All published articles of this journal are available on ScienceDirect.

Evaluation of the Effect of Neurofeedback on Polysomnographic Changes and Improvement in the Life Quality of People with HIV with Sleep Disorders: A Clinical Trial Study
Authors Info & Affiliations
Abstract
Introduction
Sleep disorders are considered as one of the most common illnesses among people with HIV. Due to this, using neurofeedback devices to alter brain waves is implemented as a complementary therapy. The aim of this study was to evaluate the effectiveness of neurofeedback on changes in interrupted sleep, duration of sleep, restless legs syndrome, and improve the quality of life in people with HIV with sleep difficulties.
Methods
The current study is a clinical trial and applied type of research in which the pre-test and post-test of two interventional and placebo groups were compared. The statistical population of all patients referred to the HIV Research Center of Imam Khomeini Hospital Complex was selected randomly. In this respect, 15 volunteer patients (9 volunteers in the treatment group and 6 volunteers in the placebo group) were chosen and placed into groups via random sampling. In addition, the Pittsburg Sleep Quality Index (PSQI) was used for the evaluation of sleep quality. Data were analyzed after statistical analysis through standard tests.
Results
The results of this study showed that neurofeedback was able to cause significant changes in reducing stress levels. This treatment was able to improve the quality of life indicators in participants. Also, there were changes in polysomnographic data; however, they were not significant.
Conclusion
Based on these data, Neurofeedback therapy could be considered a complementary therapy to improve sleep disorders in people with HIV.Moreover, this treatment was able to improve the quality of life and stress indicators in these patients by improving brain waves.
1. INTRODUCTION
As an indicator of well-being, sleep quality can adversely affect medical conditions. In clinical populations, poor sleep quality is linked to increased co-morbidities, mortality, healthcare costs, and a decline in the quality of life [1]. Sleep disturbances are defined as trouble initiating and maintaining sleep or early morning awakening [2]. A number of biological factors contribute to poor sleep quality in HIV-infected patients. These factors include involvement of the central nervous system (CNS), opportunistic infections, immune dysfunction, antiretroviral side effects, and psychosocial distress [3].
There are several adverse consequences associated with poor sleep quality in the HIV-infected population [4]. These consequences include an impact on quality of life, diminishing sleep duration, exacerbated restless leg syndrome, and cognitive impairment [5]. The causes of sleep impairment may be difficult to distinguish at this stage, especially in the advanced stage, as patients may also be experiencing a great deal of anxiety related to the medication as well as the HIV virus, which may interfere with sleep [6]. Despite this fact, little attention has been paid to this condition. Sleep disturbances are generally measured as a normal consequence of HIV infection, and their treatment is usually considered insignificant in comparison to other complications [7]. Therefore, some medications, such as novel neurofeedback therapy, which is an effective complementary therapy with few side effects, can improve these conditions in HIV patients and are required [8].
The short-term nature of neurofeedback, the lack of side effects, and the effects on brain waves and interactions make it an attractive alternative to pharmacological interventions [9]. Experimental and theoretical studies have examined the effects of neurofeedback on the immune system, as well. A hypothesized effect of neurofeedback training on the extensive bidirectional neuronal connections and feedback loops between the CNS and immune system, as well as subsequent general quality of life of HIV-positive people, has been proposed since neurofeedback training impacts brain function at the neuronal level [10, 11].
In the present study, we examined key factors related to treatment outcomes and psychological problems experienced by people with HIV that could be managed by healthcare providers. The purpose of this study was to identify the magnitude and associated factors of sleep quality in one of the largest referral hospitals located in Tehran, Iran, for people, unfortunately, living with HIV.
2. MATERIALS AND METHODS
2.1. Study Participants
This study examined 30 people with HIV referred to a sleep clinic at the Imam Khomeini Hospital Complex in Tehran, Iran, between October and March 2020. Participants were divided into two groups: a treatment group (9 individuals) and a placebo group (6 individuals), and a total consisted of 15 individuals. In this study, to evaluate health-related quality of life, two questionnaires were used: HIV/AIDS Quality of Life (HAT-QoL)/SF-36, Depression Anxiety Stress Scales (DASS), and Pittsburgh Sleep Quality Index (PSQI). A total of five subscales are included in this questionnaire, including (1) sleep quality, (2) sleep latency, (3) sleep duration, (4) sleep efficiency, and (5) sleep medication use. The PSQI is the most validated instrument used in research to assess global sleep quality in HIV-positive individuals (Sleep disorder was identified with the PSQI questionnaire). DASS refers to three self-report measures assessing negative emotional states, such as depression, anxiety, and stress [12]. Based on the validated Persian version of DASS, we measured depression, anxiety, and stress on a Likert scale of 0 to 3. The higher the score, the greater the degree of depression, anxiety, and stress.
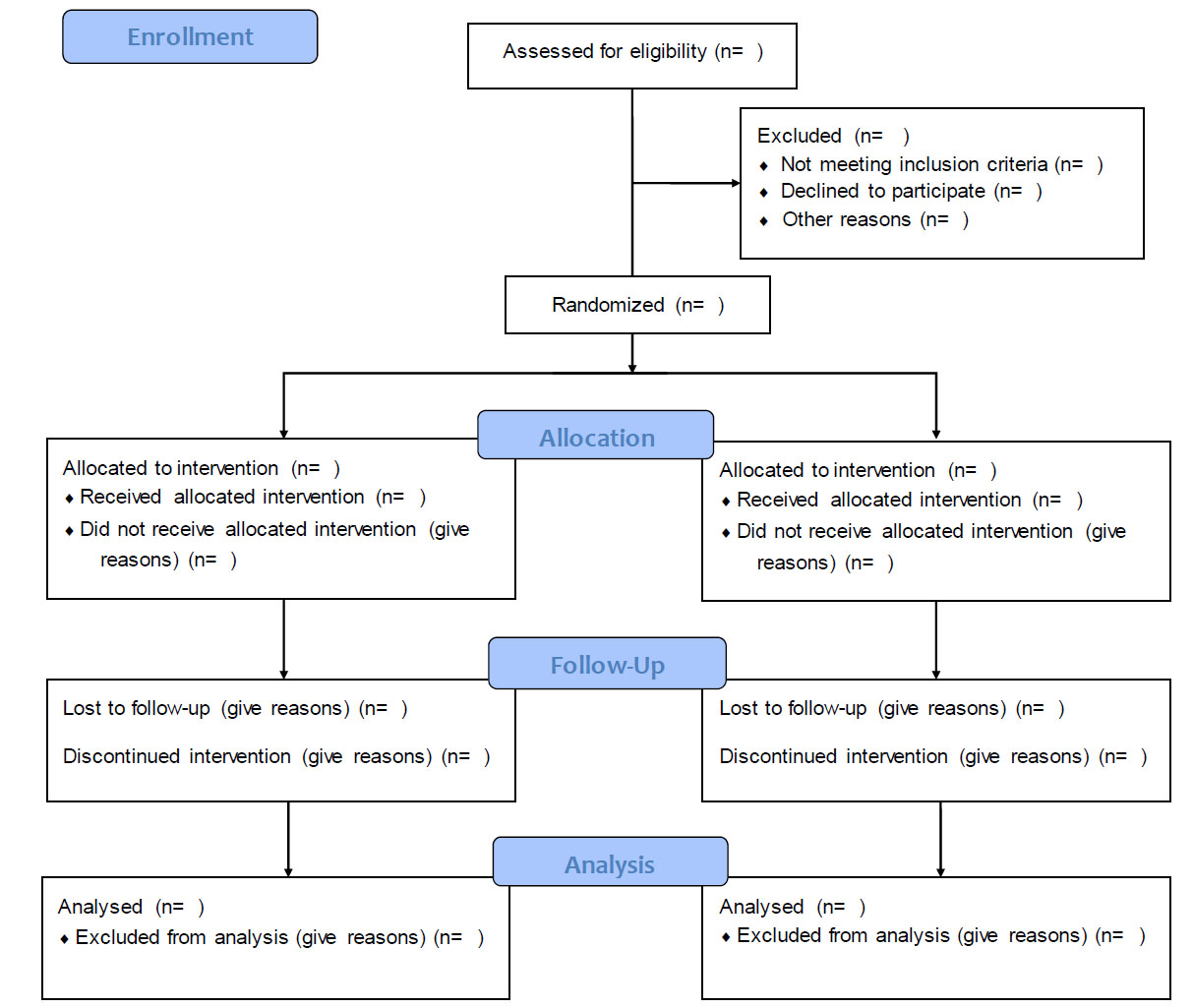
Additionally, we collected patient demographic information and medical histories, including gender, age, education, marital status, history of heart and lung disease or diabetes, body mass index (BMI), employment status, CD4+ T cell count, and co-infections with tuberculosis and hepatitis B. The inclusion criteria were as follows: all participants were older than 18 and younger than 50 years old (The age group of 18 to 50 years was selected based on the clinic visits, and there were no clients above or below this age), they had no history or symptoms of psychotic disorders, no history or symptoms of convulsions, had a diagnosis of one of the sleep disorders based on the PSQI questioner; and provided consent to participate in the study. The exclusion criteria were as follows: history or symptoms of convulsions, history of usage of hypnotic drugs, and history of usage of ECT (People who undergo hypnotic drugs have different brain waves from normal people, and these people were excluded from the study) (Fig. 1).
2.2. Neurofeedback Training
With the EEG neurofeedback system, linked ears were used with the active electrode at Oz (occipital midline). A tone was provided to the subjects when the alpha frequency (12–15 Hz) exceeded their initial testing frequency (2 minutes with eyes open). During neurofeedback, subjects were continuously monitored for EEG activity to prevent them from drifting into sleep. If the EEG deteriorated into sleep, the assigned investigator would tell the subject to refocus on the tone. The reward tone was shifted to a slightly lower frequency (low beta, 4–8 Hz, high theta, 25–30 Hz) after subjects maintained an alpha amplitude of double the baseline level for 20 minutes; training continued for a total of 16 weeks.
2.3. Polysomnography (PSG) Test
A polysomnography test was conducted during a night hospitalization of patients. The respiratory hypopneas of patients, their Leg Movement Index, and the Snoring Index (SI), were recorded.
2.4. Statistical Analysis
In the case of categorical variables, frequency and percentage were used to describe the characteristics, and for continuous variables, means and standard deviations were employed. In order to analyze all of the results, SPSS software (version 26) was used, using a t-test analysis. Statistical significance was p < 0.05 level for all analyses.
3. ETHICAL CONSIDERATIONS
Participants completed self-administered instruments in the waiting room of the sleep clinic while waiting for their medical appointment and provided written consent.
4. RESULTS
In this study, 15 people with HIV (15 males) with the mean and standard deviation of age were 25 ±1 and 45 ± 1, respectively. According to previously defined guidelines, all subjects completed the entire 16-week study along with the entire symptom questionnaire at each study visit.
4.1. WHO Quality-of-Life Brief Questionnaire
Table 1 shows the quality of life associated with participants in our study. The most satisfied parameters of this index in our study were medical treatments and special medical instructions (60%), health service (60%), transportation facilities (53.3%), support of friends (33.3%), level of anxiety (33.3%), social relationship (26.6%), and life facilities (26.6.%). In comparison, the least fulfilled index of quality of life questionnaire included enjoyment in life (6.6%), life safety and security (6.6%), level of environmental health (6.6%), level of energy (6.6%), level of appearance (6.6%), money availability (6.6%) and sleep (6.6%).
| Variables | Satisfied | Dissatisfied | Completely Dissatisfied | Neither Satisfied nor Dissatisfied | ||||
|---|---|---|---|---|---|---|---|---|
| No (%) | No (%) | No (%) | No (%) | |||||
| Treatment | Placebo | Treatment | Placebo | Treatment | Placebo | Treatment | Placebo | |
| Quality of life | 1 (6.6) | 2 (13.3) | 1 (6.6) | - | 2 (13.3) | - | 5 (33.3) | 4 (26.6) |
| Level of health condition | 2 (13.3) | 2 (13.3) | 3 (20) | 2 (13.3) | - | 1 (6.6) | 4 (26.6) | 1 (6.6) |
| Level of physical condition | 2 (13.3) | 2 (13.3) | - | - | 1 (6.6) | - | 6 (60) | 4 (26.6) |
| Medical treatments and special medical instructions | 6 (60) | 3 (20) | 1 (6.6) | 1 (6.6) | - | 1 (6.6) | 2 (13.3) | 1 (6.6) |
| Enjoy from life | 1 (6.6) | 1 (6.6) | 4 (26.6) | 3 (20) | - | - | 4 (26.6) | 2 (13.3) |
| Life value | 3 (20) | 1 (6.6) | 3 (20) | 1 (6.6) | - | - | 3 (20) | 4 (26.6) |
| Life safely and security | 1 (6.6) | - | 3 (20) | 3 (20) | 5 (33.3) | 3 (20) | - | - |
| Level of concentration | - | 2 (13.3) | 1 (6.6) | - | 4 (26.6) | 2 (13.3) | 4 (26.6) | 2 (13.3) |
| Level of environmental health | 1 (6.6) | 2 (13.3) | - | - | 4 (26.6) | 1 (6.6) | 4 (26.6) | 3 (20) |
| Level of energy | 1 (6.6) | - | 2 (13.3) | 5 (33.3) | - | - | 6 (60) | 1 (6.6) |
| Level of appearance | 1 (6.6) | 2 (13.3) | 4 (26.6) | - | - | - | 4 (26.6) | 4 (26.6) |
| Money availability | 1 (6.6) | - | 5 (33.3) | - | - | - | 3 (20) | 6 (60) |
| Daily news availability | 3 (20) | 2 (13.3) | 5 (33.3) | 1 (6.6) | - | - | 1 (6.6) | 3 (20) |
| Personal interest availability | - | 1 (6.6) | 4 (26.6) | 3 (20) | - | - | 5 (33.3) | 1 (6.6) |
| Work capacity | 2 (13.3) | 1 (6.6) | 4 (26.6) | 2 (13.3) | 1 (6.6) | - | 2 (13.3) | 3 (20) |
| Sleep | 1 (6.6) | - | 4 (26.6) | 2 (13.3) | 3 (20) | - | 1 (6.6) | 4 (26.6) |
| Daily activity | 2 (13.3) | 2 (13.3) | 4 (26.6) | 1 (6.6) | - | - | 3 (20) | 3 (20) |
| Social relationship | 4 (26.6) | 4 (26.6) | 1 (6.6) | - | - | - | 4 (26.6) | 2 (13.3) |
| Sex | - | 4 (26.6) | 4 (26.6) | - | 1 (6.6) | - | 4 (26.6) | 2 (13.3) |
| Support of friends | 5 (33.3) | 1 (6.6) | 2 (13.3) | 3 (20) | - | - | 2 (13.3) | 2 (13.3) |
| Life facilities | 4 (26.6) | 3 (20) | 1 (6.6) | 1 (6.6) | - | 1 (6.6) | 4 (26.6) | 1 (6.6) |
| Health service | 6 (60) | 1 (6.6) | 1 (6.6) | 2 (13.3) | - | - | 2 (13.3) | 3 (20) |
| Transportation facilities | 5 (33.3) | 1 (6.6) | 1 (6.6) | 2 (13.3) | - | - | 3 (20) | 3 (20) |
| Level of anxiety | 5 (33.3) | 1 (6.6) | - | 1 (6.6) | - | 1 (6.6) | 4 (26.6) | 3 (20) |
| Variables | Normal | Slight | Medium | Intense | Very Intense |
|---|---|---|---|---|---|
| No (%) | No (%) | No (%) | No (%) | No (%) | |
| Depression | 4 (26.7) | 2 (13.3) | 1 (6.7) | 5 (33.3) | 3 (20) |
| Treatment | 6 (40) | 3 (20) | - | 3 (20) | 3 (20) |
| Placebo | - | - | - | 3 (50) | 3 (50) |
| Anxiety | 8 (53.3) | 2 (13.3) | 1 (6.7) | 1 (6.7) | 3 (20) |
| Treatment | 9 (60) | 1 (6.7) | 1 (6.7) | 1 (6.7) | 3 (20) |
| Placebo | - | 1 (16.7) | 1 (16.7) | 1 (16.7) | 3 (50) |
| Stress | 3 (20) | 3 (20) | 1 (6.7) | 4 (26.7) | 4 (26.7) |
| Treatment | 7 (46.7) | 2 (13.3) | - | 2 (13.3) | 4 (26.7) |
| Placebo | - | - | - | 2 (33.3) | 4 (66.7) |
4.2. Depression Anxiety Stress Scales (DASS) Questionnaire
Table 2 illustrates the association between depression, anxiety and stress among participants. A comparison of these characteristics between the two groups of patients in the treatment group showed that treatment in the stress group can improve the normal life of these patients significantly (p < 0.05). Our results showed that about 60% and 40% of our patients with anxiety and depression reached to normal state with treatment in this study, respectively. Results of the placebo group demonstrated equality between this group and the treatment group in depression, anxiety and stress parameters versus the treatment group.
4.3. Pittsburgh Sleep Quality Index
Table 3 explains the sleep quality index. Therefore, significant or descriptive mean differences were observed over time and also between groups for sleep latency (13.3%), duration (53.3%), and efficiency (53.3%), except for sleep quality and sleep medication, which showed no significant differences among treatment and placebo groups.
| Variables | 0.00 | 1.00 | 2.00 | 3.00 |
|---|---|---|---|---|
| No (%) | No (%) | No (%) | No (%) | |
| Subjective sleep quality (treatment) | - | 1 (6.7) | 14 (93.3) | - |
| Subjective sleep quality (placebo) | - | 1 (6.7) | 14 (93.3) | - |
| Sleep latency (treatment) | 2 (13.3) | 9 (60) | 3 (20) | 1 (6.7) |
| Sleep latency (placebo) | 1 (6.7) | 3 (20) | 7 (46.7) | 4 (26.7) |
| Sleep duration (treatment) | 8 (53.3) | 1 (6.7) | 2 (13.3) | 4 (26.7) |
| Sleep duration (placebo) | 3 (20) | 4 (26.7) | 1 (6.7) | 7 (46.7) |
| Sleep efficiency (treatment) | 8 (53.3) | 1 (6.7) | 2 (13.3) | 4 (26.7) |
| Sleep efficiency (placebo) | 3 (20) | 4 (26.7) | 1 (6.7) | 7 (46.7) |
| Use of sleep medication (treatment and placebo) | 10 (66.7) | 2 (13.3) | 2 (13.3) | 1 (6.7) |
| Sex | Age | History or Symptoms of Psychotic Disorders | Diagnosis of one of the Sleep Disorders | History or Symptoms of Convulsion | History of Usage of Hypnotic Drugs | History of Usage of ECT | Nationality | Drug Use | Antiretroviral Drugs |
|---|---|---|---|---|---|---|---|---|---|
| Male-woman | 18-50 | No | No | Yes | No | No | Lord, Kurd, Baloch Turk |
no | Efavirenz Rilpivirine Duravirin |
| Polysomnography (PSG) Test Indexes | Treatment | Placebo |
|---|---|---|
| Leg Movement Index | 0.980±0.2 | 0.1±0.3 |
| EMG | 0.980±0.3 | 0.9±0.4 |
| Respiratory Hypopneas | 1.120±0.2 | 0.8±0.1 |
| Snoring Index SI | 0.4±0.1 | 0.5±0.3 |
4.4. Polysomnography (PSG) Test Indexes
Table 5 explains some of the polysomnography (PSG) test indexes. Therefore, significant or descriptive mean differences were not observed among groups. Unfortunately, not all indicators were evaluated due to lack of facilities and lack of patient cooperation.
5. DISCUSSION
The term sleep disorder refers to a lack of sleep or poor quality of sleep. It is common for individuals with sleep disorders to be unable to experience restorative sleep, to have trouble falling asleep or staying asleep, or to wake up early in the morning [13]. There is a greater prevalence of sleep disorders and other sleep difficulties among participants than among the general population [14]. Sleep problems can indicate an increased risk of depression, pain, and substance abuse for people with HIV [15]. It has been reported previously that the prevalence of poor sleep quality among HIV-positive individuals ranged from 40% to 100% when it came to their quality of sleep. Additionally, HIV-related dementia may contribute to sleep difficulties in patients with advanced HIV disease (AIDS) [16].
The severity of disrupted sleep may not always be distinguishable from the overall quality of life of the patient by physicians [17]. Among HIV-positive patients, sleep is associated with quality of life on a complex and multidimensional scale, and this index may also influence the underlying symptoms of insomnia [18]. According to our findings, participants are mostly satisfied with medical treatments and health service instructions. For example, a recent study reported that access to medical services had a significant impact on HIV patients' sleep quality [19]. On the other hand, the least satisfied indexes of the quality of life questionnaire were enjoyment in life, level of appearance, money availability, and sleep. Studies have reported varying prevalence levels of sleep disorders among participants, which may be interpreted by the study location, the demographic characteristics of the participants, the inclusion and exclusion criteria, or the different data collection techniques used in the studies [20] (Table 4).
Neurofeedback is used in our study to assess changes in brain state and to fine-tune, strengthen, and enhance brain cell efficiency. As a result, first behavioral changes observed by patients following neurofeedback treatment typically include a change in sleep pattern and a change in sleep regulation. it was reported that neurofeedback training (12-14 Hz, SMR) on animals such as cats could change their sleep electroencephalogram (EEG) [21]. Evaluating neurofeedback protocols improved subjective sleep quali ty. Through neurofeedback, psychological state of the body as well as undesirable anxious thoughts throughout everyday life would be controlled. Moreover, it also treats certain disorders by improving CNS function.
CONCLUSION
To sum up our findings, a new understanding of the relationship between poor sleep quality and a profile of risk factors in HIV-infected individuals has been gained. The poor quality of sleep among these patients appears to be a common problem caused by a variety of factors. In order to improve the quality of sleep for this group of individuals, intervention is necessary. Aside from pharmacological treatment, other non-pharmacological interventions that may be effective in treating sleep disorders include sleep hygiene training, behavioral changes, and stress reduction techniques. Furthermore, with the purpose of enabling more effective prevention and treatment of sleep disturbances in participants, future research is required in order to determine the pathophysiology of poor sleep quality and other sleep disturbances.
LIST OF ABBREVIATIONS
| CNS | = Central Nervous System |
| DASS | = Depression Anxiety Stress Scales |
| PSQI | = Pittsburgh Sleep Quality Index |
| SI | = Snoring Index |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study has been approved by the Tehran University of Medical Sciences' ethics committee reviewed and approved the study protocol (ir.TUMS.VCR.REC.1398. 998).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
ACKNOWLEDGEMENTS
The authors would like to thank the staff of Imam Khomeini Hospital Complex, Tehran University of Medical Sciences, Tehran, Iran, for their contribution to this study and Bioline and Iran's National Elites Foundation (SN: 1345, Medinateb Co., Iran) and Dr.Amir Ali Ramezani (Department of Microbiology, Faculty of Biochemistry, Biophysics and Biotechnology, Jagiellonian University, Krakow, Poland) and Iran's National Elites Foundation.

