All published articles of this journal are available on ScienceDirect.

Knowledge of Students regarding HIV/AIDS at a Rural University in South Africa
Authors Info & Affiliations
Abstract
Introduction:
Knowledge about HIV/AIDS is essential for facilitating safer sexual behaviour hence, it is important in controlling HIV. Therefore, in the absence of a cure for the pandemic, adequate knowledge about the virus remains the backbone of prevention efforts.
Objective:
To assess the knowledge regarding HIV/AIDS among undergraduate students at a rural university in Limpopo Province, South Africa.
Methods:
A cross-sectional descriptive quantitative survey-based study was conducted at a rural-based university in South Africa. Stratified random sampling was used to select 345 students. A self-administered questionnaire composed of 26 questions was utilised to gather data and the data were analysed using SPSS version 26. Multiple logistic regression and chi-square tests [χ2] were employed to determine the association between HIV/AIDS knowledge and demographic variables.
Results:
The overall HIV/AIDS knowledge score of students shows that (74)21% had a poor level of knowledge, (126)37% had average knowledge, and (145)42% had adequate knowledge. There was no significant difference between male and female students regarding their knowledge about HIV/AIDS. Factors, such as age, level of study, the field of study, and religion, were not significantly associated with HIV/AIDS knowledge. However, the race was significantly associated with knowledge with coloureds and mixed races, almost six times less knowledgeable than blacks.
Conclusion:
In conclusion, students had inadequate knowledge about HIV/AIDS. Misconceptions about HIV/AIDS facts, transmission routes, and prevention aspects were also prevalent among students. The present study accentuates the need for providing students with more HIV/AIDS education to fill HIV knowledge gaps and misconceptions.
1. INTRODUCTION
Despite concerted global efforts to combat Human Immunodeficiency Virus (HIV), increasing new infections and risky sexual behaviours is a pressing global public health problem [1]. It is estimated that AIDS has killed about 35 million people since it emerged in the eighties [2]. Most people living with HIV/AIDS are found in Sub-Saharan African countries, which accounts for more than two-thirds of the people living with HIV worldwide [1]. Despite HIV infecting people of all ages, young people aged 15–24 years account for approximately 50% of all new HIV infections [3]. Furthermore, most of these young people reside in the East and Southern Africa region compared to other regions on the continent [2]. Out of 4.2 million young people diagnosed with HIV, most are young women [3]. The young women in the Sub Saharan region account for 26% of new HIV infections [2]. Furthermore, globally, about a million curable cases of sexually transmitted infection are contracted each day [4].
Worldwide, South Africa is the most affected country, with an estimated 7.2 million people living with HIV/AIDS [1]. Furthermore, in South Africa, about 7% of young people aged 15 - 24 were diagnosed with HIV [5]. Also, the youth are the least covered by the antiretroviral treatment program, i.e., 14.3% [6]. The high rates of sexually transmitted diseases among youth can be ascribed to young people engaging in high-risk sexual behaviours due to peer pressure and immaturity to handle sexual pressure [5]. Studies on youth sexual behaviours in South Africa show that young people continue to face the greatest risk of HIV infection [7]. Furthermore, other surveys reported that South African youth (15-24 years) exhibit unsafe sexual behavioural practices. These include a high average number of partners, sex with unknown persons, inconsistent use of condoms, negative views about condom use, and abuse of various substances [8]. Other studies conducted in South Africa show that unplanned pregnancies are prevalent among youth aged 15-24 [7, 9]. This is the age group in which Higher Education Institutions (HEIs) particularly deal with students' admission into post-school education.
Universities are considered high-risk areas that fuel the spread of HIV infection because students engage in risky sexual behaviours [10]. University students engage in high-risk sexual behaviours, such as early sexual debut, multiple sexual partners, having older sexual partners, substance abuse before sex, and unprotected sex, making them vulnerable to HIV infection [11]. This is exacerbated by the fact that university students underestimate the risk or severity of HIV/AIDS; they are immature to handle sexual pressures, have misconceptions about the virus and easily succumb to peer pressure [12].
In light of the threat posed by HIV/AIDS, it is imperative to improve youths understanding and awareness around these issues globally [13, 14]. Due to the absence of a vaccine or cure for AIDS, knowledge regarding HIV/AIDS remains the critical enabler for changing risky sexual behaviours [15]. HIV/AIDS education is one of the proven strategies for combating HIV/AIDS [16]. According to knowledge, attitude and behaviour theory, being aware of the disease is the first stage in the behaviour change process [17]. Previous research suggests that having the correct knowledge about HIV reduces new infections in countries most affected by the disease [3]. Therefore, engaging young people through education is key to protecting their health and addressing the HIV epidemic [12]. Considering that young people are the future of tomorrow, it is important to grasp young people's knowledge about HIV/AIDS-related issues because, at the moment, it can be prevented through protective behaviours and behaviour change [18].
While specific HIV/AIDS knowledge has been explored extensively in university students, several studies have consistently found relatively high HIV knowledge scores among the student population [19, 20]. However, other studies found that there are still knowledge gaps [21, 22]. Most of the published studies on HIV/AIDS were conducted in South African urban-based universities rather than underserved rural areas [22-27]. In general, South African university students are knowledgeable about HIV infection [22-27]. To our knowledge, there no such information was provided to the students in a rural-based university in South Africa.
The Limpopo Province is generally referred to as a rural province and has two universities that are classified as rural-based and historically disadvantaged, namely the University of Venda (UNIVEN) and the University of Limpopo (UL) [23]. Fiscal challenges characterise historically disadvantaged universities due to budgetary cuts, which have dire implications for managing HIV/AIDS prevention programmes [24-27]. Based on studies conducted at the university where this study was conducted, there are inadequate HIV/AIDS prevention and mitigation programmes for students and staff [26, 27]. Besides, there is limited commitment to support these programmes from the universities [27-30]. Therefore, most students who are not targeted by these programmes have knowledge gaps regarding HIV/AIDS. As a rural province, Limpopo has one of the growing HIV prevalence rates in the country [23]. In South Africa, rural populations face many challenges that put the youth of university-going age at risk of acquiring HIV infection, such as poor health services, unemployment, poverty, illiteracy, and inadequate health reproductive information compared to young urbanites [28, 29]. Also, the rate of HIV in rural Limpopo is a growing public health concern over the past decade. Tuberculosis and AIDS remain the leading cause of death [23]. Preventing new HIV infections among university cohort people remains one of the province's strategies to tackle the pandemic.
Considering the high HIV infection rates among youth and the need to meet the 90-90-90 goals, South Africa, through the Department of Higher Education and Training, initiated university-based HIV/AIDS mitigation and prevention programmes to reduce new infections among the students [30]. University students are vital members of society and every nation's future [31]. Reducing the number of university students who contract HIV is one of South Africa's government strategies to defeat the pandemic [32]. Furthermore, based on Sustainable Development Goals (SDG 3), it is paramount to empower individuals with HIV/AIDS knowledge to defeat the pandemic [33]. There is a pressing need to assess the level of knowledge regarding HIV/AIDS among students at a rural university to serve as a baseline for developing appropriate HIV/AIDS education programmes that affect behaviour change. To our knowledge, no studies have assessed the knowledge of HIV/AIDS among students at a rural-based university in South Africa. Most studies have focussed on knowledge of the general population. In most African countries, there are some Urban-Rural inequities in terms of access to services and information dissemination [34, 35]. Therefore, this study sought to explore students' knowledge regarding HIV and AIDS at a rural university in South Africa.
2. METHODS
2.1. Study Design
This cross-sectional survey-based study was conducted to assess the knowledge of HIV/AIDS among students at a rural-based university in South Africa. The design enabled the researcher to make inferences about possible relationships between variables and socio-demographic characteristics [36]. The goal was to obtain information that is a snapshot of a population at a certain time, allowing conclusions to be drawn across a wide population [37]. The design was considered appropriate because it was cost-effective and less time-consuming; also, there was no need to follow up on the respondents. The limited budget was able to cater to all the costs associated with this study.
2.2. Study Area
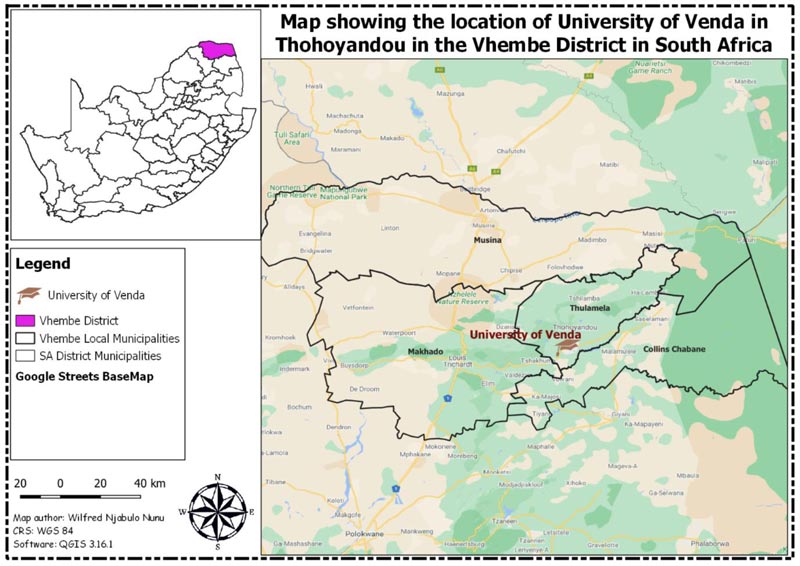
The study was conducted at a rural-based university located in Limpopo province in South Africa. University of Venda (UNIVEN) is one of the 24 state-owned public universities in South Africa. It is mainly a residential university with one main campus located in Thohoyandou town and has eight schools that incorporate 61 academic departments. The eight schools include Agriculture Sciences, Education, Environmental Sciences, Health Sciences, Human & Social sciences, Law, Management Sciences, and Mathematical & Natural Sciences. It has about 15,500 students, inclusive of postgraduates and undergraduates. Furthermore, it has a staff capacity of 800 comprising teaching staff, administrative staff, and support staff [38]. Some students at the institution engage in risky sexual behaviours, such as drug abuse, and unprotected sex, putting them at risk of HIV infection; also, many students are involved in the termination of pregnancies. Due to these reasons, more students are testing positive for HIV. Hence, this study at UNIVEN provides the opportunity to assess students' knowledge about HIV/AIDS at a university in a rural setting. This study's findings may assist university management in designing public health measures that improve student HIV knowledge, which translates into safer sexual practices. The map showing the study area is presented in Fig. (1).
2.3. Study Population
The study targeted senior undergraduate students. Senior students refer to those in their third and fourth years of study during the 2018 academic year. This target population was seen as appropriate because they had been studying in the institution for a longer time and would have undergone all the training curriculum stages and would give a comprehensive assessment. Therefore, their responses were bound to be more comprehensive regarding the study research questions. There were 4702 students registered in the academic year of 2018. This study was part of a large doctorate study that focused on developing a framework to integrate HIV/AIDS [39] content into curricula; hence it targeted third- and fourth-year students who were assumed to have prior learning experience regarding HIV/AIDS education. Furthermore, this student cohort was selected because the study sought to compare HIV/AIDS knowledge and respective socio-demographics, such as scientific areas of study and different years of study. It should be noted that different programs offer varied curriculums and are spread in a different number of years for one to complete in specific fields. Therefore, there was a need to have an inclusive population to draw out results that are generalisable to the whole university.
2.4. Sample Size and Sampling Procedure
The formula suggested by Slovin [40] was used to calculate the sample size, which is as follows:
whereas:
n = sample size
N = total population
e = margin of error (which is 0.05 or 5%)
In this case, N = 4702, which denotes university students from 8 schools at Univen and the level of precision [e] is +/- 0.05 of the true value from this study. The calculated sample size was 369.
= 4702/ 1 +(4702*0.05x0.05)
= 4702/1+ (4702*0.0025)
= 4702/1+ 11.755
= 4702/12.755
n = 369
In anticipation of the non-response rate, the researcher increased the sample size by 20%, from 369 to 443. Proportional allocation based on the selected schools' population was used to decide the required sample size for each school. Therefore, this involved stratification of students according to schools and a consistent proportion was selected from each school to make up the minimum sample size required for this study. The students were then selected from each school using stratified random sampling from a list of students until the sample size of 443 was achieved. If a student is selected and refuses to participate in the study, the next available student, who met the criteria was approached until the minimum sample size required was obtained.
2.5. Data Collection
The data was collected using a validated structured questionnaire adapted from previous studies [41, 42]. The authors chose these instruments because they were used to assess HIV/AIDS knowledge among university students. They were publicly available survey questionnaires in the context of this study. The questionnaire was developed in English, as this is the language of instruction at this rural university. The researchers in this study modified the original questionnaire's Likert scale to yes and no responses to suit how English is understood in this part of the world. The questionnaire was composed of three sections, socio-demographics, basic HIV/AIDS knowledge, and HIV transmission, and HIV prevention knowledge, totalling to 26 items using yes or no responses. The reliability and validation of the questionnaire were checked by conducting a pre-test before the actual data collection. The necessary minor adjustments to the questionnaire were made based on pre-test feedback. The data collected from the pre-test was only used to refine the data collection tools, and it was not part of the data that was finally analysed for this research. Furthermore, the participants in the pre-testing stage were not called back for the actual study.
Knowledge about HIV/AIDS was graded using Bloom's cut-off point scoring system [43]. The original Bloom's cut-off points, “low ≤ 50%,” “average: 51% and 74%”, and “high ≥ 75%,” were adapted and modified from HIV/AIDS knowledge questionnaire used on Malaysian university students [44]. Therefore, 1 score for a correct answer and 0 for incorrect answers were assigned. The score range was between 0 and 26. The overall score of HIV/AIDS knowledge was defined as follows: poor knowledge was in the range of 0-13 (0-50%), average knowledge was in the range of 14-19 (51-74%), and knowledgeable was categorised as 20+ (75%). The researcher and the research assistants distributed the questionnaires during school hours. Before administering the questionnaire, the purpose of the study and objectives were explained to the participants. Appointments were made with the respondents at least one week before data collection. Written consent was obtained first among all survey participants before administrating the questionnaire. All students were contacted at regular lectures, and the questionnaire was distributed and collected on the same occasion. In order to obtain the required minimum sample size, the questionnaires were distributed in various places, i.e., faculties' squares, libraries, cafeterias, and corridors.
2.6. Data Analysis
Data were checked for completeness and accuracy before being coded using entered Microsoft Excel 2016. The cleaned data were analysed using the Statistical Package for the Social Sciences (SPSS) version 26. Descriptive statistics, such as frequencies, percentages, tables, and graphs, were utilised to describe the questionnaire's demographic and knowledge items. Inferential statistics were performed to determine the relationship between variables of interest with the outcome variable “knowledgeable.” Firstly a Chi-squared test was conducted to determine whether or not variables, such as age, gender, race, level of study, the field of study, and religion were significantly associated with the level of knowledge. The chi-squared p-value of less than 0.05 denoted that these variables influenced the level of knowledge. Furthermore, Multiple Logistic Regression (MLR) was performed to compute odds ratios used to determine the strength of association and the confidence intervals generated. A p-value of less than 0.05 was considered significant.Only fully completed questionnaires qualified to be included for analysis to get comprehensive results.
3. RESULTS
3.1. Socio-demographic Characteristics of the Study Respondents
Six items assessed the demographics of the sample. A total of 443 questionnaires were distributed, and 345 questionnaires were returned, yielding a response rate of 77%. The results indicated that most of the respondents were in the age group of 20-29 (288/83.5%), male (227/65.8%), were of African descent (307/89%), were in the fourth year (183/53%), from School of Law (53/15.4%) and Christianity (339/98.3%) was the most dominant religion among these respondents Table 1.
| Variables | Category | Number of Respondents | Percentage of Respondents |
|---|---|---|---|
| Age (Years) | 20-29 | 288 | 83.5 |
| 30-39 | 35 | 10.1 | |
| 40-49 | 22 | 6.4 | |
| 50-59 | 0 | 0.0 | |
| 60-69 | 0 | 0.0 | |
| Gender | |||
| Male | 227 | 65.8 | |
| Female | 118 | 34.2 | |
| Race | Black | 307 | 89 |
| Coloureds | 38 | 11 | |
| White | 0 | 0.0 | |
| Level of Study | |||
| Third-year | 162 | 47 | |
| Fourth year | 183 | 53 | |
| School | |||
| Agriculture | 30 | 8.7 | |
| Education | 43 | 12.5 | |
| Environmental Sciences | 45 | 13 | |
| Health Sciences | 49 | 14.2 | |
| Human and Social Sciences | 42 | 12.2 | |
| Law | 53 | 15.4 | |
| Mathematical and Natural Science | 33 | 9.6 | |
| Management | 50 | 14.5 | |
| Religion | |||
| Christianity | 339 | 98.3 | |
| Traditional | 5 | 1.4 | |
| Islamic | 0 | 0.0 | |
| Hinduism | 1 | 0.3 |
3.2. General HIV/AIDS Knowledge
Table 2 shows the frequency of the distribution of HIV/AIDS knowledge. The majority of the respondents (273/79.1%) knew that HIV causes AIDS, and almost 95.6% (330) knew that condoms must be used to prevent HIV infection. About 80.3% (277) of the students were aware that a healthy-looking person could also be infected with HIV, and (289) 83.8% knew that using drugs before sex increases the risk of getting HIV. However, knowledge gaps were noted on nine items as only slightly above half [203/58.8%] answered that HIV and AIDS are the same things, and only 35.9% (124) correctly answered the question that “eating healthy foods can keep a person from getting HIV” and 52.2% (180) answered that antiretroviral drugs could cure HIV infection. Some respondents also had a misconception about the following items: 49% (169) responded incorrectly to the question that probed whether or not “AIDS is an infectious disease caused by bacteria.” These findings are presented in Table 2.
Table 2.
| - | - | Correct Response | Incorrect Response | ||
|---|---|---|---|---|---|
| Correct Answer to the Statement | N | % | N | % | |
| Statement regarding General knowledge about HIV/AIDS | |||||
| HIV/AIDS is the same thing | No | 203 | 58.8 | 142 | 41.2 |
| There is a cure for AIDS. | No | 238 | 69 | 107 | 31 |
| AIDS is caused by HIV | Yes | 273 | 79.1 | 72 | 20.9 |
| A person can get HIV by sharing a glass of water with someone who has HIV. | No | 164 | 47.5 | 181 | 52.5 |
| To prevent HIV infection, a condom must be used for every round of sex. | Yes | 330 | 95.7 | 15 | 4.3 |
| It is possible to get HIV when a person gets a tattoo. | Yes | 276 | 80 | 69 | 20 |
| Eating healthy foods can keep a person from getting HIV. | No | 124 | 35.9 | 221 | 64.1 |
| All pregnant women infected with HIV will have babies born with AIDS. | No | 160 | 46.4 | 185 | 53.6 |
| One can reduce the risk of HIV by having fewer sexual partners. | Yes | 261 | 75.7 | 84 | 24.3 |
| Antiretroviral drugs can cure HIV infection. | No | 180 | 52.2 | 165 | 47.8 |
| A healthy-looking person can also be infected with HIV. | Yes | 277 | 80.3 | 68 | 19.7 |
| AIDS is an infectious disease caused by bacteria. | No | 169 | 49 | 176 | 51 |
| Using alcohol or drugs before or during sex can increase a person's risk of getting HIV. | Yes | 289 | 83.8 | 56 | 16.2 |
| Statements regarding how HIV/AIDS is transmitted | |||||
| Sexual intercourse | Yes | 305 | 88.4 | 40 | 11.6 |
| Using a dirty toilet seat | No | 172 | 49.9 | 173 | 50.1 |
| Sharing a needle to inject drugs with someone who is HIV positive. | Yes | 329 | 95.4 | 16 | 4.6 |
| Hugging someone with AIDS | No | 200 | 58 | 145 | 42 |
| Having vaginal sex without a condom | Yes | 320 | 92.8 | 25 | 7.2 |
| Getting bitten by a mosquito that is carrying a virus | No | 126 | 36.5 | 219 | 63.5 |
| Having anal sex without using a condom | Yes | 289 | 83.8 | 56 | 16.2 |
| Statements regarding prevention measures | |||||
| Proper condom use | Yes | 257 | 74.5 | 88 | 25.5 |
| Screening blood before transfusions | Yes | 309 | 89.6 | 36 | 10.4 |
| Get tested and know your partner's HIV status | Yes | 300 | 87 | 45 | 13 |
| Limit Sexual Partners | Yes | 329 | 95.4 | 16 | 4.6 |
| Taking Pre-exposure Prophylaxis medication | Yes | 286 | 82.9 | 59 | 17.1 |
| Taking Post-exposure prophylaxis medication | Yes | 320 | 92.8 | 25 | 7.2 |
3.3. HIV Transmission Knowledge
Knowledge of HIV transmission was also assessed using seven questions with yes and no responses. The majority of the students knew that HIV is transmitted through sexual intercourse (305/88.4%), by sharing infected needles (329/95.4%), having vaginal sex without a condom (320/92.8%), and anal sex without a condom 289 (83.9%). However, knowledge gaps were noted on two items only; 49.9% (172) answered that HIV is not transmitted through a dirty toilet seat, and more than half (219/63.5%) answered that HIV is transmitted through the mosquito that is carrying the virus. This is summarised in Table 2.
3.4. Knowledge Regarding HIV Prevention
Knowledge of HIV prevention was assessed in six questions with yes and no responses. Most students responded correctly by answering that to prevent transmission of HIV, one has to properly use condoms (257/74.5%), screen blood before transfusion (309/89.6%), get tested, and know your partners status (300/87%), limit sexual partners (329/95.4%), take pre-exposure prophylaxis medication (286/82.9%) and take post-exposure prophylaxis medication (320/92.8%). These findings are presented in Table 2.
3.5. Relationship Between HIV/AIDS and Socio-Demographic Variables
Fig. (1) illustrates the student level of HIV/AIDS knowledge. When the sample was stratified into poor, average, and adequate knowledge, the results showed that (74) 21% students had a poor level of knowledge, (126) 37% had average knowledge, and (145) 42% had adequate knowledge. Table 3 illustrates the cross-tabulation of socio-demographic characteristics associated with HIV/AIDS knowledge. When Multiple Logistic regression was computed, age, gender, level of study, the field of study, and religion were some of the variables not significantly associated with knowledge. However, race was significantly associated as respondents who belonged to coloureds or mixed race were almost six times less knowledgeable about HIV/AIDS than blacks (OR = 5.77, C.I 95% (2.93-11:38)), as summarised in Table 3.
Table 3.
| Variable | Knowledgeable [%] | Not Knowledgeable [%] | MLR-OR [95%CI] | Chi-Square |
MLR- P-value |
| Age | |||||
| 18-25 years | 89.6 | 10.4 | *** | 0.122 | |
| 26-35 years | 74.3 | 25.7 | 1.92 [0.57 - 6.49] | 0.290 | |
| 36-45 years | 95.5 | 4.5 | 0.27 [0.02 - 1.62] | 0.123 | |
| Gender | |||||
| Male | 55.5 | 44.5 | *** | 0.117 | |
| Female | 72.9 | 27.1 | 0.65 [0.32 - 1.33] | 0.240 | |
| Race | |||||
| Black | 91.3 | 8.7 | *** | 0.000 | |
| Coloureds/ mixed | 54.1 | 45.9 | 5.77 [2.93 - 11.38] | 0.000* | |
| Level of study | |||||
| Third Year | 48.7 | 51.3 | *** | 0.404 | |
| Fourth Year | 43.2 | 56.8 | 1.89 [0.84-4.28] | 0.124 | |
| Field of study | |||||
| Agriculture | 93.3 | 6.7 | *** | 0.002* | |
| Maths and Natural Sciences | 81.8 | 18.2 | 3.08 [0.45-20.9] | 0.250 | |
| Health sciences | 75.0 | 25.0 | 10.91 [1.7-70] | 0.012* | |
| Human and Social sciences | 70.0 | 30.0 | 7.5 [1.3-43.09] | 0.023* | |
| Environmental Sciences | 65.5 | 34.5 | 5.74 [0.94-35.25] | 0.059 | |
| Law | 76.5 | 23.5 | 6.5 [1.02-41.4] | 0.047* | |
| Education | 93.8 | 6.25 | 1.56 [0.18-13.1] | 0.684 | |
| Management | 75.0 | 25.0 | 9.06 [1.3-62.52] | 0.025 | |
| Religion | |||||
| Christianity | 79.4 | 20.6 | *** | 0.005* | |
| Traditional | 20.0 | 80.0 | 14.41 [1.18-175] | 0.036* | |
| Hinduism | 100 | 0 | 1 | ||
4. DISCUSSION
The students in this study had inadequate knowledge about HIV/AIDS, with less than half (42%) of the students having a score above 20, which was low compared with other similar studies. Similar findings were also reported in a study among Egyptian university students, which reported that 35% of the students reported low score [45]. However, other university students in developing countries reported an adequate level of knowledge about HIV/AIDS. Studies conducted among university students in South Africa [22] demonstrated that 97.8% of the students had adequate knowledge about HIV/AIDS. Higher levels of knowledge have been observed in other African universities [46-51]. This can be attributed to long-decade investment in HIV/AIDS awareness by the local governments and the international community [22, 52]. Furthermore, high levels of education are associated with heightened knowledge levels [50, 52, 53]. The different student populations may explain the difference in knowledge about HIV/AIDS in this study. Some programs incorporate a significant amount of HIV and AIDS content by their design and targets, while some programs do not [45]. It is common for some programs [particularly in Health Sciences] to have more knowledgeable students about HIV and AIDS compared to some programs as there is usually much content covered on health-related issues, of which HIV and AIDS fit in that scope [45]. Inaccurate knowledge about HIV/AIDS might lead to poor attitudes towards HIV/AIDS; hence young people may indulge in risky sexual practices [50]. This calls for Higher Education Institutions to integrate HIV/AIDS content into their undergraduate curriculum to close knowledge gaps and misconceptions.
The study's findings also showed that race was a significant factor influencing the level of knowledge amongst our respondents with coloureds and mixed-race almost six times less knowledgeable than Blacks. These findings are almost similar to those of a study conducted at Jackson State University on Black African-American students that found over 96% of the students to be knowledgeable on HIV and AIDS issues [12]. However, some studies contradict this finding as they have found that the level of knowledge amongst blacks was significantly lower than that of whites [54].
The study also showed that most students knew that HIV is transmitted by sharing a needle to inject drugs with HIV positive, sexual intercourse, and having vaginal sex and anal sex without a condom. The findings are in agreement with two South African studies [50]. A cross-sectional study conducted among university students in Gauteng reported that about 98.1% of the female students and 96.4% of the male students knew that the virus could be passed on through unprotected sex. About 90.9% knew that a person could have HIV and pass it on to others without showing symptoms [50]. Furthermore, a study conducted among South African vocational universities concluded that 96% of students knew that the virus could be passed on through unprotected sex, and 71% knew that HIV could be passed from a pregnant mother to her unborn child [19]. A high degree of South African youth exposure to HIV/AIDS education programs may explain the findings [51].
Although the students exhibited knowledge about HIV/AIDS, they had misconceptions about how HIV was transmitted and prevented and the general facts about HIV/AIDS. The students incorrectly answered that HIV and AIDS are the same things (58.8%), and eating healthy foods can prevent getting HIV (47.5%). Of note, more than half of the students (52.2%) answered incorrectly that antiretroviral drugs can cure HIV infection. About 49% incorrectly answered that AIDS is an infectious disease caused by bacteria. Similar misconceptions about HIV/AIDS were reported in previous studies [55-57]. This illustrates that misconceptions about HIV/AIDS are still existent in South Africa and beyond. This can be ascribed to limited HIV/AIDS education among tertiary students. Furthermore, this can be explained by the fact that students only acquired basic technical information about HIV without knowing how the disease is transmitted [22]. The misconceptions visible in this study may lead students to indulge in risky sexual behaviours, leading them to acquire sexually transmitted infections, such as HIV [58].
The study also indicated no significant difference between male and female students regarding their knowledge about HIV/AIDS. The study findings are consistent with study findings conducted in South Africa [50, 59], African universities [59], and other parts of the world [20, 60]. However, some other studies showed that female students were significantly knowledgeable about HIV/AIDS than men [57, 61, 62]. It should also be noted that somestudies reported that male students possess higher levels of knowledge [45, 46].
The area of study did not influence the levels of HIV/AIDS knowledge score. This finding was not expected since previous literature suggests that most life and health sciences students know about HIV/AIDS [63, 64]. Furthermore, a study conducted among Malaysian university students showed that students from science faculties scored highly compared to non-science students concerning HIV knowledge [56]. Similar conclusions were also reached by a study conducted among American universities [10]. This can be explained by the fact that HIV/AIDS-related content is integrated into some university undergraduate academic programmes. Furthermore, having scientific knowledge is associated with a better understanding of the pandemic [50, 56]. Therefore, there is a need to integrate HIV/AIDS content into the undergraduate academic curriculum.
5. STUDY LIMITATIONS
The study's findings add to previous literature that suggests a need to integrate HIV/AIDS-related content into undergraduate curricula. As the study was conducted in one university; therefore, the results cannot be generalised and should be interpreted cautiously.
Therefore, there is a need to conduct the study on a large sample from different universities. The study used a self-reported questionnaire to collect data due to which recall bias can occur, and this can affect the data's quality. By virtue that these questionnaires were self-administered, the response rate was 77%. Some completed questionnaires were either not returned to the researchers or were incomplete and did not pass for analysis. This lowered the subsequent response rate.
CONCLUSION
The overall level of knowledge about HIV/AIDS among university students is high as it is above 80% on average; In terms of race, the levels are low for races, such as the coloureds and the mixed populations. Misconceptions about HIV/AIDS facts, transmission routes, and prevention aspects are still prevalent among higher education institutions. Therefore, there is a need to embark on awareness campaigns to ensure that correct information is disseminated to overcome these misconceptions, myths, and misunderstandings to foster desirable behaviours that would minimise the spread of HIV and AIDS.
LIST OF ABBREVIATIONS
| AIDS | = Acquired Immune Deficiency Syndrome |
| HIV | = Human Immune Deficiency Virus |
| HEIs | = Higher Education Institutions |
| C.I | = Confidence Interval |
| MLR | = Multiple Logistic regression |
| OR | = Odds Ratio |
| UNAIDS | = United Nations Programme on HIV and AIDS |
| HEAIDS | = Higher Education HIV and AIDS Programme |
| UNIVEN | = University of Venda |
ETHICAL APPROVAL AND CONSENT TO PARTICIPATE
The study was reviewed, and full ethical clearance was granted by the University of Venda Research and Ethics Committee [SHS/17/PH/08/1506].
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was obtained from all the participants prior to data collection.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
The research was funded by the University of Venda Research and Publications Committee [SHS/17/PH/16] and Higher Education South Africa [HESA] E376. The funders only provided financial resources to support the implementation of the study. The researchers wrote six-monthly reports to inform the funders regarding the progress of the study.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The author would like to thank the University of Venda for funding this study. The authors would like to thank the promoters of this work, the heads of departments, the deans of schools, faculty members, and students, who made this study possible.

