All published articles of this journal are available on ScienceDirect.

Short-term Effect of Training in Increasing Midwives’ Knowledge, Attitudes, and Practices Related to HIV and AIDS Prevention
Abstract
Introduction:
The study aims to analyse the effect of the training intervention program on midwives’ HIV-related knowledge, attitudes, and practices in Central Java. The training focused on HIV epidemiology, transmissions, co-infections, PITC, risk contacts, and prevention of mother-to-child transmission (PMTCT). It was designed to improve midwives’ knowledge, positive attitudes, and HIV/AIDS prevention practices, including reducing fear and stigma concerning people living with HIV/AIDS (PLWHA).
Material and Methods:
This study employed a Quasi-experimental pre-post-test design. The respondents are 50 village midwives equally divided into experimental and control groups. Data were collected using a questionnaire adapted from WHO, and it included questions about participant demographic characteristics, knowledge, attitudes, and practices on HIV and AIDS prevention programs. Furthermore, training consists of lecturing, group discussion, simulation, conversation with PLWHA, and watching a film about HIV including practicum.
Results:
There was a positive effect on midwife knowledge, attitudes, and practices in the early detection of HIV cases for pregnant women and reproductive age groups and HIV/AIDS prevention programs. The improvement in knowledge, attitudes, and practices occurred significantly in the intervention compared to the control. The adjustment intervention effects were beneficial and statistically significant (p-value <0.05), particularly the magnitude of the treatment effect for the knowledge score, which increased of 7.73% of the baseline mean knowledge. There was a significant association between knowledge and practices with a p-value of 0.002.
Conclusion:
Training midwives in HIV prevention was a beneficial program and positively impacted knowledge, attitudes, and practices. This study recommended the need for comprehensive training for village midwives, especially those related to their tasks in HIV prevention.
1. INTRODUCTION
The Human Immunodeficiency Virus (HIV) epidemic in Indonesia has been increasing three times higher compared with many other South East Asian countries. Recent data showed that the prevalence increases in housewives and children more than in critical populations. The higher incidence rate among mothers/housewives is because most husbands are
more likely to have sexual relations with commercial sex workers. Most mothers conducted HIV tests when their husbands died, and their children have been getting chronic diseases such as diarrhea, upper respiratory tract infection, and pneumonia [1, 2]
Based on WHO recommendations, in the absence of participation in mother-to-child transmission prevention programs (PMTCT), the percentage risk of HIV mothers transmitting the virus to their babies is around 15% to 45%. Therefore, early detection during pregnancy provides a gateway to preventing children from acquiring HIV from their mothers. HIV test is crucial for encouraging the mother to participate in the PMTCT program. However, voluntary counselling and tests (VCT) in many health services, as one of the efforts to encourage people, including mothers, to be aware of their status voluntarily, has not been utilized optimally. Even though the number of identified high-risk people has increased, fewer have participated in counselling and test. Provider-Initiated HIV (PITC) testing and counselling for pregnant mothers have been introduced and should be provided by health workers, including midwives, as a part of antenatal care (ANC) services. Therefore, midwives had to be educated in HIV prevention, reducing stigma and discrimination, including fear of spreading the disease [3, 4].
The Government of Indonesia launched a village midwife program in 1989 to place a skilled birth attendant in every village to respond to the high rate of maternal mortality [5]. Midwives are the primary sources of reliable health information and role models for potential and pregnant mothers since they provide many maternal and child health services, particularly for the villagers. Midwives have high-intensity interaction with mothers in the MCH clinic and at home compared to other health professions. Instead of providing services, the key role of midwives also includes health promotion related to sexual and reproductive health and HIV/AIDS. Therefore, midwives would play an important role as health educators and promotors to encourage the mother to do HIV tests. However, many midwives lack knowledge and attitudes toward sexuality and HIV/AIDS [6].
Demak Regency reported that the 2021 cumulative number of people HIV infected is about 638 or 0.03% of the total population, including pregnant mothers. In 2014, the data identified only 2 cases, increasing significantly from 2015 until now. Since Regency Health Office recommended that village midwives conduct the PITC approach as routine care of pregnant women in the ANC clinic, they should be educated and trained about HIV/AIDS, primarily PMTCT and PITC. There are 269 village midwives in Demak, and less than 20% have been informed about HIV/AIDS and PMTCT. Stigma and discrimination, including fear of contagion disease, are still high among midwives [7, 8].
Health providers, including midwives, need information about HIV/AIDS because they lack knowledge about transmission and prevention. One study reported that nearly half, or 42.4%, of health providers, discriminate against patients living with HIV/AIDS (PLWH) in their services, such as doing PLWH isolation and using personal protection equipment when providing services to PLWH. The negative attitudes of health providers include judgments about the moral worth of PLWH [9, 10] and rejection of providing a service because of fear of contagion [11].
A factor that causes the failure of HIV prevention efforts is the high stigma and discrimination against people living with HIV. Stigma makes people with HIV, and their families feel afraid and embarrassed to seek help related to the disease, even refusing to take precautions. Stigma occurs in society and health care [12], and some health workers prefer to be distant and not offer health care to HIV people. This includes Female Sex Workers, IDUs, and males who have sex with a man. Stigma by health workers occurs because of the anxiety of contracting HIV while treating patients. Based on research conducted in Iran, around 45% and 53% of health workers have poor and moderate attitudes toward people living with HIV. They fear being infected when caring for PLWH patients, making health workers inform their colleagues in writing. This information is conveyed to correctly use universal precautions in treating the patient [13, 14]. The results also show that health workers who treat HIV patients will be shunned by their socio-environment, including family, and colleagues [14]. A study in Indonesia also found that health workers were shunned by colleagues, family, and friends in the neighborhood for working with HIV patients. Another study found that health workers still fear HIV, thus, they avoid caring for the patients [10, 15]. In recent years, though there have been efforts to prevent HIV transmission from mother to child in Central Java Province, which is integrated into antenatal care services, HIV cases among pregnant mothers remain increasing. The previous study shows that midwives tend to refuse to serve pregnant mothers who were suspected of being infected by HIV [16]. They would instantly refer the suspected mother to a hospital due to fear of contracting the disease. Lack of Knowledge and misinformation on HIV causes including negative attitudes toward people living with HIV among midwives remain high [17]. This study was conducted to improve ANC services related to HIV and AIDS prevention including reducing stigma at the village level by enhancing village midwives’ knowledge, attitudes, and practices. Furthermore, it examines the short-term training effect of midwives’ knowledge, attitudes, and HIV and AIDS prevention procedures.
2. MATERIALS AND METHODS
The study employed a quasi-experimental design with a comparison group baseline and end-line measurements using non-random assigned intervention and control groups at Demak regency. There are 27 health centres throughout Demak regency, with a total number of village midwives were 269 persons [7]. On average, there are 10 village midwives for each health centres. Ten health centres were selected purposively with inclusion criteria: the highest incidence of HIV cases among pregnant mothers and children, and the highest number of high-risk men. The village midwives at selected health centres who never attended HIV training and were willing to participate were involved in this study. The participants' recruitment shows as follows:
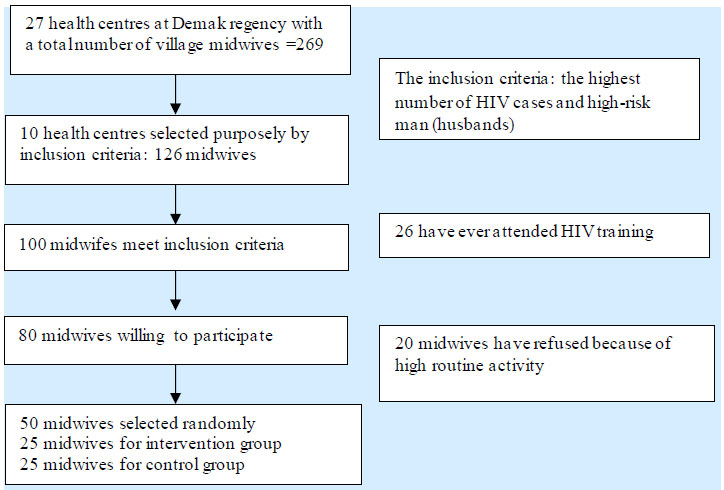
The sample size was calculated using the Lemeshow formula by assuming of a confidence interval of 95% and a power of 80%; [18-20] in addition to a minimum difference of two KAP before and after the intervention, resulting in a minimum sample of 22 each. Considering the possibility of dropping out during intervention, the researchers selected to invite of a total 50 midwives who met the inclusion criteria to participate in this study. The experimental and control groups were carefully selected to avoid the possibility of contact across the group and to prevent the risk of contamination. Then, five midwives were recruited randomly at each health centre to participate in this study.Therefore, the intervention and control groups consisted of 25 midwives, respectively.
The study was conducted from July 2019 until September 2019, and the participants signed an informed consent form before observation. The Ethical Review Board of the Faculty of Public Health at Diponegoro University, Semarang, Indonesia approved the study protocol with No. 195/EC/FKM/2019.
2.1. Intervention Procedures
Training intervention for midwives consisted of three days with ten sessions focused on basic information, including the HIV epidemic. Day first consists of lecturing and discussing HIV/AIDS awareness and attitudes, transmission and infection control, navigating the stigma, discrimination, psycho-social impact of HIV/AIDS, the roles of midwives and practices with mothers, addressing trauma, and social support issues related to ANC HIV testing. The following day is simulation and role-playing, including a discussion of cases and testimony from people living with HIV/AIDS, and day third is a practicum, fieldwork, and case analysis. During training, all participants were provided snacks and lunch. At the end of the 3-day training, they were provided the compensation of 3 days transportation and incentive fees including educational materials. Classes were held in District Health Office. Although the control group did not receive the HIV training intervention along with the intervention group, after completion of the study, the training was provided to the control group with a similar quantity and quality, including the same compensation.
A five-person team collected data, including health personnel and research. The instrument was a standardized, interviewed-administered questionnaire adapted from WHO. It consists of (1) Sociodemographic characteristics such as sex, age, duration of being a midwife, and experience in handling HIV/AIDS patients. (2) Knowledge regarding HIV/AIDS as assessed by 25 close-ended questions. The question is such as “ PITC refers to HIV testing and counselling which is recommended by health providers to persons who has HIV risk behaviour “, answer: yes (1) or no (0), (3) attitudes towards HIV/AIDS prevention including universal precautions used and stigma by 10 questions. For example “During ANC services, a midwife has to ask the pregnant mother to do HIV testing” answer: strongly agree (2), agree (1) and neutral (0), disagree (0). (4) midwives’ practices to prevent HIV/AIDS are assessed by 15 questions. The question example is: “I always do HIV counselling for pregnant women during ANC services”. For each knowledge question, the score is one point for the correct answer and zero for the incorrect one, and the possible score ranges from 0-25. Each attitude statement was scored from 2 for the most positive attitude to zero for the most negative and the possible score range 0-20. Respondents selected one choice ranging from strongly agree and disagree. For practice questions, one point is awarded for the practice and none for the not practice and the possible score ranges 0-15.
The questionnaire was validated with pilot testing to check the validity and reliability of 30 midwives in six other health centres in the Demak district. The pilot testing result was good reliability with a Cronbach alpha of more than 0.82. Furthermore, sociodemographic characteristics variables of both groups were administered before intervention and compared between the two groups to identify confounding variables. Variables of knowledge, attitudes, and practices related to HIV/AIDS prevention were administered at baseline and after the intervention.
2.2. Statistical Analysis
Univariate analysis was employed to describe means, median, frequencies, percentages, and standard deviations for sociodemographic data, knowledge regarding HIV/AIDS, attitudes, and practices related to HIV prevention, including universal precautions. The difference scores in baseline data between the independent variables of the intervention and control group were tested by Chi-squares for dichotomous and independent t-tests for continuous variables. At each follow-up/end-line time, the magnitude of the intervention effect is counted through the difference between the intervention and control groups in the mean score change. This is shown in the formula below:
The intervention effect = (Post-test–Pre-test) intervention – (Post-test–Pre-test) control groups
Linear mixed models were employed to quantify and test the statistical significance of intervention effects on knowledge and attitude scores at post-test and follow-up time. Unadjusted and adjusted fixed effects models in follow-up and intervention times were tested. Each model included the repeated measure, the respondent as an individual subject, with an unstructured covariance type. The variables’ characteristics, including experience in caring for PLWHA, counselling, referring to hospital, home visits, and educating HIV pregnant women show homogenous between intervention and control groups before intervention. Therefore, no covariate variable should be adjusted to a fixed effects model. In addition, the association between practice scores as a dependent variable, and knowledge, and attitudes as independent variables was also tested by simple linear regression. SPSS v21 was employed for running statistical analyses.
3. RESULTS
In the intervention and control groups, the independent variables’ knowledge, attitudes, and practices related to HIV/AIDS prevention were measured before, one month after, and two months after. Categorical and Continuous independent variables are summarized and compared between the intervention and control groups before intervention (Tables 1 and 2, respectively).
| Characteristics | Intervention Group (n = 25), | Control Group (n = 25), | p-value | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Age (Y) | 35.6 | 5.976 | 35.20 | 5.259 | 0.401 |
| Length of working (Y) | 13.56 | 6.427 | 13.12 | 6.294 | 0.403 |
| Characteristics | Intervention Group (n = 25),n (%) | Control Group (n = 25), n (%) | p-value | |
|---|---|---|---|---|
| Education | ||||
| 3-years Diploma | 14 (56) | 17 (68) | 0.185 | |
| 4-years Diploma | 9 (36) | 8 (32) | ||
| Master graduates | 2 (8) | 0 (0) | ||
| Experience in PLWHA care | ||||
| Have experience | 12 (48) | 17 (68) | 0.137 | |
| Have no experience yet | 13 (52) | 8 (32) | ||
| HIV Early detection of pregnant women | ||||
| Have experience | 12 (48) | 19 (76) | 0.061 | |
| Have no experience yet | 13 (52) | 6 (24) | ||
| Counselling for unwanted pregnancy to adolescents | ||||
| Have experience | 22 (88) | 15 (60) | 0.029 | |
| Have no experience yet | 3 (12) | 10 (40) | ||
| Referring pregnant women at HIV risk to hospital | ||||
| Have experience | 5 (20) | 6 (24) | 0.299 | |
| Have no experience yet | 20 (80) | 19 (76) | ||
| Home visit to HIV patient | ||||
| Have experience | 5 (20) | 6 (24) | 0.299 | |
| Have no experience yet | 20 (80) | 19 (76) | ||
| Mentoring HIV patients as case managers | ||||
| Have experience | 1 (4) | 6 (24) | 0.137 | |
| Have no experience yet | 24 (96) | 19 (76) | ||
| HIV education for pregnant women | ||||
| Have experience | 22 (88) | 18 (72) | 0.106 | |
| Have no experience yet | 3 (12) | 7 (28) | ||
The Chi-Square Test showed that the education of respondents and the prevalence of variables related to experience with HIV care, early detection, referring HIV patients, home visits, and education were homogenous between the two groups, except the experience in counselling for unwanted pregnancy of adolescents was statistically significantly higher in the intervention group than the control group with p-value 0.029 (Table 3). Thus, the intervention effect on knowledge, attitudes, and practices was adjusted for this variable. No other baseline data significantly differed between the groups. Questions related to knowledge, attitude, and practices were measured before, one month after (follow-up 1), and 2 months after the intervention (follow-up 2).
| Variables | Intervention Group (n = 25), Mean (SD) |
Control Group (n = 25), Mean (SD) |
p-value |
|---|---|---|---|
| Pre-test | |||
| Knowledge | 18.20 (2.141) | 18.56 (1.356) | 0.759 |
| Attitudes | 9.88 (0.332) | 9.48 (0.714) | 0.007 |
| practices | 7.56 (2.599) | 7.96 (4.363) | 0.652 |
The statistical result using the independent T-Test showed that the prevalence of variable age of respondents and length of work between the intervention and control group have no differences. The average age of midwives is around 35 years old, and the length of employment is 13 years, meaning most respondents have worked relatively for a long time.
3.1. Differences between Intervention and Control Groups Related to Knowledge, Attitudes, and Practices of PITC before the Intervention
The intervention program was conducted within three days using a classroom setting. Based on the theory of Social Cognitive, the knowledge and attitudes of respondents who receive training will improve by 50% [21]. Descriptive statistics describe the mean, frequency, percentage, and standard deviation for sociodemographic characteristics of respondents, knowledge, attitudes, and practices related to HIV/AIDS prevention.
There is no difference between knowledge and practice scores in the prevention for the control and intervention groups. The respondents have not received HIV/AIDS prevention training for both groups. However, the attitudes mean score was significantly different between the two groups, with a p-value of 0.007. Most respondents have a positive attitude toward HIV prevention. For knowledge, the average score of the intervention and control groups is 18.20 and 18.56, with a p-value of 0.759. The practice mean score for the control and intervention groups is slightly higher at 7.96 and 7.56 with a p-value of 0.652
Post-test 1 measurement was given shortly after one month of the intervention, and the respondents’ knowledge had increased from 18.20 to 20.44. There was a significantly increased knowledge of the intervention group by 2.24 points. Meanwhile, the practice variable in the intervention group increased significantly from 7.56 to 8.04, and the p-value was 0.035. In attitude variables, there is no difference between the intervention and the control groups because the attitude change needs to take longer than the knowledge. The attitudes score slightly increase from pre-test to post-test 1 and post-test 2 with the mean scores were 9.88, 9.89, and 9.95 respectively.
The measurement results of 2 months after the intervention showed increased respondents’ knowledge, especially related to counselling communications to HIV patients. The intervention group’s knowledge, attitude, and practice variables also increase. In the second post-test, there is a difference between the knowledge and attitude of the intervention and control groups. However, the practice between the control and intervention groups has shown a significant difference. Even though the groups had statistically different practice scores, the increase was lesser than the knowledge score. After two months of intervention, some practices can be accomplished while on the field.
3.2. Effect of Treatment on Knowledge and Attitudes toward HIV on Village Midwives in Demak District
Unadjusted intervention effects at post-tests 1 and 2 are shown in Table 4. The intervention was associated with a statistically significant increase in knowledge score with a p-value < 0.05 for both follow-up times. From the baseline to post-test 1, knowledge scores increased by 1.5 points more in the intervention group than in the control group. It represented an intervention-related increase of 7.79% of the baseline mean knowledge score. The absolute intervention effect on the attitude score was smaller than the knowledge score, although the improvement was very small and statistically insignificant. Since the training is only three days, it needs more time to boost motivation to change the midwife’s attitudes toward preventing HIV/AIDS. For the practice score, the absolute intervention effects were larger than the attitude scores, but the proportional increase in the former was smaller. The intervention-related benefit for all dependent variable scores was similar at both follow-up times.
| Score | Overall mean at baseline (Grand mean) |
Intervention effects (unadjusted), Follow-up I |
Intervention effects (unadjusted), Follow-up II |
||||
|---|---|---|---|---|---|---|---|
| Absolute magnitude (95% CI) | p-value | As % of baseline mean | Absolute magnitude (95% CI) | p-value | As % of baseline mean | ||
| Knowledge | 19,253 | 1.500 (0.801-2.199) | 0.001 | 7.79 | 1.120 (0.421-1.819) |
0,002 | 5.91 |
| Attitude | 9,673 | 0.100 (0,096-2.296) | 0.865 | 2.06 | 0.040 (-0.273-0.193) | 0.734 | 4.13 |
| Practice | 8.080 | 0.720 (-0.684-2.124) | 0.313 | 8.91 | 0.240 (-1.164-1.164) | 0.736 | 2.97 |
| Grand mean Score | Overall mean at baseline (Grand mean) |
Intervention effects (adjusted), Follow-up I |
Intervention effects (adjusted), Follow-up II |
||||
|---|---|---|---|---|---|---|---|
| Absolute magnitude (95% CI) | p-value | As % of baseline mean | Absolute magnitude (95% CI) | p-value | As % of baseline mean | ||
| Knowledge | 19.253 | 1.142 (0,310-1,975) | 0.003 | 5.931 | 1.489 (0,656-2,321) | 0.000 | 7.733 |
| Practice | 8.080 | 0.240 (-1,481-1,961) | 1,000 | 2,970 | 0.720(-1,001-1,441) | 0,938 | 8.910 |
| Variable | B | 95% CI | β | t | P value |
|---|---|---|---|---|---|
| Constant | -16.288 | -30.509—2.067 | -2.369 | 0.027 | |
| Knowledge | 1.190 | 0.496-1880 | 0.595 | 3.546 | 0.002 |
| Constant | 19.800 | -7.878-47.478 | 1.480 | 0.152 | |
| Attitude | -1.200 | -4.022-1.622 | -0.180 | -0.880 | 0.388 |
The absence of differing characteristics between the groups did not adjust for all independent variables, except the experience in counselling of adolescents variable. The attitudes score as one of the dependent variables was also a significant difference between the groups at baseline. Therefore, an adjustment model was made without involving these variables to show the magnitude of the treatment effect. Adjustment means knowledge and practice scores at three measurements shown in Table 5. The adjustment intervention effects were beneficial and statistically significant (p-value <0.05) only for the knowledge score increase of 7.73% of the baseline mean knowledge. It is probably the effect of intervention needs more time to modify attitudes and practices.
The findings indicate that knowledge was associated with midwife practices in HIV prevention with a p-value of 0.002. It suggests that the higher score of knowledge was willing to practice more in HIV prevention. If the knowledge increases by one point, the average practice increases by 1.190 points. However, the attitudes were not associated with midwife practices with a p-value is 0.388. In this case, the attitudes variable does not contribute to explaining the midwife practices in HIV prevention (Table 6 ).
4. DISCUSSION
This quasi-experimental study was undertaken to measure and assess the effects of training to improve village midwives’ knowledge, attitudes, and practices in HIV/AIDS prevention activities in Demak District, Central Java, Indonesia. The treatments were substantially and significantly related to increasing midwives’ knowledge, attitudes, and practices. Based on the results, the expected intervention target is to reduce the incidence of HIV transmission in infants infected through their mothers during pregnancy and delivery in the Demak District. This study is expected to reduce stigma among HIV-AIDS patients and increase village midwives’ knowledge, attitudes, and practices in HIV prevention.
The intervention combines several components, including training conducted during the three days that include integration practices ANC-PMTCT, demonstration as a way of counselling, and effective communication for pregnant women to examine and prevent HIV. The intervention is targeted to reduce the incidence of HIV in infants whose mothers infect during pregnancy and childbirth. An unsupported understanding of pregnant women with the ability of the village midwife to be the primary helper in counselling and testing can lead to a higher HIV incidence in the infant age group. The midwife’s strategic position in carrying out this integration is considered a good foundation and prefix. Early detection of HIV can be unforgettable when midwives perform health checks on pregnant women. The risk of midwives contracting HIV during childbirth is also high [22]. Therefore, training to improve understanding, awareness, and positive attitudes toward early detection is beneficial. Recognizing the risk of childbearing-age and pregnant women infected with HIV is also needed. A study mentions that intervention in the form of standardized knowledge sharing and contact with people living with HIV for 50 minutes with health workers in Hong Kong can reduce the stigma among health workers [23]. The provision of HIV education, testing, and messages such as brochures, bulletins, and testimony can reduce stigma [6, 24, 25].
The midwives are recognized as responsible and accountable professionals working in partnership with women to provide the necessary support, care, and advice during pregnancy, childbirth, and the postpartum period. The mother-to-child HIV early detection factors are a pregnant mother’s readiness for HIV testing, husband support, information access, and support from midwives or other health workers [26]. In this regard, health personnel needs support in the form of early HIV detection, PMTCT services, and stigma reduction in PLWHA [27]. For midwives to provide good services to PLWHA, they are required to have complete knowledge. Following the needs of pregnant women regarding HIV / AIDS, knowledge and attitude interventions should be provided to implement knowledge and attitudes in their PMTCT activities [27, 28].
It should be noted that the most important of limitation of this study is the small sample size which is just a fraction of village midwives throughout Demak regency which has reduced the generalizability of the findings. Besides that, the three-day short-term training was probably not sufficient for changing the midwives' knowledge, attitudes and practices in preventing HIV/AIDS. Another limitation of this study includes the lack of a control group with another intervention not related to HIV prevention programs to examine the effect of the training program used in the intervention group.
5. CONCLUSION
Training midwives in HIV prevention was a beneficial program and positively impacted knowledge, attitudes, and practices in the early detection of HIV cases for pregnant women and reproductive age groups and HIV prevention programs. Differences in knowledge, attitudes, and practices occurred significantly in the group interventions compared with the control. Increased practice scores in the intervention group occurred from pre-test-post-test 1 - post-test 2, unlike in control group. The adjustment model shows that the magnitude of the treatment effect only for the knowledge score increase of 7.79% of the baseline mean knowledge. This study suggests the need for more comprehensive training for village midwives and applying the training results to their routine activities especially those related to early HIV detection in women risk groups and pregnant women.
LIST OF ABBREVIATION
| HIV | = Human Immunodeficiency Virus |
| PMTCT | = Participation in Mother-to-child Transmission Prevention Programs |
| VCT | = Voluntary Counselling and Tests |
| ANC | = Antenatal Care |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The Ethical Review Board of the Faculty of Public Health at Diponegoro University, Semarang, Indonesia approved the study protocol with No. 195/EC/FKM/2019.
HUMAN AND ANIMAL RIGHTS
No animals were used for studies that are the basis of this research. All the humans were used in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013 (http://ethics.iit.edu/ecodes/node/3931).
CONSENT FOR PUBLICATION
The participants signed an informed consent form before observation.
AVAILABILITY OF DATA AND MATERIALS
the data that support the findings of this study are available from the corresponding author [S.Z] on special request.
FUNDING
This study was funded by Faculty of Public Health, Diponegoro University.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
ACKNOWLEDGMENTS
The authors are grateful to the health officers at Demak District Health Office, Central Java Province, for their permission and help in conducting the research. Furthermore, the authors of the Faculty of Public Health at Diponegoro University for permitting this study. Special thanks to all midwives for their kind support and participation.

