI-DRMs were found. Specific DRMs and susceptibilities are detailed in Table 2, Figure (S1A-B), and Table S4.
| HIV DRT | N = 64 | Cohort A (n = 17) | Cohort B (n = 24) | Cohort C (n = 11) | Cohort D (n = 12) |
|---|---|---|---|---|---|
| HIV Genotype | |||||
| Subtype C [% (n)] | 96.9 (62) | 94.1 (16) | 100.0 (24) | 100.0 (11) | 91.7 (11) |
| Subtype A [% (n)] | 3.1 (2) | 1.5 (1) | 0.0 | 0.0 | 8.3 (1) |
| Pattern of NRTI DRMs | |||||
| No NRTI DRM [% (n)] | 6.1 (4) | 17.6 (3) | 4.2 (1) | 0.0 | 0.0 |
| M184V/I only or M184V/I + other TFV-selected DRMs (either K70E or Y115F) or single TAM that compromise neither AZT nor TFV (either D67N or K219E) [% (n)] | 40.0 (26) | 41.2 (7) | 79.2 (19) | 0.0 | 0.0 |
| Multiple TAMs [% (n)] | 40.6 (26) | 41.2 (7) | 16.7 (4) | 100.0 (11) | 25.0 (4) |
| TAM 1 DRMs[% (n)] | 18.4 (12) | 17.6 (3) | 12.5 (3) | 18.2 (2) | 25.0 (3) |
| TAM 2 DRMs [% (n)] | 12.3 (8) | 11.8 (2) | 4.2 (1) | 33.3 (4) | 8.3 (1) |
| Mixed TAM 1 + TAM 2 DRMs [% (n)] | 10.8 (7) | 11.8 (2) | 0.0 | 41.7 (5) | 0.0 |
| K65R + M184 V/I ± other non-TAM DRMs [% (n)] | 9.2 (6) | 0.0 | 0.0 | 0.0 | 50.0 (6) |
| K65R + multiple TAMs not resulting in AZT-compromise [% (n)] | 3.1 (2) | 0.0 | 0.0 | 0.0 | 16.7 (2) |
| K65R + multiple TAMs resulting in AZT-compromise [% (n)] | 1.5 (1) | 0.0 | 0.0 | 0.0 | 8.3 (1) |
| PI DRMs [% (n)] | 3.1 (2) | 1.5 (1) | 4.2 (1) | 0.0 | 0.0 |
| INSTI DRMs [% (n)] | 0.0 | ||||
| ART drug susceptibility scores for resistance to TFV | |||||
| Median Stanford resistance score (± IQR, range) | 20 (50, -10-85) | 0 (20, -10-25) | 15 (25, -10-20) | 50 (29, 30-65) | 60 (24, 30-85) |
| Stanford resistance score < 15 [% (n)] | 36.9 (24) | 70.6 (12) | 50.0 (12) | 0.0 | 0.0 |
| Stanford resistance score 15- < 30 [% (n)] | 26.2 (17) | 29.4 (5) | 50.0 (12) | 0.0 | 0.0 |
| Stanford resistance score 30- < 60 [% (n)] | 10.0 (13) | 0.0 | 0.0 | 75.0 (9) | 33.3 (4) |
| Stanford resistance score ≥ 60 [% (n)] | 15.6 (10) | 0.0 | 0.0 | 18.2 (2) | 66.7 (8) |
| Level of resistance to tenofovir | |||||
| Sus, POT-LLR or LLR % [% (n)] | 63.1 (41) | 100.0 (17) | 100.0 (24) | 0.0 | 0.0 |
| IR or HLR* % [% (n)] | 35.9 (23) | 0.0 | 0.0 | 100.0 (11) | 100.0 (12) |
| Resistance to 3TC/FTC | |||||
| Sus, POT-LLR, or LLR % [% (n)] | 7.7 (5) | 23.5 (4) | 4.2 (1) | 0.0 | 0.0 |
| IR or HLR* % [% (n)] | 92.2 (59) | 76.5 (13) | 95.8 (23) | 100.0 (11) | 100.0 (12) |
| Susceptibility to background therapy | |||||
| GSS ≥ 2 (for the regimen TFV + 3TC/FTC + DTG) [% (n)] | 36.9 (24) | 76.5 (13) | 45.8 (11) | 0.0 | 0.0 |
| GSS < 2 (for the regimen TFV + 3TC/FTC + DTG) [% (n)] | 62.5 (40) | 23.5 (4) | 54.2 (13) | 100.0 (11) | 100.0 (12) |
| Both TFV and 3TC/FTC fully active¶ [% (n)] | 7.7 (5) | 23.5 (4) | 4.2 (1) | 0.0 | 0.0 |
| TFV fully active but no predicted susceptibility to 3TC/FTC¶ [% (n)] | 55.4 (36) | 76.5 (13) | 95.8 (23) | 0.0 | 0.0 |
| No predicted susceptibility to both TFV and 3TC/FTC¶ [% (n)] | 35.9 (23) | 0.0 | 0.0 | 100.0 (11) | 100.0 (12) |
3.3. Primary Outcome
The primary analysis utilized the full analysis set (FAS) and OTT, where FAS included all PLH starting the study regimen (TFV + 3TC/FTC + DTG), while OTT excluded PLH with major protocol deviations, such as those with poor adherence or treatment discontinuation/interruption, and non-virological reasons for regimen alteration. Participants transferred out for non-VF reasons, those lost to follow-up (LFU), participants with missing VL-data in the window, and those deceased from non-HIV non-drug causes or from HIV-related causes with onset prior to enrolment were excluded.
At 24 weeks, six PLH were excluded (5 LFU, 1 died), leaving 58 in the FAS. Excluding two PLHs (treatment discontinuation) for protocol deviations, the OTT analysis included 56 PLHs. Overall, three patients met the criteria for VF (2x HIV RNA ≥ 1000 cp/mL), resulting in VS rates of 94.6% (95% CI: 85.1-98.9, n = 53/56) PLH. VS to HIV RNA < 200 cp/mL was attained in 92.8% (95% CI: 82.7-98.1, n = 52/56) in the OTT analysis Fig. (2). Sensitivity analysis is reported in Table S5.
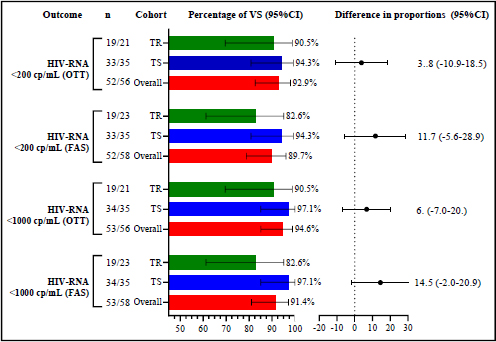
The differences in proportions of participants achieving the primary outcome across the different cohorts at 24 weeks. The red, blue, and green bars represent the whole cohort, TFV-susceptible (TS) and TFV-resistant (TR) groups, respectively. These bars indicate the percentage of PLH who achieved the primary outcome of VS to HIV RNA < 1000 cp/mL and < 200 cp/mL. Error bars display 95% confidence intervals. The forest plot illustrates the difference in proportions of participants achieving the primary outcome across cohorts, using the TR group as the reference. FAS: Full analysis set, OTT: On treatment, TFV: Tenofovir, TS: TFV-susceptible, TR: TFV-resistant, VS: Virological suppression.
Among PLH with no predicted TFV susceptibility, 90.5% (95% CI: 69.2-98.8, n = 19/21) achieved VS in OTT, while 97.1% (95% CI: 85.1-99.1, n = 34/35) with full TFV susceptibility attained VS. For HIV RNA < 200 cp/mL, 90.5% (95% CI: 69.6-69.2, n = 19/21) of those without predicted TFV susceptibility and 94.3% (95% CI: 80.8-99.3, n = 33/35) with full TFV susceptibility achieved VS Fig. (2).
At 48 weeks, one patient died from multidrug-resistant (MDR)-TB (not due to VF, attained VS at 24 weeks), and three were LFU, resulting in their exclusion. One patient switched to RAL due to an AE from DTG, and another discontinued treatment, leading to exclusions from the OTT analysis.
Out of 54 patients in the FAS, only one (who discontinued) met the criteria for VF. The OTT analysis showed 100% VS among 52 patients. For HIV RNA < 200 cp/mL, 96.2% (95% CI: 86.83-99.5, n = 50/52) in OTT achieved VS. In the OTT analysis, all patients with no predicted TFV susceptibility (100%, 95% CI: 83.2-100, n = 20/20) attained VS <200 cp/mL, compared to 93.8% (95% CI: 79.2-99.2, n = 30/32) with full TFV susceptibility (Fig. 3).
Participants excluded from the 24 week OTT analysis due to treatment discontinuation/interruption had distinct outcomes. One patient achieved VS at 48 weeks with enhanced adherence interventions, while the other responded during a brief hospitalization but did not attain VS during subsequent follow-up at 48 weeks. Repeat DRT showed no new resistance to DTG or TFV in this patient (Table S13).
Further, cohort-wise analysis, based on ART switch strategies, and subgroup analyses stratified by (i) GSS score, (ii) receipt of recycled TFV vs. receiving TFV for the first time, and (iii) initiation of 2L-ART before switching to the study regimen vs. a direct switch after 1L-ART, showed consistent VS rates across sub-cohorts. Detailed outcomes are presented in Tables S6-S9.
3.4. Secondary Outcomes
At 24 weeks, the median (IQR, range) CD4 cell count was 428 (352, 110-1105) cells/µL, reflecting a median change of 140 (95% CI: 95-187) cells/µL (Hodges-Lehman median difference) from baseline median (IQR, range) CD4 cell count of 250 (404, 11-871) cells/µL. The indications for TFV in participants who received recycled TFV in the absence of TFV susceptibility at 1L-ART failure are elaborated in Table S10, and potential drug-drug interactions are in Table S11. Fatal outcomes occurred in two participants (Table S12).
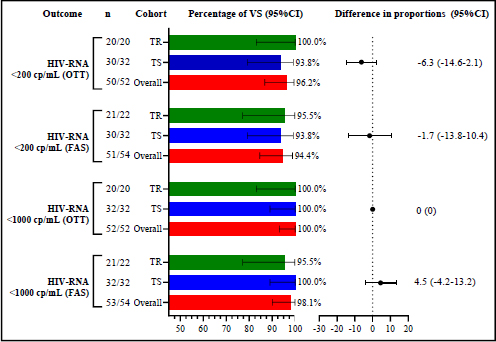
Illustrates the differences in proportions of participants achieving the primary outcome across the different cohorts at 48 weeks. The red, blue, and green bars represent the whole cohort, TFV-Susceptible (TS) and TFV-Resistant (TR) groups, respectively. These bars indicate the percentage of PLH who achieved the primary outcome of VS to HIV RNA < 1000 cp/mL and < 200 cp/mL. Error bars display 95% confidence intervals. The forest plot illustrates the difference in proportions of participants achieving the primary outcome across cohorts, using the TR group as the reference. FAS: Full analysis set, OTT: On treatment, TFV: Tenofovir, TS: TFV-susceptible, TR: TFV-resistant, VS: Virological suppression.
4. DISCUSSION
DTG is the preferred second-line core antiretroviral drug due to its effectiveness and resistance barrier. The SAILING trial demonstrated lower VF rates with DTG than Raltegravir in PLH who developed resistance to at least two ART classes while on a Non-Integrase Strand-Transfer Inhibitor (INSTI) based therapy [17]. The DAWNING trial supported the use of dual-NRTI + DTG by demonstrating the superiority of dual-NRTI + DTG to ritonavir-boosted lopinavir (L/r) at 48 weeks in PLH with VF on a 2NRTI + NNRTI-based 1L-ART, provided that at least one of the two NRTIs was fully active on DRT. Given the impracticality and limitations of resistance-testing in resource-limited settings, the WHO recommends DTG with an optimized NRTI for those failing first-line NNRTI treatment [18], sparking a debate about what constitutes ‘an effective optimized NRTI backbone.’
The WHO approach to optimizing the NRTI backbone hinges on prior NRTI use, often necessitating a switch from TFV to AZT, a drug with notable drawbacks. AZT is known to have both short and long term side effects, increases pill burden with its twice-daily dosing, and requires intricate monitoring [5, 12]. The primary concern dictating this switch is the level of resistance to the NRTI backbone and the associated loss of viral fitness during replication. Being on a recycled TFV-based regimen could be similar to taking monotherapy or dual therapy, both of which carry an increased risk of resistance. Although DTG resistance is rare among patients on second-line therapy and with viraemia on DTG, it can occur [19, 20].
Recent studies have examined the feasibility of utilizing recycled TFV in 2L-ART for patients who have failed first-line TFV-based regimens. However, a definitive consensus remains elusive. The 2024 WHO update mentions this possibility but lacks specific guidelines [19]. Evidence stems from three randomised trials and one single-arm trial. The single-arm prospective ARTIST trial was the first to demonstrate that recycling TFV and 3TC with DTG in a single-tablet regimen is effective [12, 13, 21]. The NADIA trial revealed that recycling TFV in second-line therapy was as effective as switching to AZT for VS at 48 weeks. It concluded that switching to AZT during the transition to 2L-ART was unnecessary [22, 23]. Ongoing trials, VISEND and D2EFT, also support using DTG with TDF as non-inferior to AZT and protease inhibitors like lopinavir and darunavir [24, 25]. Additionally, indirect evidence from cohorts like the EA-IeDEA cohort and the GHESKIO cohort further substantiates this approach [26, 27].
Despite these findings, the effectiveness of this single-tablet regimen in people living with HIV (PLH) who have intricate ART histories, exposure to multiple NRTI agents, and DRMs conferring multi-NRTI resistance remains underexplored. The role of drug resistance testing in making treatment decisions for these patients also requires further examination.
To build on this emerging evidence, our study focused on the virological outcomes in patients on 2L-ART with TFV + 3TC/FTC + DTG, enrolling consecutive patients who needed 2L-ART with TFV + 3TC/FTC + DTG, many of whom had previously received TFV in their failing 1L-ART regimen. Eligibility was based on predicted TFV susceptibility from DRT at 1L-ART failure. Patients who initially received AZT in 1L-ART were also transitioned to our study regimen, following WHO guidelines, even if DRT predicted no TFV susceptibility [5]. This is important given the complex ART histories, where previous treatments may have caused resistance mutations like TFV resistance from AZT-induced TAMs. Notably 40% of our cohort had been exposed to both AZT and TFV.
Our study differs from the ARTIST trial, which analyzed 60 patients who had failed 1L-ART [12, 13, 21]. We included a more diverse group, including those with no predicted TFV susceptibility at first-line failure, patients receiving recycled TFV in second-line therapy, and some starting TFV for the first time in 2L-ART despite lacking predicted susceptibility. Our main comparison was between patients with full TFV susceptibility (Cohorts A + B) and those with no TFV susceptibility (Cohorts C + D), including those receiving recycled TFV. Moreover, our study included patients with a historical record of DRMs at first-line failure who were stable on various 2L-ART regimens before switching to our study regimen. However, it is well documented that DRMs that have been identified on historical resistance test reports are considered archived and are known to persist within integrated HIV genomes, potentially reemerging during subsequent therapy lacking effective medications [28-30].
In the 48 week OTT cohort (n = 52), 21.2% (11/52) had no predicted tenofovir susceptibility due to the accumulation of multiple thymidine analogue mutations (TAMs). The K65R mutation was detected in 17.3% (9/52) overall and in 28.1% (9/32) of those who received recycled tenofovir, which is lower than the 37% (n = 20; modified intention-to-treat analysis (mITT) analysis) reported in the ARTIST study [12, 13, 21]. Overall, 42.6% of our patients lacked predicted TFV susceptibility at first-line failure, compared to 65% in ARTIST [12, 13, 21]. This difference is mainly due to our stricter resistance threshold, using a stanford score of ≥ 30 [31] to define no predicted TFV susceptibility, compared to ≥ 15 in the ARTIST study [12, 13, 21].
Despite these differences, our study achieved high VS rates with 2L-ART (TFV + 3TC/FTC + DTG). At 24 weeks, 94.6% of patients had HIV RNA < 1000 cp/mL, and 92.8% had HIV RNA < 200 cp/mL. Among those on recycled TFV, 93.8% reached VS, similar to the 95% (modified intention-to-treat analysis, mITT) rate of VS to HIV RNA < 400 cp/mL in ARTIST [12, 13, 21]. Patients without predicted TFV susceptibility had slightly lower rates of VS to HIV RNA < 200 cp/mL (90.4%) compared to those with susceptibility (94.3%). In contrast, the ARTIST trial reported 97.1% (mITT) VS to HIV RNA < 400 cp/mL in patients with TFV-resistance [12, 13, 21].
By 48 weeks, none of our patients experienced VF (OTT analysis), and 96.2% achieved VS to HIV RNA < 200 cp/mL. This included patients without predicted TFV susceptibility, those on recycled TFV, as well as individuals with K65R-DRM or multiple TAMs compromising TFV effectiveness. These findings compare favourably with the ARTIST trial, where 89% of patients on recycled TFV achieved suppression at < 400 cp/mL [12, 13, 21]. Similarly, the NADIA trial showed 92% suppression at < 400 cp/mL with a DTG-based regimen, even in those with no predicted NRTI activity [22, 23].
The findings from our study support the effectiveness of DTG combined with a recycled TFV backbone as a viable 2L-ART regimen. The once-daily fixed-dose combination of TDF (or TAF) + 3TC (or FTC) + DTG, available through the Indian National AIDS Control Programme, offers a safe, well-tolerated, and convenient single-tablet option. This regimen minimizes side effects associated with AZT, reduces pill burden, and simplifies monitoring requirements [5, 12]. These findings are especially trivial considering the observation that 20% of our study cohort who received their 1L-ART under the National programme were exposed to both TFV and AZT, in which case, selection of an optimized NRTI backbone in 2L-ART becomes a dilemma.
However, our study has certain limitations that should be considered. This is a small-scale investigation that contributes to the emerging evidence supporting the use of recycled TFV in 2L-ART, particularly suggesting effectiveness even in patients without predicted TFV susceptibility based on DRT at 1L-ART failure. Assessing the virological effectiveness of ART regimens, especially regarding genotypic drug-susceptibility, remains challenging in resource-limited settings where DRT is still a nascent modality of investigation. Additionally, although the follow-up of patients in our study was pragmatic for clinical practice, our patient selection was guided by guidelines recommending specific indications for TFV in 2L-ART, particularly in the cohort receiving recycled TFV without TFV susceptibility. Larger studies are needed to validate and generalize our findings more broadly. Finally, sensitivity analysis indicated that our data is sensitive to treatment discontinuation/interruption and/or poor adherence, and our interpretations are based on OTT analysis.
Despite these limitations, this study is the first in India to evaluate 2L-ART regimens across varied ART histories and DRT results. It addresses key gaps in optimizing NRTI backbones in 2L-ART and provides initial evidence supporting the use of recycled TFV with DTG, either after failure of 1L-ART or when both NRTIs are compromised.
5. LIMITATIONS AND CRITICAL DISCUSSION
Despite the encouraging findings, this study has several important limitations that warrant discussion. Methodological features of the study were designed to address these limitations wherever feasible.
5.1. Small Sample Size and Single-center Design
This study was conducted at a single tertiary care hospital with a relatively small cohort. Although the sample size was adequately powered for the primary outcome, it limited the ability to detect statistically significant subgroup differences, especially among participants with complex resistance patterns. Nonetheless, the pragmatic design utilizing routine clinical practices and adherence to WHO public health guidelines supports external validity in comparable resource-limited settings.
5.2. Non-randomised, Observational Study Design
The lack of a randomised control group limits the ability to establish causal associations. However, the prospective nature of the study enabled structured and systematic data collection with consistent follow-up. Stratification of participants into cohorts based on TFV susceptibility and ART history facilitated meaningful internal comparisons. This real world design reflects clinical decision-making in resource-constrained environments.
5.3. Heterogeneity in ART Histories and Regimen Switches
Participants had diverse ART exposures and varying durations on prior regimens, contributing to clinical heterogeneity. To mitigate this, the study incorporated predefined cohort stratification based on ART history and genotypic resistance profiles.
5.4. Reliance on Historical Drug Resistance Testing
Drug resistance testing data used for regimen selection were obtained at the time of 1L-ART failure. While this may not accurately reflect subsequent resistance evolution, it is consistent with WHO and national programmatic guidelines. Additionally, archived mutations identified on historical resistance assays are known to persist within latent viral reservoirs and can reemerge, supporting the clinical utility of such data in guiding second-line therapy.
5.5. Limited Duration of Follow-Up
The study assessed virological suppression over 48 weeks, which is sufficient to evaluate short- to mid-term outcomes but may not capture long term durability. The cohort is being followed up for long term outcomes with the aim of determining the sustained efficacy and safety of regimens containing DTG in combination with a potentially compromised NRTI backbone.
5.6. On-Treatment Analysis and Potential for Adherence Bias
The primary outcome analysis was conducted using an On-Treatment (OTT) approach, which excludes individuals who discontinued therapy, were lost to follow-up, or had missing virological data. This has the potential to overestimate treatment effectiveness. However, sensitivity analyses were performed, and the reasons for exclusion were clearly documented. The OTT approach was considered appropriate for evaluating regimen efficacy under conditions of confirmed adherence, thereby providing a realistic estimate of expected performance in well-managed clinical settings.
CONCLUSION
This study provides valuable insights into the virological effectiveness of 2L-ART regimens comprising TFV + 3TC/FTC + DTG in a real world clinical setting. Despite a significant proportion of participants lacking predicted TFV susceptibility due to DRMs identified on the basis of DRT at 1L-ART failure, high virological suppression rates were observed at both 24 and 48 weeks. These findings reinforce the potential of DTG-based 2L-ART regimens in diverse clinical scenarios, particularly those with a potentially compromised NRTI backbone.
Our study demonstrated that clinical decisions based on pragmatic implementation of WHO guidelines-such as continuing TFV despite lack of genotypic susceptibility-can result in successful outcomes, particularly when combined with DTG, which has a high genetic barrier to resistance. This outcome supports the feasibility of simplified, once-daily, fixed-dose combinations as viable options for second-line therapy, especially in resource-constrained settings where alternatives, like AZT, pose challenges in terms of toxicity, adherence, and monitoring requirements.
The study’s results align with and support the findings from trials, such as ARTIST and NADIA, while also offering novel insights specific to the Indian context. It is especially relevant considering the high proportion of PLH exposed to both TFV and AZT during their treatment history, as well as the sparse use of VL testing under national ART programmes, and the inaccessibility of genotypic drug resistance testing facilities. Thus, our findings contribute to the evolving evidence base informing 2L-ART strategies.
DECLARATION
Parts of the study were presented as a poster at CIDSCON 2024, Hyderabad, India. The authors take full responsibility for the statement that no exclusively AI-generated text has been incorporated into the manuscript.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: S.A.: Study conception and design; D.S.: Data curation; N.R.: Data analysis or interpretation; K.A.: Validation; N.K. and A.A.: Draft manuscript;. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| AE | = Adverse Event |
| AZT | = Zidovudine |
| CD4 | = Cluster of Differentiation 4 (a type of T-cell) |
| DAIDS | = Division of AIDS (U.S. National Institutes of Health) |
| DRM | = Drug Resistance Mutation |
| DRT | = Drug resistance Testing |
| DTG | = Dolutegravir |
| FDA | = U.S. Food and Drug Administration |
| GFR | = Glomerular Filtration Rate |
| GSS | = Genotypic Susceptibility Score |
| HIV | = Human Immunodeficiency Virus |
| HIVDR | = HIV Drug Resistance |
| IQR | = Interquartile Range |
| INSTI | = Integrase Strand Transfer Inhibitor |
| IR | = Intermediate Resistance |
| LLR | = Low Level Resistance |
| MDR-TB | = Multidrug Resistant Tuberculosis |
| NRTI | = Nucleoside Reverse Transcriptase Inhibitor |
| PLH | = People Living with HIV |
| POT-LLR | = Potential Low-Level Resistance |
| PR | = Protease |
| RT | = Reverse Transcriptase |
| TAMs | = Thymidine-Analog Mutations |
| TAF | = Tenofovir Alafenamide |
| TDF | = Tenofovir Disoproxil Fumarate |
| TFV | = Tenofovir |
| VS | = Virological Suppression |
| WHO | = World Health Organization |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The ethical approval was obtained from the Institutional Ethics Committee of Base Hospital and Army College of Medical Sciences, Delhi Cantt, India (No. SRC/01/2023/10).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
All the data and supporting information are provided within the article.
ACKNOWLEDGEMENTS
We acknowledge the contributions of Metropolis Healthcare Pvt. Ltd. for providing detailed drug resistance reports and the Stanford HIV Drug Resistance Database for invaluable assistance. Special thanks to Mr. Mahipal Singh, Ms. Preeti Singh, and Mr. Ambare for their assistance with data compilation. The authors also acknowledge the use of Generative Pre-trained Transformer-3.5 [GPT-3.5, OpenAI (2023)] for language guidance.

