All published articles of this journal are available on ScienceDirect.

Challenges to Antiretroviral Therapy Adherence and Coping Strategies to Overcome Them: Qualitative Investigations of Adolescents Living with HIV, their Caregivers, and Clinicians in Vietnam
Authors Info & Affiliations
Abstract
Background:
Adolescents living with HIV (ALHIV) in Vietnam are known to struggle with adherence to Antiretroviral Therapy (ART).
Objective:
To examine treatment challenges and facilitators experienced by ALHIV from the perspective of adolescents, their caregivers, and providers, and to inform an adherence intervention.
Methods:
In-depth Interviews (IDIs) of adolescent/caregiver dyads and Focus Group Discussions (FGDs) with adolescents, caregivers, and clinicians were conducted in Hanoi, Vietnam. We used semi-structured guides to encourage open-ended responses. We queried the challenges adolescents experience taking ART medications and being adherent, their awareness of disease status, and facilitators to support high adherence. Audio-recorded IDIs were translated into English, and coded and analyzed in NVivo using a thematic approach.
Results:
A total of 78 individuals participated in the study. Forty individuals participated in IDIs (20 adolescents and 20 caregivers). All adolescents had acquired HIV perinatally. We conducted six FGDs: four with adolescents, and one each with caregivers and clinicians. We identified major themes regarding awareness of HIV status (most caregivers reported they had disclosed to their child, while few adolescents revealed the knowledge of their status); perceived barriers to adherence (medication-related challenges, stigma, school-associated issues, financial obstacles, system challenges, awareness of HIV status); and adherence facilitators (development of dose-taking habits, reminder systems, social support). Differences between adolescents and caregivers related to key issues were evident.
Conclusion:
Further research is needed to elucidate discrepancies in adolescent-caregiver viewpoints and develop interventions tailored to both ALHIV and their caregivers.
1. INTRODUCTION
Adolescents and young adults represent a growing proportion of PLHIV globally, with one-third of all new infections occurring in individuals aged 15–24 years [1, 2]. Recent research highlights disparities in the HIV care continuum for adolescents and young adults compared to adults [2]. Although data are relatively sparse, studies indicate that this population is challenging to reach and experiences a high risk of virologic failure [3], underscoring the need to improve HIV testing [4], retention in care [5-9], and ART adherence [8, 10, 11].
Adolescents face special challenges in part due to developmental changes that may include identity formation, behavioral experimentation, impulse inhibition, and risk-taking [12-14]. Adolescents living with HIV (ALHIV) often experience barriers to treatment, including stigma [15, 16], lack of social support [15-20], drug and alcohol use, and neurological deficits for those perinatally-infected [21]. Studies on ART adherence among adolescents and young adults reveal suboptimal adherence, with rates as low as 41% [20], much lower than their older counterparts [18]. Intervention studies have found that youth-tailored care [17], peer support networks [17, 22-25], and education-based interventions [26, 27] are associated with improved ART adherence and retention.
ART adherence and retention are generally suboptimal in low resource settings [6, 28-34], including in Asia [35]. In Vietnam, HIV remains a national health threat despite rapid ART expansion [36], largely due to challenges in HIV testing and ART uptake, adherence, and retention. Vietnam has among the lowest ART adherence rates in Southeast Asia, with an estimated 30% below 90% adherent. [35]. In Vietnam, an estimated 6,500 children and adolescents live with HIV [37]; in recent years, the first surviving cohorts of perinatally-infected children have transitioned to adult outpatient clinics (OPCs), with thousands more expected to transfer to OPCs in coming years [38].
Given the increasing number of ALHIV in Vietnam and evidence that ALHIV face ART adherence challenges, we conducted the Supporting Adolescent Adherence in Vietnam (SAAV) Study, a mixed-methods research study designed to improve understanding of the experience of ALHIV on ART. The study included a recently-completed randomized controlled trial (RCT) to test a mHealth adherence support intervention among ALHIV receiving treatment in Hanoi [39]. To better understand challenges to and facilitators of adherence among ALHIV and to inform the intervention, we conducted an initial qualitative study with adolescents, caregivers, and clinicians.
2. MATERIALS AND METHODS
2.1. Subjects and Study Design
This study was conducted from May-August 2017 in Hanoi, Vietnam, which was home to 28,668 PLHIV in 2019 [40]. The study site was the Infectious Diseases (ID) Clinic at the National Hospital for Pediatrics (NHP). In 2017, the clinic was staffed by 12 physicians and 24 nurses who provided treatment to about 450 HIV-infected children under age 18; approximately 200 were 12 years or older. Patients collected ART medications monthly, and at their visit, exams and adherence counseling were also conducted; CD4-count tests were carried out every 6 months and VL tests annually. At the age of 18, adolescents transitioned to adult outpatient clinics near their homes.
We conducted in-depth interviews (IDIs) of adolescent-caregiver dyads and focus group discussions (FGDs), two each with male adolescents and female adolescents, and one each with caregivers and NHP clinicians who provide ART care. Recruitment of adolescents was done with the assistance of clinicians using purposive sampling to ensure roughly equal gender and a variety of ages between 12-17 years old. Eligible adolescents on ART coordinated by the NHP, agreed to follow study procedures, and provided informed consent; caregivers were recruited simultaneously and provided written informed consent. Adolescents and caregivers participated in an IDI, an FGD, or both. All clinicians at the ID clinic were invited to participate and provided consent.
2.2. Data Collection
Trained interviewers conducted IDIs and FGDs in Vietnamese in private rooms at the NHP. For IDIs, a semi-structured interview guide was used, employing open-ended questions on the experience of taking medication, challenges and facilitators to adherence, and adolescent-caregiver relationships. Because some adolescents may not have known their HIV status, care was taken to avoid disclosure during IDIs, with ART referred to as “medication”. Adolescents were interviewed alone unless their caregiver asked to accompany them.
FGDs also addressed ART challenges and facilitators, and solicited input on the proposed mHealth intervention (described elsewhere) [39]. Questions queried adolescents generally, rather than participants’ specific experiences. The FGD with caregivers addressed experiences of caring for ALHIV, barriers to ART adherence, and ways to provide support. It did not ask about HIV among caregivers themselves. The FGD with clinicians focused on experiences treating adolescents, including barriers to adherence. FGDs and IDIs were audio-recorded and supplemented with written notes.
The study was approved by institutional review boards at the University of New England, the Institute of Population Health and Development (in Hanoi), and the National Hospital for Pediatrics (in Hanoi).
2.3. Analytic Methods
Audio-recordings were transcribed and translated into English by a bilingual translator, and English transcripts were reviewed for accuracy by a second investigator, then coded and analyzed using NVivoTM software [41]. Preliminary analysis produced major themes, with a further generation of sub-themes. We compared views and experiences between participant groups, and when both members of patient-caregiver dyads discussed a given topic, within-dyad convergence and divergence of statements to understand views between adolescent-caregiver pairs were examined. We prioritized responses by their frequency and also explored disparate views.
| IDI Participants | FGD Participants | ||||
|---|---|---|---|---|---|
| Characteristic | Adolescents (N=20) | Caregivers (N=20) | Adolescents (N=28) | Caregivers (N=8) | Clinicians (N=11) |
| Gender (female) (N/%) | 10 (50.0) | 15 (75.0) | 14 (50.0) | 5 (62.5) | 9 (81.8) |
| Age (years) (Mean/St Dev) | 13.8 (1.5) | 47.5 (14.1) | 13.8 (1.5) | 48.6 (13.4) | |
| Caregiver relationship to child (N/%) |
|||||
| Mother | 10 (50.0) | 3 (37.5) | |||
| Father | 4 (20.0) | 3 (37.5) | |||
| Grandparent | 5 (25.0) | 2 (25.0) | |||
| Other relative | 1 (5.0) | ||||
| Clinician role (N/%) | |||||
| Physician | 3 (27.3) | ||||
| Nurse | 7 (63.4) | ||||
| Psychologist | 1 (9.1) | ||||
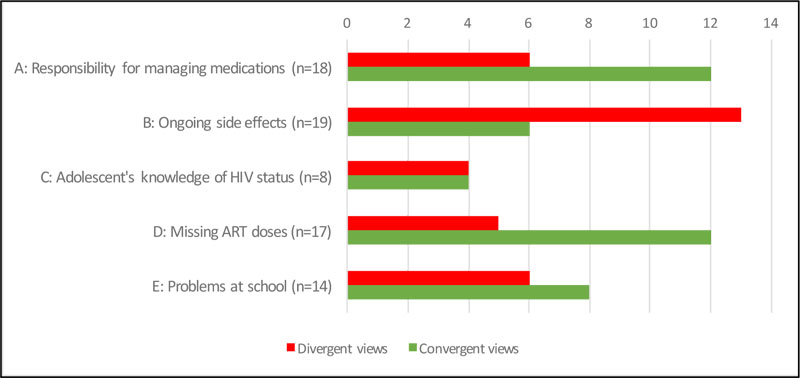
Notes: 1. When either adolescent or caregiver said nothing about topic or the response was unclear, that dyad was excluded from the within-dyad analysis. 2. Details on convergence/divergence by theme: A: Convergence (n=12). 3 dyads: adolescent has sole responsibility for managing medications; 9 dyads: adolescent/caregiver share responsibility for medications. A: Divergence (n=6): 6 dyads: all 6 adolescents: adolescent has sole responsibility vs. all 6 caregivers: responsibility is shared. B: Convergence (n=6). 1 dyad: yes, there are side effects; 5 dyads: no side effects. B: Divergence (n=13). 9 dyads: adolescents: no side effects vs caregivers: yes, there are side effects; 4 dyads: adolescents: yes, there are side effects vs. caregivers: no side effects. C: Convergence (n=4). 3 dyads: adolescent fully understands status; 1 dyad: adolescent does not understand status. C: Divergence (n=4). 1 dyad: adolescent fully understands status vs. caregiver: adolescent does not understand; 1 dyad: adolescent partially understands status vs. caregiver: adolescent fully understands; 1 dyad: adolescent does not understand status vs. caregiver: adolescent fully understands; 1 dyad: adolescent does not understand status vs. caregiver: adolescent partially understands. D: Convergence (n=12). 9 dyads: adolescent never misses/adherence is good; 2 dyads: adolescent sometimes forgets; 1 dyad: adherence is poor. D: Divergence (n=5). 5 dyads: all 5 adolescents: sometimes miss doses vs. all 5 caregivers: never misses dose. E. Convergence (n=8). 7 dyads: adolescent has no problems at school; 1 dyad: fears stigma or experienced actual stigma. E. Divergence (n=7). 6 dyads: adolescent: no problems at school/no fear of stigma vs. caregivers: fears stigma or actual stigma experienced at school; 1 dyad: adolescent: fears stigma vs. caregiver: no problems at school.
3. RESULTS
3.1. Overview
We conducted six FGDs (four with adolescents, one each with caregivers and clinicians) and 40 IDIs with 20 adolescent/caregiver dyads. A total of 78 individuals participated; 41 adolescents, 26 caregivers, and 11 clinicians (Table 1). The mean age of adolescent participants was 13.8 years (SD 1.5 years), of which 50% were females. The mean age of caregivers was 47.5 years (SD 14.1 years), of which 71% were females; 71% were a parent. Clinician FGD participants included seven nurses, three physicians, and a psychologist; most were female (9/11).
Major themes emerged regarding awareness of HIV status among adolescents and the disclosure process, as well as adherence barriers and facilitators. While many adolescent-caregiver pairs expressed similar views, some statements diverged on key themes (Fig. 1). Below we describe medication-taking by adolescents, and then HIV status knowledge and disclosure, adherence barriers, and, finally, facilitators of adherence. Direct statements illustrate findings, with additional statements provided in Table 2.
3.2. Medication-Taking
IDIs revealed that half of the adolescents (9/18 who spoke on this topic) felt they were responsible for their medication-taking, with little engagement of caregivers. Typical statements included: “For now, I take it by myself” and “No one [reminds me].” The other half indicated shared responsibility for medication-management. As a 13-year-old boy replied when asked who managed the medication container, himself or his mother: “Both of us.”
However, caregivers typically (15/18) portrayed medication management as a dual responsibility, including six caregivers of children who described independence regarding pill-taking (Fig. 1). For example, the grandmother of a 14-year-old boy, who said he managed his pill-taking, described a collaborative process: “Every morning, I take out the pills and give them to him, and remind him to remember to take it right when he gets to school.” While many caregivers stressed the maturity of their adolescents, several indicated that their children were too young to have sole responsibility for something so important and stressed their own role in medication management. The mother of a 14-year-old explained in an IDI: “He is at the naughty age. He sometimes forgets, so he essentially depends on me. For instance, when it’s time for him to take the pills, he and I usually take them together at the same time.”
3.3. Awareness of Status and Disclosure of HIV Status
Knowledge of one’s HIV status appeared mixed among adolescents. While most adolescents in IDIs said little about their HIV status specifically, partly because interviewers did not ask explicitly about it, of those who did (8/20), half indicated the knowledge of their HIV infection and what it meant. For instance, one participant claimed: “I already know so I didn’t ask” (IDI, 13-year-old girl). Several others had apparently never inquired and were unclear about the extent of their illness. Others seemed to lack awareness that they had a medical condition. For instance, a 14-year-old boy in an IDI stated: “I just think that it [the medication] makes me stronger.”
In contrast, nearly all caregivers (17/20) asserted that their child was aware of his/her status (Fig. 1), although four doubted that the child fully appreciated what this meant. The uncle of a 15-year-old girl explained: “She only knows that she has HIV, only knows the name of it, but does not really know what HIV is.” The others (3/20) indicated that their adolescents only knew that they were sick. Only four dyads were consistent in what the child understood; three pairs agreed that the adolescent understood his/her status fully, while one pair was consistent on the lack of knowledge (Fig. 1). Four pairs revealed divergent views, with the caregiver believing his/her child knew more than the child conveyed independently.
Closely related to adolescents’ knowledge of their HIV status was whether and how disclosure had been made to the child, which appeared to be a complex and troubling undertaking for many caregivers. Most (15/20) said that they had informed their adolescent about their status, while for others (2/20), doctors had conveyed this information. The remaining caregivers (3/20) had limited such discussions with their child, explaining that they planned an in-depth conversation in the future. Some (3/20) noted that disclosure depended upon the adolescent’s ability to comprehend the nature of HIV infection. This thought is illustrated by the uncle of a 15-year-old girl in an IDI: “I think we have to explain and talk to them logically and slowly so they can understand. … they might not be able to understand, so we still need to talk a bit about it to them.”
Preparation prior to disclosure was stressed by several caregivers. A mother of a 15-year-old explained in an IDI: “Before talking to her, I had to prepare in order for her to understand the disease…. First, I had psychological preparation to give her advice. Second, advising her helps her to understand so that her pill-taking is effective.” Clinicians played a critical role in this process. Some caregivers described having their adolescents meet with clinicians before they tackled disclosure. The father of a 13-year-old girl noted in an IDI: “Before [I told her] about her illness status, she had some consultancy sessions from her doctors.”
A number of caregivers revealed substantial reluctance to discuss HIV with their children. One IDI participant, whose 14-year-old grandson had learned of his status from a clinician, said: “I have never talked to him about this [HIV]… Never.” When probed further, she indicated fear of her grandson’s reaction: “I think it’s very hard. I’m afraid that he might get depressed.” Several worried about whether the child would understand his/her situation. A father of a 12-year-old boy explained in an IDI: “We don’t know what he feels, so we don’t want to talk about it with him. He just knows about the name of it, but doesn’t understand, so there is no need to talk to him.” Others were concerned about what the child might say to others. As a father said, “We are afraid that he will not be aware, can’t keep his mouth [shut], and talk with his friends. Then his friends might discriminate and won’t play with him.”
Conversely, several caregivers exhibited confidence and described straightforward conversations about HIV with their child. One mother of a 13-year-old girl said in an IDI that her daughter was “totally fine” when she learned of her illness. This mother “just talked to her, and she [the daughter] understood.” Others spoke movingly of these conversations (Table 2); for some, such communication was relatively natural:
At night, sometimes when it is the two of us, we lay down and talk to each other, about how was school that day, or how was soccer. Then I will tell him that his father had this also, also his brother, and they weren’t able to have the medicine, and that’s why they died. (IDI, mother of a 15-year-old boy)
In their FGD, clinicians noted that caregivers often experience difficulties discussing HIV with their children and solicit help to do so from the clinicians. They stressed that “the caregiver has to be ready,” and that sometimes, “the caregivers themselves are not ready.” They also stated that disclosure may affect an adolescent’s motivation to adhere to their ART medications, a topic addressed in more detail below.
| Disclosure and Knowledge of HIV Status | Adherence Barriers | Adherence Facilitators |
|---|---|---|
|
Discussions of HIV between caregivers and their children Generally, she cannot really understand about her disease because she is still a small child. We cannot let her know, either. (IDI, mother of 12- year-old girl) At the beginning, there was only me and my child. Then gradually, there were grandparents, and then both grandparents talked when we relaxed or were at the dinner table. And we said dad was like this, dad had [HIV] like that. You have to take medicine, since you now have the disease—not only you, but mom also has the disease, so he really understands. (IDI, mother of 14-year-old boy) Emotions felt when talking to child I feel like, I love her, she was so young when I talked to her about it, so I feel badly for her. … Yes, I did worry, I worried that she might feel negative or sad. I did worry, but I also supported and encouraged her.” (IDI, mother of 15-year-old girl) When asked how she felt when speaking to her son about his condition: “[smiling] [I felt] that I really care for him.” (IDI, mother of 14-year-old boy) Knowledge of HIV status [When asked about whether his child knows his disease status:] Yes, I think he knows now. At first, he usually asked “Dad, why do I have to take these pills, I’m not sick” At that time, it wasn’t a right time to talk to him. We just said that you have to take it, that you could get sick any time. So you have to take pills. Your life depends on these pills. So you have to take it every day, even if you’re not sick. And he didn’t say anything else. Sometimes he asked grandparents, they said the same thing, so he didn’t ask again…We don’t want to talk clearly about this to him, but in the future, we will. But now, we don’t want to talk to him…So we don’t know what he feels, so we don’t want to talk about it with him. He just knows about the name of it, but doesn’t understand, so no need to talk to him. (IDI, father of 12-year-old boy) [When asked about relationship between knowledge of disease status and adherence:] I see in the clinic there are two major problems. For kids whose parents already told them their disease, they have very good adherence. Whereas for kids who don’t know, they don’t know the importance of taking pills on time, so this is a problem. (Clinician FGD, psychologist) |
Side Effects Every time he changes the pills, he has new side effects, so he can’t eat anything. And then he gets tired or sick. (IDI, grandmother of 14-year-old boy) Since she has been taking medication, she has not had side effects. Maybe at the beginning, she had a rash or diarrhea. In these situations, we stopped taking pills and [asked] the doctor to change to another kind of medication. (IDI, uncle of 15-year-old girl) He was tired and stopped taking his medicine for a year. He had diarrhea until he felt scared. He was so thin you could see his bones, leg bones, arm bones. Then he was only skin and bones, so I brought him to the hospital for 10 days, more than 10 days. (IDI, grandmother of 15-year-old boy) Stigma I came to school to talk with teachers because they didn’t let him study, and he was put in the corner of the class. So, I looked at his notes, and there was nothing written down. He said his teacher put him in the corner and didn’t let him study….. I went to the dean and [he] said if teachers knew that he has a disease and are afraid that he transmitted it to other kids, [we can’t] let him study here…. (IDI, grandmother of 15-year-old boy) I am afraid that when she grows up, for example, associating with friends or there’s someone who loves her, what would happen if they know about her disease? We think a lot [about this].” (IDI, mother of 12-year-old girl) Since she began secondary school, it’s gotten better. She doesn’t get into any trouble. Most of the teachers know about this so there aren’t any troubles. (IDI, grandmother of 14-year-old girl) Financial challenges Overall, it’s quite expensive to travel. For both of us, the cost is about 600-700 thousand dong [US $25-30]. … Every time we have to come here, it’s hard. It’s not easy. We live quite close to here. There are people who live far away, farther than us. I don't know how they can get here. (IDI, father of a 12-year-old boy) ….Actually I have to rent a motorbike taxi which costs about 250,000 dong, because we don’t have a vehicle, while the bus here causes us [to be] car sick. The traveling for us is really difficult. You see, I just earn 200,000 dong a day, but the cost to get here per month is 250,000 dong, so sometimes I didn’t come to take pills. Honestly, traveling is really difficult for my family… our family is in the poor condition, her father has not worked since he had an accident two years ago. (IDI, mother of 15-year-old girl) |
Establishing a routine Normally we counsel or advise patients to take pills when it’s appropriate for them—for example, when the time does not affect the patient’s school time, or to take pills at home before going to school. And it is very easy to drink at night. (FGD, clinician) I rarely [set my alarm]…I got used to [taking pills]. (IDI, 14-year-old boy) …In the past, I used to set an alarm by cellphone but now it is a habit. As the meal comes or by being reminded by the family members, [he] takes the medicine. (FGD, father of 14-year-old boy) Reminders Generally, when he wasn’t used to it, [it was difficult]. Sometimes he did take his pills about 15 to 20 minutes late. But after getting used to it as well as setting an alarm on the phone and having help from others, it is now a habit …because he is not the only one who is sick. I am, and he is, too. (IDI, father of 12-year-old boy) [When asked about the reminder system for his child:] My kid at home still needs a caregiver to remind him Overall, it’s just that he doesn’t fully follow the rules, so we still need people to help and to remind him. (IDI, father of 12-year-old boy) [When asked why his child forgets to take pills:] It’s because now she is grown up, so sometimes she plays with her sister or brother. My family has many kids, so she might forget, so her grandparent or I have to remind her. (IDI, uncle of 15-year-old girl) [When asked about best reminder system:] I think it’s to set an alarm early in the morning so I don’t wake up late…[and in the afternoon] not playing too much and not forgetting to take pills…I think having an alarm is the most convenient. (IDI, 13-year-old boy) It was difficult to take the medicine on time as he was small because I had to work but now he is able to take medicine without my help, I just set an alarm in the cellphone to remind him to take medicine…now, he is matured so he knows to do it. (FGD, grandmother of 12-year-old boy) |
|
School-related challenges [When asked about her child taking ART at school:] Because he doesn’t dare to take medicine in front of his friends, he goes to drink water and go to toilet then he takes medicine, when we enroll him in the class, we talked clearly with his teacher in advance that he has the disease, my family doesn't hide it, doesn't hide his disease from his teacher. (IDI, mother of 14-year-old boy) [When asked how long his child has known about his HIV status:] He has known since he was in kindergarten school. His friends laughed at him and jeered him. When he was back home, he asked why his friends said he was sick with AIDS. We all said don’t worry about that. They are just joking; it doesn’t matter. (IDI, father of 12-year-old boy) |
Social support [When asked about support from others in her community:] I learn from the others who are also in the same condition as me. We talk and share with each other, about some topics that I understand, some I don’t. Then I come and talk to them, and share with them and then share with my child. (IDI, mother of 15-year-old girl) [When asked about the primary motivators for her child’s adherence:] Generally, the family’s encouragement is the main motivation. They are mature and they know more. (FGD, grandmother of 12-year-old boy) |
3.4. ART Adherence and Barriers to Adherence
Participants generally agreed that adherence among child participants was relatively high (Fig. 1). Most adolescents (10/17 in IDIs, 14/28 in FGDs) asserted that they never missed doses. “No, I don’t forget” was a typical statement. Most noted that taking their medications was part of their morning routine. A 12-year-old girl in an IDI stated: “In the mornings, I take medicine frequently. Before I go to school, I take medicine.” Some (9/20 in IDIs, one FGD participant) said that they would tell their caregiver when they missed or took a dose late. Others (2/20 in IDIs, one FGD participant) stated that they would not reveal lapses because they feared their caregiver would be angry.
Similarly, most caregivers (16/20 in IDIs, 4/8 FGD participants) described perfect or very high adherence among their respective adolescents. Most (9/16) were in agreement with their child; however, five cared for an adolescent who described lapses (Fig. 1). Several caregivers stressed their focus on adherence with their children, often from an early age, like this father of a 14-year-old boy: “…I talked with him that he should take medicine on time throughout his life. If he took medicine on time, he would be healthy …. Then, he took medicine regularly, and now he knows how to do it.” Another FGD participant explained that her grandson felt strange when he missed doses. When queried further, this grandmother elaborated: “It makes him tired, sick. …. my grandchild told me that he feels different if not taking medicine on time, so I set the alarm… to remind him to take medicine on time.”
Both caregivers and adolescents agreed that when doses were missed, it was mainly due to evening social activities. As a 14-year-old girl responded in an FGD, when asked when she might forget to take her medication: “In the evening, [because] I am absorbed in playing.” The mother of a 14-year-old boy said that her son missed doses “…[at] times when he was too focused on playing.”
Clinicians acknowledged that some adolescents were poorly adherent. They described situations in which caregivers had insisted that their child’s adherence was good, and yet the child had developed drug-resistance over time, suggesting poor adherence. The clinicians also described instances when adolescents resisted caregivers’ efforts to support adherence. One female nurse explained: “… Some patients are under the parent’s control, but then they hide it [the pill] or they just keep the medicine in their mouth and then spit it out later. This is a difficulty.”
Participants also described a range of adherence challenges, particularly medication-related challenges, stigma, school-associated issues, financial obstacles, system challenges, and awareness of HIV status, each of which is examined below.
3.5. Medication-related Challenges
About one-fourth of adolescents (6/20 in IDIs, 4/28 in FGDs) revealed ongoing medication-related problems, including pill taste and size, but mainly side effects. They described tiredness, nausea, vomiting, and being uncomfortable. However, half of the caregivers (10/20 in IDIs, 4/8 FGD participants) indicated that their adolescents experienced side effects. As one mother of a 12-year-old girl explained in an IDI, “The regular difficulty is the uncomfortable feeling after taking the medication. She vomits sometimes. If there’s medication in the vomit, she has to take another one.” Within-dyad divergence on this topic was notable (Fig. 1); only one adolescent whose caregiver described side effects expressed a similar view. Two child-caregiver pairs agreed that side effects had been a challenge at first, but had diminished over time. One caregiver stated that her grandson’s side effects had been so severe that he stopped his medications altogether. Additional statements are provided in Table 2.
Clinicians agreed that side effects persisted among adolescents, explaining that side effects are common when beginning a new drug regimen or taking medications for long periods of time. As one elaborated, “Yes, side effects are still present when taking medications, such as anemia, or when patients have taken a new regimen, this is a common response. Patients on one regimen for a long time may have anemia.”
3.6. Stigma
Enacted and anticipated stigma represented a challenge for some participants, but not others. Among the adolescents, about one-third overall (9/20 in IDIs and 5/28 in FGDs) stated that classmates knew they had to take medications and did not treat them differently, though most peers were unaware of the medications’ purpose. A similar proportion (7/20 in IDIs, 8/28 in FGDs) claimed that their peers and teachers did not know their HIV status, so stigma was not an issue. Some (1/20 in IDIs, 5/28 in FGDs) described fearing that teachers and/or classmates at school would learn about their HIV status. One 13-year-old girl revealed in an IDI: “Yes, I am afraid. [The hardest thing I have to deal with] is hiding my disease from others.”
Enacted stigma was described by a similar proportion of adolescents. Some (1/20 in IDIs, 5/28 in FGDs) described being shunned socially when fellow students discovered their status. One 14-year-old girl (FGD) explained: “When their parents tell them about my disease, they do not want to be close to me...Yes, they are [afraid to play with me].” Only one child, a 15-year-old boy in an IDI, described feeling stigmatized by teachers:
Q: How does your teacher treat you?
A: Her behavior is not quite respectful.
Q: It means that she discriminates against you?
A: Yes.
In contrast, half (9/20 in IDIs and 4/8 FGD participants) of the caregivers expressed anticipated stigma, both in their neighborhoods and at their child’s school. Several described trying to prevent neighbors from discovering their child’s status, and keeping their child isolated from other children. As the grandmother of a 12-year-old girl, who suffered from infection-related skin problems, noted in an IDI: “She only stays inside the house. When she was in grade 4, she still had friends…. But [now] … we are afraid her friends will find out, so she has to stay at home.” Others described gossip in their communities: “…Some people are talking, and we know that, that means people around here do have prejudice …. People do not feel comfortable with this type of disease....” (IDI, mother of a 15-year-old girl.)
Many caregivers (7/20 in IDIs, 4/8 in the FGD) indicated anxiety about potential stigma at school from teachers or students, though their children either did not mention stigma or claimed he/she experienced no problems at school (Fig. 1). A mother of a 13-year-old boy explained: “I’m afraid that if they found out, they will talk badly about him.” Several caregivers described requiring that children take medications at home to avoid dose-taking and risk of disclosure at school.
Similar to adolescents, caregivers’ depictions of enacted stigma in school settings were rare. One mother of a 14-year-old boy said that her son had shared with her instances when classmates treated him badly. When asked whether these difficulties came from his friends, the caregiver responded: “Yes.…when he goes to school, the friends somehow discriminate and some even avoid him.” Another caregiver, the grandmother of a 13-year-old girl, noted: “… Sometimes during parents’ meeting, some of the parents, they don’t want to be near her. …. She sometimes feels sad [and] doesn’t want to go to school anymore, so my family and I have to encourage her.” In one case, a caregiver revealed that her grandson had quit school due to feeling stigmatized by teachers (Table 2).
Clinicians confirmed these fears of school-based stigma, acknowledging the strategy adolescents often employed in choosing to take their medications at home rather than at school. One clinician explained: “… the child is afraid of someone finding out why they must take pills. When taking medicine at school, they are afraid that people will see them taking many pills.”
3.7. School-related Challenges
Beyond school-associated stigma, several adolescents described difficulties due to missing school, mainly for monthly clinic visits and medication pick-up. As one 12-year-old child in an IDI responded, when asked what was the hardest thing about his medications: “I have to skip classes.” Several others described making excuses for missing school, like this 13-year-old boy in an IDI: “Yes. …. [I said] “Teacher, I have a health check appointment today.”
Both clinicians and caregivers indicated that children’s absences from school to collect medications could impact their education negatively. When asked whether her patients faced discrimination, one clinician explained: “They always try to ask the teacher for absence from school to go to the clinic, and if they have too many absences, they are afraid of the teacher.” Some caregivers (6/20 in IDIs, 4/8 FGD participants) also described school absences as a problem. One mother of a 15-year-old boy elaborated: “In Dong Anh, adults can collect medicine every two months. Meanwhile, children must do it every month, so they have to call their teachers for an absence, or they’ll be punished.” Several caregivers revealed stress from these absences and pressure to explain them to teachers. One participant explained:
Every month, coming here to get pills takes us all day. We spend one day to get here. For him, he has to skip one day of school. If it’s a holiday, then it’s fine. But then every month I have to ask his teachers and lie, and say that there is some stuff at home so he has to skip school. (IDI, mother of a 13-year-old boy)
3.8. Financial Issues
Nearly half of caregivers (8/20 in IDIs, 3/8 FGD participants) described financial or time-related burdens caring for their adolescents. The mother of a 15-year-old boy explained in an IDI: “It’s just that I don’t have money to buy milk for him. …. When they come over, neighbors also give us 200-300 thousand dong. My parents are also poor, so it’s just the two of us depending on each other to live.” The most commonly-noted financial burdens, mentioned by about one-third of caregivers (6/20 in IDIs, 3/8 in FGDs), were related to purchasing additional (non-ART) medications or monthly clinic trips to retrieve medication. As the grandmother of a 13-year-old girl stated in an IDI: “Honestly, we’re in the countryside. We don’t get paid…. we’re old and uncles and aunts have families of their own. So, sometimes it’s quite hard for us to buy medicine for her.” The cost of travel to the clinic posed major challenges for a number of caregivers (4/20 in IDIs, 2/8 FGD participants). Additionally, some (6/20 in IDIs, 1/8 FGD participants) complained of having to take time off work to go to the clinic. The father of a 14-year-old boy explained in an IDI: “We have no choice…Each time I bring him to the hospital, I have to take off one day.”
Financial pressures affected caregivers and their quality of life; many spoke of high levels of stress and/or anxiety related to daily pressures and fear for their child’s future: “…We are not in easy circumstances. Everyone is worried when something happens to their children. … Having no money, you cannot save your child and this disease is not mild. … I am anxious for each day she grows up, so much anxiety.” (IDI, mother of a 12-year-old girl.)
3.9. System Challenges
Clinicians highlighted the difficulty adolescents experienced when transitioning to adult outpatient clinics at age 18, required by the national insurance system. They explained that patients preferred to remain at the pediatric clinic because it was familiar. As one clinician elaborated: “They don’t want to leave. They just want to stay… The children get used to coming to the clinic here, and then they have to move.” The move to an adult clinic could represent an abrupt adjustment:
…. When the children come here, the environment is open and they share. Sometimes in the adult clinic, the environment is completely different. All patients are adults and the kind of patient is different from the environment here. … In summary, I only see that the transition is most difficult. The children try to linger [at the pediatric clinic]….(FGD, clinician)
3.10. Awareness of HIV Status
For clinicians, children’s motivation to maintain high ART adherence was linked with HIV disclosure. One clinician noted, “For kids whose parents already told them about their disease, they are very adherent. ….for kids that don’t know, they don’t know the importance of taking these pills on time. This is a problem.” Another clinician described a recent encounter: “Yesterday, there was a 10-year-old patient. The mother hasn’t disclosed everything about the sickness to the child. So, when telling the patient to take medicine, he said he doesn’t like it.”
3.11. Facilitators of ART Adherence
Three main adherence facilitators for adolescents were apparent: developing dose-taking habits, reminder systems, and social support.
3.12. Forming the Habit of High Adherence
Participants spoke frequently about adherence to habit formation. Among caregivers, about one-third (4/20 in IDIs, 6/8 in the FGD) described routines, often linked with rising in the morning, returning home after school, or meals. One father of a 13- year-old stated in an FGD: “The medicine is like the food to be served on time, as a habit.” A fellow caregiver agreed, noting: “Habits make them follow it unconsciously….” Several children spoke similarly. When asked whether he faced any challenges taking his ART pills on time, one boy replied: “I feel normal because it’s like a habit to me.” (IDI, a 14-year-old boy)
Clinicians likewise noted positive habit-formation among their patients and their own role in supporting such behaviors. One clinician noted, “Actually, most children are teens who have visited the clinic for a long time. They have gone to the clinic for many years, probably from 2008 or 2009, so by now, they are used to such things. I think that taking medicine, missing doses, or other things about medicine are over. It's a matter of routine.”
3.13. Reminder Systems
For both adolescents and caregivers, setting an alarm was a critical adherence-support strategy. “I think setting an alarm is the best way” was a common statement. Some adolescents (11/20 in IDIs and 7/28 in FGDs) described using a phone alarm or alarm clock to take medication on time. Caregivers (12/20 in IDIs and 5/8 FGD participants) agreed that alarms were helpful. In an IDI, the mother of a 15-year-old girl described her adolescent’s alarm usage: “I give her a phone and she sets the alarm clock herself. I also keep reminding her to charge it to avoid the case of running out of battery. She forgot sometimes when she was 4-5 years old, but now, she is 15-16, and the essential thing is the phone, so she won’t let it run out of battery.”
Most adolescents (14/20 in IDIs, 18/28 in FGDs) asserted that a family member reminded them to take their pills. For some (4/20 in IDIs, 4/28 in FGDs), these in-person reminders were more effective than alarms. When probed about this support, one 14-year-old boy in an IDI explained: “Because sometimes I couldn’t get up or didn’t hear the alarm, so having someone remind me will be much better.” A 12-year-old girl in an IDI described relying on her caregiver, but with an alarm back-up: “For me, if my grandma is busy, then I set an alarm, maybe 5 minutes before, so I can remember and go to get the pills.” For some adolescents (11/20 in IDIs, 6/28 in FGDs), grandparents were especially important in this regard, particularly when parents were away working.
Several caregivers (4/20 in IDIs, 2/8 FGD participants) stressed that it was helpful when other family members were also on ART because reminders could be used for everyone, with doses taken together in a supportive fashion. When asked about the best way to remind her son to take medications, the mother of a 14-year-old boy commented in an IDI: “He takes pills at the same time as his father, so when his father takes it, he takes it also.” (See Table 2 for additional statements.)
3.14. Social Support
Adolescents described support primarily within their homes. Nearly half (8/20) described speaking with their caregivers about taking medications in a way that conveyed receiving support. As a 14-year-old boy in an IDI stated: “I share with them about the difficulties…I ask them when I will get better.”
While all adolescent and caregiver participants viewed their relationships as supportive, the level of HIV-related communication varied. As noted above, many caregivers expressed an open attitude and ability to discuss HIV and ART with their child. This grandmother provided an illustrative statement:
It’s not hard for us to talk about this [HIV]. Sometimes before sleep, she asks me how long will she have to take these [the pills]. I just tell her that because she has this disease, she has to take them on time every day, regularly. (IDI, grandmother of a 14-year-old girl)
Conversely, just over half of IDI participants (11/20 adolescents, 11/20 caregivers) conveyed a reluctance to share HIV-related experiences and medication-taking challenges. A 14-year-old girl in an IDI explained: “I don’t share with anyone [about my troubles taking pills].” A number of caregivers confirmed this hesitation: “No, he doesn’t talk about that [side effects]. Even when he is tired, he never talks or shares with mom and dad.” (IDI, father of a 12-year-old boy.)
Some clinicians (3/11) were emphatic about the importance of home-based support for children, particularly adherence support. One felt that encouragement from a family member was critical for adolescents, noting that non-parental caregiving could be problematic: “In my counseling experience, if the caregivers, like grandparents, they really care about them. [But] some caregivers are not their parents, so the level of care is not enough…. it’s difficult for the kids.”
Some adolescents (2/20 in IDIs, 6/28 in FGDs) and caregivers (6/20 IDIs, 1/8 FGD participants) spoke of support at school. While adolescents typically described their peers as neutral or as acting “normally” toward them, two (both in FGDs) along with several caregivers (all in IDIs) depicted teachers as supportive. For instance, one 14-year-old girl stated that her teacher was “…Very kind. She encourages me to try to eat sufficiently to have a good health.” The mother of a 12-year-old boy explained it this way:
“He goes to school without my help, and at school, teachers also care about him. The head teacher really cares about students, and she knows our problems, so she and also the school [generally] creates a lot of opportunities for us.”
4. DISCUSSION
This qualitative study is one of the first to focus on the ART-related experiences of ALHIV in Vietnam, particularly ART adherence barriers and facilitators. The study is strengthened by data collection from child-caregiver dyads and ART clinicians that allowed triangulation of data and comparison of views between ALHIV and key players in their HIV treatment environment. We have a number of important findings related to dose-taking, challenges faced by ALHIV and their caregivers, and sources of treatment support. On some topics, the study revealed similar views between adolescents and caregivers. However, divergent views emerged on other issues, highlighting the varying ways different people experience HIV, with important implications for programs aimed at strengthening ART outcomes among ALHIV.
First, a major finding was notable disagreement among caregiver-adolescent pairs among caregiver-adolescent pairs on two major topics: ART medication management and knowledge among the children of their HIV status. With regard to the former, a substantial proportion of children claimed that they had sole responsibility for managing dose-taking, whereas their caregivers claimed it was a shared task. Adolescents may be aware of their increasing role in taking medication independently, while caregivers are acutely mindful of their continued role in ensuring that pills are taken correctly. Agreement on roles is obviously important for effective therapy and has been shown to be a predictor of optimal adherence [42]. Clearly-defined responsibilities can also be critical for the caregiver-adolescent relationship; adolescents typically take on greater responsibility for their medications as they mature, ideally within the context of supportive family relationships [42]. Although most caregiver-adolescent pairs in our study were in agreement, differing views of adolescents as they age may be important for clinicians to anticipate, so they provide effective support.
The other area of disagreement was related to the adolescents’ knowledge of their HIV status. Among the child participants who discussed this in detail, half responded differently than their caregiver. Such disagreement is concerning given the threat posed to clear communication and collaborative efforts within households to manage adolescent ART effectively. Importantly, many caregivers exhibited obvious reluctance to disclose their child’s status to him/her and discussing HIV generally. We have observed this challenge elsewhere in Asia [43], as have researchers in other settings [44-47]. Effective disclosure is critical, both in enhancing health outcomes for children and in preventing HIV transmission to others [48]. Our caregiver participants spoke frankly about wanting to disclose when their children were sufficiently mature and about the role clinicians played in disclosure. With these points in mind, our findings add to the evidence highlighting the need for programs to support caregivers in disclosure of HIV status to their children and to educate adolescents on HIV and ART.
Second, we found a high degree of agreement regarding both ART adherence, which most participants portrayed as relatively high in our population, and adherence facilitators in this population. Yet, it is important to highlight the fact that among the adolescent IDI participants, one-fourth described adherence lapses of which their caregivers seemed unaware. Clinician participants were more pointed about the degree of poor adherence experienced by some patients, revealing frustration with both nonadherent adolescents and with caregivers who would not acknowledge and discuss lapses. As with disclosure, strengthening support to both caregivers and clinicians who treat ALHIV, along with adherence-promoting interventions designed for adolescents, will be essential to ensure effective ART management for ALHIV.
The agreement among participants regarding adherence facilitators for ALHIV was notable. This encompassed development of dose-taking habits, use of reminders, and social support. While these have been identified previously [49-55], to our knowledge, this is the first time they have emerged as adherence facilitators for ALHIV in Vietnam. Perhaps most prominent was consistent identification of ‘habit’ as indicative of an internalized dose-taking routine. All three participant groups stressed the importance of linking daily events with pill-taking and with making it a normal activity in the home. Frequent use of alarms or reminders can be viewed as both independent facilitators and essential to the process of habit-formation over time. For effective social support, open communication about HIV between children and caregivers is critical, as our clinician participants stressed repeatedly. The strong association clinicians made between verbal encouragement at home and adherence—and their concern that some caregivers failed to provide such support—was consistent in their views regarding disclosure and its part in helping adolescents understand the need for adherence. This finding reinforces the need for interventions to assist caregivers of ALHIV, including programs focused on communication skills.
Third, this study revealed important adherence barriers for ALHIV, including side effects and stigma. Prior research has identified side effects for patients generally [56, 57], and for adolescents specifically [49, 58]; our study confirms the burden of prolonged medicine-related effects on ALHIV in Vietnam. Similarly, stigma is a well-cited adherence barrier globally [59-61]. For children, school-associated stigma has been observed in multiple settings [62-66]. Our findings highlight the ways in which anticipated stigma continues to influence caregiver and child behaviors, including avoiding pill-taking at school, making excuses for missing school, and hiding ART from teachers and peers. Caregivers in our study also feared stigma from neighbors, keeping children at home, despite the resulting emotional and/or social isolation of their children. Most adolescents did not describe stigma explicitly, but those who did conveyed negative impacts, including ill-treatment by peers and teachers. Of note, caregivers in our study were more likely to describe both side effects and stigma than adolescents; substantial discordance was evident even within caregiver-adolescent pairs. Such discrepancies have been described previously, including regarding stigma [67]. In our study, it is hard to know whether views genuinely varied or whether caregivers were more comfortable discussing potentially distressing subjects. In addition to warranting more research to better understand these divergent views, our findings suggest that school-based programs to reduce HIV-related stigma should be a priority.
Fourth, an important finding emerged among caregivers: the striking nature of the financial and time-related costs associated with caring for ALHIV. Though not a new issue [43, 68, 69], the degree of distress conveyed by caregivers is noteworthy given the study’s context—a hospital in the capital of a middle-income country, where ART is provided free of charge. In part, this relates to the fact that many children receiving ART in Vietnam must travel for treatment. Our caregiver participants were often poor, elderly, and/or caring for more than one PLHIV. Their accounts of high stress and anxiety echo findings from research on psychological effects experienced by caregivers of PLHIV elsewhere [70-73]. They also underscore the need for interventions to assist caregivers of ALHIV in Vietnam, including programs that provide both emotional and financial support.
Finally, we acknowledge several limitations. This study included a small number of participants from one clinic in northern Vietnam, which may reduce the generalizability of findings. Participants may have provided misleading information due to poor recall or social desirability bias, a common limitation of qualitative research. Despite these limitations, this is one of the first studies to focus on ALHIV in an Asian setting. Our use of multiple data sources allowed triangulation of a rich array of information pertaining to experiences of a Vietnamese adolescent on ART, yielding important themes related to adherence barriers and facilitators that may inform interventions to improve outcomes for ALHIV in Vietnam and other settings.
CONCLUSION
This qualitative investigation sheds light on barriers to ART adherence among ALHIV and the coping strategies adolescents and their caregivers have developed to support adherence in this population. While participants agreed on key facilitators of adherence, they also revealed divergent views regarding HIV disclosure and specific barriers to adherence. This suggests a need for further research to understand better the reasons for discrepancies between ALHIV and caregiver accounts and for interventions tailored for caregivers of ALHIV as well as for adolescents themselves as they prepare to transition to adult care.
AUTHORS’ CONTRIBUTIONS
LLS shared overall responsibility for study conception and design (with MBD), helped manage and analyze data, interpret findings, and draft the manuscript.
VCN assisted in study design, implementation, and data collection, and helped interpret findings and draft the manuscript.
KH assisted in study design and played a key role in data analysis, interpretation of findings, and drafting of the manuscript.
RB assisted in study design and helped interpret findings and draft the manuscript.
LTH contributed to the overall study design, and helped interpret findings and draft the manuscript.
NVL helped interpret findings and draft the manuscript.
LTY helped interpret findings and draft the manuscript.
ALG contributed to the overall study design, helped interpret findings and draft the manuscript.
JEH contributed to the overall study design, and helped interpret findings and draft the manuscript.
DTL contributed to overall study design, assisted in study implementation, and helped interpret findings and draft the manuscript.
MBD shared overall responsibility for study conception and design (with LLS), conducted on-site training for data collection, assisted in study implementation, and helped interpret findings and draft the manuscript.
All listed authors contributed to the final manuscript.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and review boards at the following institutions: 1) University of New England, , Australia (Approval letter #071316-001); 2) the Institute of Population Health and Development, Vietnam (Approval reference #2016/PHAD/SAAV-01-01); and 3) Ethics Committee of the National Hospital for Pediatrics, Research Institute for Child Health, Vietnam (Approval reference #VNCH-RICH-16-015).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
The authors confirm that they obtained informed consent from all the caregivers (some parents, some not), as well as informed assent from the adolescents.
AVAILABILITY OF DATA AND MATERIALS
We are still analyzing the study data. We plan to make the transcripts public at the University of New England at a future time once the analysis is complete. In the meantime, requests for access to the data can be made to Dr. DeSilva at mdesilva1@une.edu.
FUNDING
We acknowledge support from the United States National Institutes of Health, Institute for Mental Health (NIH/NIMH 1R21 MH109381-01).
CONFLICT OF INTEREST
JEH has received consulting fees from Merck. LLS has received consulting fees from the Khesar Gyalpo University of Medical Sciences of Bhutan. The authors declare that they have no conflicts of interest.
ACKNOWLEDGEMENTS
The authors acknowledge the funding provided by the National Institutes of Health. We also thank all the adolescents, caregivers, and HIV providers in Hanoi who participated in this study. Their willingness to share their personal stories made this study possible.

