All published articles of this journal are available on ScienceDirect.

HIV Treatment and Care Services in Yemen: Implications Of Internal Country Conflicts
Abstract
Introduction:
Yemen has been experiencing an internal conflict since 2011 influencing the HIV treatment program.
Objective:
This study aims to assess the implications of internal country conflicts on HIV-treatment program performance for policy formulation, programme planning and national resource mobilization.
Methodology:
Secondary data analysis and mixed methods of quantitative and qualitative were used. Data analysis was conducted through SPSS. The sample size was 84 for quantitative and 35 for qualitative.
Results:
Mean age of PLHIV was 40.5 (±10.6 SD) years and 64.3% were males, 42.9% married, and 9.5% had HIV-positive children. 84.5% of PLHIV have more than one symptom at the first visit and most of them presented late with clinical stages 3 and 4. HIV/TB co-infection represents 9.5% for pulmonary TB and 2.4 for extrapulmonary TB. Access to ART during the conflict significantly depended on the residence of PLHIV (p < 0.0005) and (95% confidence interval (CI): 2.48 to 1.22) and on the availability of the clinic (p < 0.0005) with (95% CI: 1.007 to 1.953). 41.7% of PLHIV were LTFU, 25.7% gave conflict as the main reason, 66.6% of PLHIV experienced a change in ART regimen per lifetime, and 70.9% of them gave ARV stockout as the main reason. Most PLHIV had difficulty accessing services during conflict. Most PLHIV (13/20) were not comfortable with the quality of service. All HCPs mentioned that the HIV-treatment program is funded only by the Global Fund and experienced shortages of ARVs before and during the conflict.
Conclusion:
It is important to have national policies and resources for HIV-treatment programs so one can ensure the sustainability of services.
1. INTRODUCTION
Human immunodeficiency virus (HIV) treatment and care are consecutive stages of HIV medical care that people living with HIV (PLHIV) go through from the date of HIV diagnosis to the date of receiving antiretroviral therapy (ART) and reaching viral suppression [1, 2]. It has been recognized that ART has broader benefits in the prevention of sexual transmission of HIV and in improving the quality of life of PLHIV [3-5]. Nowadays, there is no doubt that antiretroviral drugs prevent HIV infection [6]. However, it is necessary to reach optimal adherence to ART to promote viral suppression and prevent HIV transmission, disease progression, and mortality [7]. Therefore, ART is used as secondary prevention in an infected person, and it can also be used to prevent HIV transmission either before exposure through preexposure prophylaxis or post-exposure prophylaxis [8].
Widespread wars in the Middle East extended beyond the direct killing of people and the destruction of infrastructure. It diverted public funds to military spending and created a need for humanitarian assistance due to a decline in financial resources. Therefore, the lack of supply of basic goods, unemployment, and the lack of purchasing power remains the main constraints during and after armed conflict [9]. Armed conflict forces people to be displaced from their hometowns to escape intensive violence, migrate, or seek asylum in other countries. The displaced families have less economic means for their health and education and might become a victim of sexual violence, especially women and children [10, 11].
Yemen has gone through multiple armed conflicts, violence and insecurity in the last decades. The recent armed conflict that escalated across Yemen in March 2015 has displaced more than 2 million internally displaced population (IDPs) who left their home governorates of Yemen in search of safety, life, and security. They are living in overcrowded shelters that expose them to the risk of violence, especially among women and children [12]. Moreover, the health system in Yemen was further influenced by the armed conflict, where only 50% of health facilities are fully functional; as well, there is disruption of salaries of most health workers [13]. Access to HIV treatment is critical during an unstable security situation, which may lead to significant logistics and strategic challenges, especially in a fragile health system. The conflict in Kenya, e.g., influenced HIV treatment in different manners, including lowering HIV treatment access and stock-out of ART and other supplies that prevent HIV transmission such as condoms [14, 15]. In addition, conflicts create a state of poverty, thus some poor people will not be able to have access to treatment and become a source of infection to other people [16]. There is also a potential risk of opportunistic infections and interrupted treatment and resultant viral resistance during conflicts among children [17].
The prognosis of HIV disease during humanitarian crises is influenced by several factors such as food insecurity, unclean water supply, a higher rate of infectious diseases, and psychological stress [18]. It is also crucial to make an HIV clinic accessible to PLHIV to ensure optimal adherence to ART that can maintain a Viral Load (VL) level undetectable in the blood and therefore prevent HIV transmission to others [19]. However, stable HIV patients, who have no opportunistic infections and are on ART for at least 6 months with VL less than 1000 copies/ml, have to visit the clinic every 6 months for clinical assessment [20-22]. In addition, the major concern during emergency situations for PLHIV, who are under ART is to secure the ART supply chain. Therefore, it is important for all HIV and Acquired Immune Deficiency Syndrome (AIDS) actors to include HIV emergency response in their emergency plans and encourage the use of national resources [23].
Yemen’s ongoing political and armed conflicts prevent AIDS response and cause challenges toward the scaling up of HIV treatment and care services, which is still limited to five governorates out of 22 governorates, Therefore, this study aimed to assess the implications of internal country conflict on the HIV treatment and care services in Yemen for policy formulation, program planning, and national resource mobilization. It will benefit policymakers in Yemen by providing guidance on increasing the preparedness of the National AIDS Control Program (NAP) and the Ministry of Public Health and Population (MOPHP) during conflicts.
2. MATERIALS AND METHODS
The method of this study has taken three phases to gather data from HIV treatment and care clinics in Al Sadaqa hospital in Aden Governorate and Ibn Sina Hospital in Hadramout Governorate for a better understanding of the research problem and allow complete and synergistic utilization of data.
2.1. Phase I: Analysis of Health Service Data (Secondary Data)
Secondary data was gathered from the HIV treatment and care clinics in Aden and Hadramout. The study population was all PLHIV who enrolled in HIV treatment and care services for the period 2007-to 2015. All PLHIV of both sexes, including children who enrolled in HIV treatment and care services from 2007-to 2015 in both Aden and Hadramout will be included in this analysis. A purposive nonprobability sampling method was applied for health service data as follows:
- 469 PLHIV who enrolled in care in both Aden and Hadramout governorates.
- 346 PLHIV initiated ART in both Aden and Hadramout governorates.
The study was focused on the specific types of indicators needed to conduct the analysis of health service data as follows:
- Percentage of adults and children receiving antiretroviral therapy (ART) among all adults and children living with HIV.
- Percentage of PLHIV known to be on treatment 12 months after initiation of ART.
Health service data was gathered from March to June 2017 and analysed using an Excel sheet and Tier.net software.
2.2. Phase II: Quantitative Data
A cross-sectional design was used to collect primary data on the predictions of PLHIV from Aden and Hadramout HIV clinics to determine whether there is a relationship between different variables. This study did not assess the impact of conflict because the conflict is still ongoing. Furthermore, those under the age of 14 were children, based on the World Health Organization (WHO) classification, who were excluded from the study because they were too young to provide appropriate answers to the study's questions as well as those with mental health problems and non-Arabic-speaking refugees [24].
A systematic random sampling method was applied with a sample of 76 PLHIV required to obtain a 95% confidence interval of +/- 5% around a coverage estimate of 5% in two clinics based on NAP report of 2010 and Country Progress Report of 2014. To allow for an expected dropout rate of 10%, a total of 84 questionnaires were delivered. The formula for estimation of the sample size of a single proportion was taken from the Oxford Handbook of Medical Statistic as follows [25]:
n = 1.962 (p) (1-p)/d2
n = required sample size.
p = expected population proportion. It is the estimated coverage (177 PLHIV were under treatment in Aden and Mukalla sites in 2010 over the estimated number of PLHIV 3400, so the coverage will be 177/3400*100=5%)
d = the desired width of the confidence interval and precision, here is 0.05
n = (1.96)2 * 0.05 * 0.95 / (0.05)2
n = 76 (10% drop-out rate = 76 * 10% = 7.6 rounded to 8)
n = 84
A systematic random sampling method was applied for quantitative studies to select PLHIV based on inclusion and exclusion criteria. The instrument used for the quantitative study was a questionnaire designed as closed-ended questions to collect information from PLHIV. This questionnaire was developed by the researcher based on the variables and data needed to collect. It consisted of three main sections:
1. Demographic data.
2. HIV care data.
3. HIV treatment data.
IBM SPSS Statistics software version 23 was used to analyse the data gathered from a quantitative method. Descriptive statistics cross-tabulation, mean, and standard deviation were used to analyse data. Inferential statistics were used to identify statistically significant differences between variables through multivariate analysis of variance (MANOVA test). This test was used to test the hypothesis and to analyse the effect of one or more independent variables on two or more dependent variables at a level of significance ≤ 0.05.
2.3. Phase III: Qualitative Data
The qualitative research relied on a phenomenological design for a better understanding of the situation that respondents had experienced before and during the conflict. Moreover, this design explains how the HIV treatment and care program operates before and during the internal country conflict. The sampling unit for this study included a representative of adult PLHIV and health care providers (HCPs) who were selected from the health facility providing HIV treatment and care services.
The sample size for the interview was as follows:
- 15 HCPs who are working at HIV treatment and care sites in Aden and Mukalla.
- 20 PLHIV who are enrolled in HIV treatment and care during 2007-2010 in Aden clinic.
A purposive nonprobability sampling method was applied for qualitative studies among PLHIV and HCPs. The tools for qualitative studies were obtained through an open-ended questionnaire. The questionnaire for qualitative data among PLHIV includes five main sections: (1) Access to services before the conflict (2) Service provision and patient satisfaction before the conflict (3) Patient needs (4) Access to services during the conflict (5) Quality of service during the conflict. While the questionnaire for qualitative data among HCPs consists of six main sections: (1) General information (2) Programmatic data (3) HIV treatment & care services (4) Access to services (5) Infrastructure and logistics (6) The challenges.
In-depth and unstructured face-to-face interviews were used in this research to collect qualitative data to identify the participant’s emotions, feelings, and opinions regarding HIV treatment and care services. There was choosing a well-trained and skilled moderator from outside the HIV treatment and care clinic to ensure neutrality and avoid bias. Moreover, triangulation was used by conducting the interview from different clinics and different groups in Aden and Hadramout. In addition, the respondent validation technique was applied by testing the initial results with participants to see if they still rang true.
The qualitative data gathered from personal interviews were transcribed, coded for key themes and subthemes, and analysed manually. The analysis was divided into two main thematic areas and six subthemes covering the research objectives to arrive at, a meaningful explanation of HIV treatment and care services performance before and during the conflict and the gaps in policies and strategies. The qualitative data was gathered for two months, from July-August 2017.
2.4. Inclusion and Exclusion Criteria for Primary Data
2.4.1. A. Inclusion Criteria for PLHIV
1. Males living with HIV >14 years old enrolled in ART during 2007-2010 in Aden clinic.
2. Females living with HIV >14 years old enrolled in ART during 2007-2010 in Aden clinic.
3. PLHIV started ART at another site from 2007 to 2010 and transferred to the Aden clinic.
2.4.2. B. Exclusion criteria for PLHIV
1. Adult PLHIV receiving HIV treatment and care in other clinics.
2. Children living with HIV < 14 years.
3. PLHIV with mental disability.
4. PLHIV with psychiatric problems.
5. Refugees who are not speaking the Arabic Language.
2.5. Research Ethics
The Research Ethics Committee of the University of UKM approved the research with a reference number (UKM PPI/111/8/JEP-2016-614). Research overview and objective information were explained to the respondents and informed consent was taken from all participants in the study. Moreover, the National AIDS Control Program and MOPHP were informed about the purpose of the research.
2.6. Study Limitation
Armed conflict in Yemen prevented carrying out primary data collection in all HIV treatment and care clinics and arranging for interviews with policymakers. The security situation was better in Aden and Mukalla City in Hadramout compared to the previous period and in other governorates. However, the situation is still experiencing bombings, shootings, and incidents involving IEDs and assassination attempts from time to time [26]. Therefore, the movement was risky from one governorate to another and did not guarantee safety. Therefore, the data that is collected from two health facilities in the Aden and Hadramout governorates will be subjected to bias. Moreover, the secondary data presented in this study relied on reports written by the HCPs and underwent information selection and self-reporting bias.
2.7. Conceptual Framework
The conceptual framework developed in this study, as shown in Fig. (1), illustrates the different variables that affect HIV treatment and care services performance in Yemen. Demographic factors and conflict/political instability consider independent variables that influence access to HIV treatment and care services and LTFU and may lead to treatment failure and death as poor outcomes which, in turn, influence the performance of HIV treatment and care programs.

3. RESEARCH RESULTS
3.1. Phase I: Secondary Data Analysis
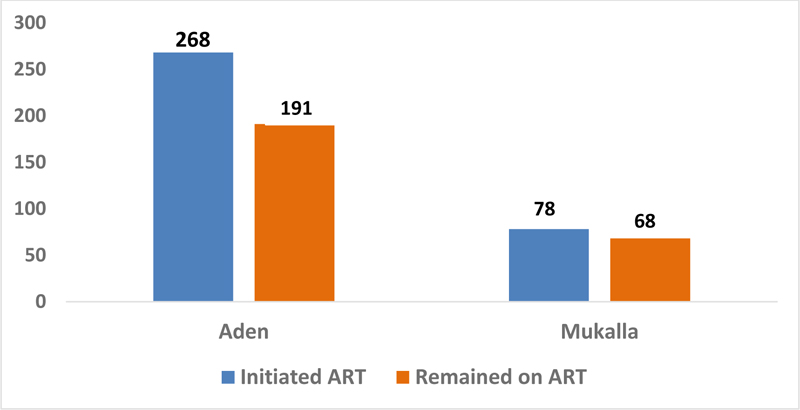
The analysis involved a total of 469 PLHIV who enrolled in care and 346 under ART in both Aden and Hadramout governorates. The highest number was in Aden clinic, which represents 77.5% (268/346) of the total number of PLHIV, while 22.5% (78/346) have seen in Mukalla clinic. There were 191 PLHIV out of 268 (71.3%) in Aden, and 68 PLHIV out of 78 (87.2%) in Mukalla had remained on ART, as shown in Fig. (2).
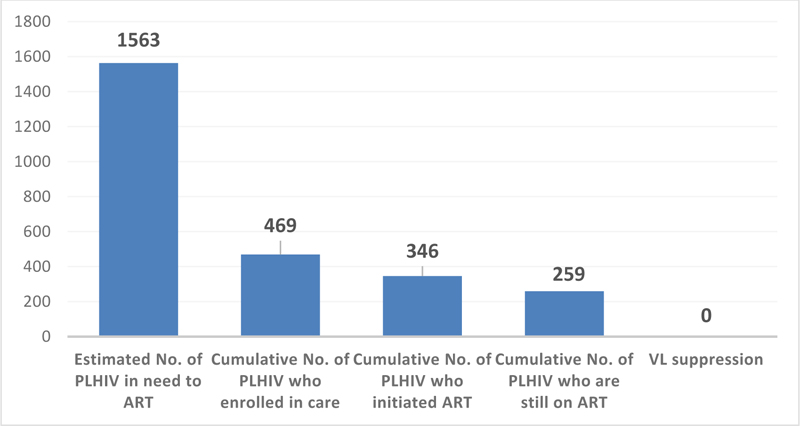
The estimated number of PLHIV in Aden and Hadramout governorates was (1563) based on the NAP/ Joint United Nations Program on HIV and AIDS (UNAIDS) working group using the Spectrum software. The cumulative number of PLHIV who enrolled in care for the duration of 2007-2015 was (469), which represents 30% out of 1563. Only 73.8% (346/469) had initiated ART. The cumulative number of PLHIV who are remaining on ART after the exclusion of LTFU and death cases was (259) out of (346), which represents 74.9%. There was no VL test in Yemen to show viral suppression, as shown in Fig. (3).
The ART coverage in Aden and Hadramout governorates was 16.6% (259/1563) of the estimated number of PLHIV in need of ART. 95.4% (247/259) of PLHIV were adults (>14 years), 4.6% (12/259) were children (<14 years), and male to female ratio was (1.5:1). Death cases represented 14.2% (49/346), and 11.2% (39/346) had a loss to follow for three consecutive months from the start of service in 2007 to 2015.
Patient profiles were characterized by a predominance of men (male: female ratio 1.5:1 (156/103), with a mean age of 36 years and (± 9.1 SD). 85% (294/346) had been infected with HIV via heterosexual contact. Demographic, clinical, and immunological profiles of 346 PLHIV enrolled in HIV treatment programs during the period between 2007 and 2015 in Aden and Mukalla HIV treatment sites are shown in Table 1.
The majority of patients 78.3% (271/346) presented late with clinical stages 3 and 4, and most of them 46.4% (159/346) initiated combination ART at Cluster of differentiation 4 (CD4+ T-cell count 201-350 cells/mm3) as shown in Table 1.
Most regimens included Tenofovir and Efavirenz ART 45.6% (158/346) as shown in Table 2, and TB treatment started for 12.7% (44/346) of them.
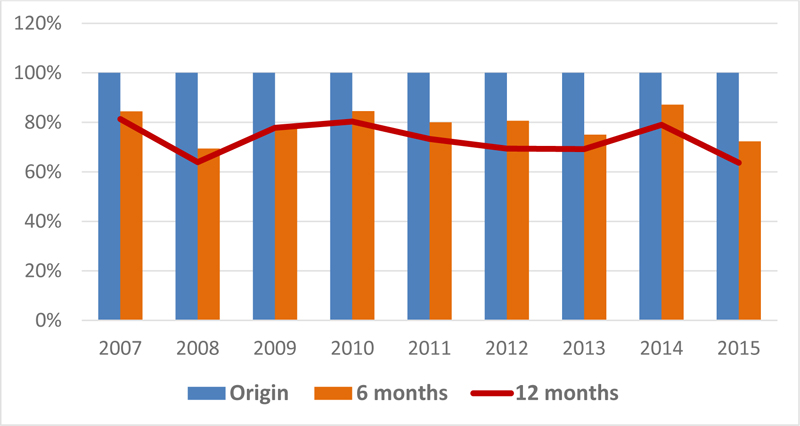
Treatment outcomes of the 346 PLHIV cohorts each year for the period 2007-2015 in Aden and Hadramout displayed the percentage of PLHIV known to be on treatment 12 months after initiation of ART. This cohort analysis showed a fluctuation of the retention curve rate after 12 months of ART initiation around 70% for each year, as shown in Fig. (4). In this figure the first column represents the original cohort that started ART, the second column represents the retention rate of each cohort after six months of ART initiation each year, and the red line shows the retention rate of each year cohort after 12 months after ART initiation.
| Variables | - |
n (Total n = 346) |
% |
|---|---|---|---|
| Age | 0-14 | 19 | 5.5 |
| 15-29 | 92 | 26.6 | |
| 30-39 | 105 | 30.4 | |
| 40-49 | 88 | 25.4 | |
| >49 | 42 | 12.1 | |
| Sex | Males | 246 | 71.1 |
| Females | 100 | 28.9 | |
| Exposure category | Heterosexual | 294 | 85 |
| Homosexual | 21 | 6 | |
| MTCT | 3 | 1 | |
| Blood transfusion | 28 | 8 | |
| CD4+ | ≤ 200 | 128 | 36.7 |
| 201-350 | 159 | 46.4 | |
| > 350 | 59 | 16.9 |
| First-line ART Regimen |
n (Total n = 328) |
% |
|---|---|---|
| Tenofovir (TDF) 300mg /Emtricitabine (FTC) 200mg / Efavirenz (EFV) 600mg | 158 | 45.6 |
| Zidovudine (AZT) 300mg / Lamivudine (3TC) 150mg / Efavirenz (EFV) 600mg | 65 | 18.8 |
| Tenofovir (TDF) 300mg /Emtricitabine (FTC) 200mg / Nevirapine (NVP) 200mg | 11 | 3.2 |
| AZT 300mg/3TC 150mg/NVP 200mg | 100 | 28.9 |
| Abacavir (ABC) 300mg/3TC 150mg/NVP 200mg | 2 | 0.6 |
| ABC 300mg /3TC 150mg/EFV 600mg | 1 | 0.3 |
| Subtotal of PLHIV under 1st line regimens | 337 | 97.4 |
| Second – line ART Regimen | ||
| TDF 300mg/FTC 200mg/ Lopinavir/ritonavir (LPV/r) 400mg/100mg | 3 | 0.9 |
| AZT 300mg/3TC 150mg/LPV/r 400mg/100mg | 5 | 1.4 |
| ABC 300mg/Didanosine (ddI) 400mg/LPV/r 400mg/100mg | 1 | 0.3 |
| Subtotal of PLHIV under 2nd line regimens | 9 | 2.6 |
| Total PLHIV under 1st and 2nd line regimens | 346 | 100 |
There were 10.7% (37/346) of patients presented with HIV-related clinical manifestations after a year of starting ART, which is not related to immune reconstitution syndrome. However, around 2.6% (9/346) switched to second-line ART, as shown in Table 2. 32.4% (112/346) of PLHIV experienced ART substitution within the first-line regimens.
From the start of the HIV treatment and care program till the end of 2015, there has been an increased number of AIDS-related deaths and LTFU. The mean AIDS mortality rate was 13.7%, while the trend fluctuated each year and reached a peak in 2011 and 2012, and the mean LTFU rate was 18.5%. 54 PLHIV out of 346 who did not follow-up since the start of HIV treatment and care services in 2007 to 2015 were 81.5% (44/54) Yemenis, 64.8% (35/54) females, 50% (27/54) married and 51.9% (28/54) among the age group 25-49 years. The years 2011 and 2012 showed the highest rate of loss to follow-up in the cohort analysis of 2007-2015, which declined in 2013 and 2014 and rose again in 2015.
3.2. Phase II: Quantitative Results
The analysis involved 84 questionnaires of interviewed PLHIV during the study period with a response rate of 100%.
The mean age of the respondents was 40.5 (±10.6 SD) a year, and the highest percentages were 35.7% (30/84) and 29.8% (25/84) among the age groups 30-39 years and 40-49 years, respectively. While there are no PLHIV among the age group 0-14 years, who meet the inclusion criteria of being enrolled in ART at HIV treatment and care sites in Aden or Mukalla or at other sites from 2007 to 2010 at the time of the interview. There were 64.3% (54/84) of PLHIV males, while females represented 35.7% (30/84).
42.9% (36/84) of PLHIV interviewed were married, 25.0% were single, 23.8% were widowed, and 8.3% were divorced. 57.1% of PLHIV partners had HIV, and 15.4% had HIV-infected children.
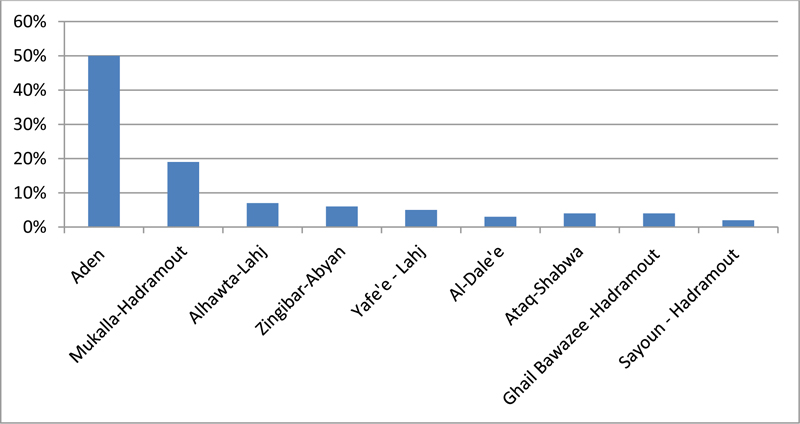
There were 50.0% (42/84) of PLHIV living in Aden governorate, 19.0% in Mukalla city of Hadramout governorate, and the remaining PLHIV were from neighbourhood governorates and districts with no HIV treatment and care services as shown in Fig. (5).
34.5% (29/84) of PLHIV had secondary education, 29.8% had primary education, 23.8% were illiterate or at least could write and read, and 11.9% had academic education.
56% (47/84) of PLHIV were unemployed, 22.6% (19/84) were working with the Government, while 21.4% (18/84) were working in the private sector.
98.8% (83/84) of PLHIV were Yemeni and 1.2% were non-Yemeni (Somali Nationality).
There is a gap between HIV diagnosis, enrolment in HIV care, and initiation of ART each year. There were 46.5% (39/84) of PLHIV who had been diagnosed before and in 2007, 33.3% (28/84) enrolled in care in 2007, and only 19% (16/84) of them initiated ART. Meanwhile, in 2008-2009, fewer people were diagnosed with HIV positive, enrolled in HIV care, and initiated ART. However, in 2010 most PLHIV (44.1%) had initiated ART, although there was low access to HIV diagnosis and care services in the same year where only (21.4%) of them were diagnosed HIV positive and (27.4%) could access and enrol in HIV care services as illustrated in the Table 3.
The first clinic visit is to identify which stage where PLHIV is located and whether they are in need to initiate ART or not. Where the follow-up visits bring out information on PLHIV condition for those who have still not initiated ART and came for clinical and para-clinical assessment and those on ART. There are four CLINICAL stages that categorize HIV disease severity, and it ranges from mild symptoms (stage 1) to severe symptoms (stage 4). This research showed that 84.5% (71/84) of PLHIV had more than one sign and symptom at the first visit to the clinic in Aden governorate and Mukalla City of Hadramout governorate, and 15.5% (13/84) of PLHIV had no signs and symptoms as shown in Table 4.
| Year | Diagnosis | Enrolment in Care | ART Start | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Before and 2007 | 39 | 46.5 | 28 | 33.3 | 16 | 19.0 |
| 2008 | 7 | 8.3 | 12 | 14.3 | 16 | 19.0 |
| 2009 | 20 | 23.8 | 21 | 25.0 | 15 | 17.9 |
| 2010 | 18 | 21.4 | 23 | 27.4 | 37 | 44.1 |
| Total | 84 | 100 | 84 | 100 | 84 | 100 |
| Signs and Symptoms | N | % |
|---|---|---|
| Weight loss | 54 | 64.3 |
| Fever | 37 | 44 |
| Diarrhoea | 37 | 44 |
| Cough/chest infection | 21 | 25 |
| Oral Candidiasis | 18 | 21.4 |
| Lymphadenopathy | 12 | 14.3 |
| Papular pruritic eruptions | 11 | 13.1 |
| Oral ulceration | 10 | 11.9 |
| Dizziness | 10 | 11.9 |
| Amnesia | 5 | 6 |
HIV and TB coinfection represented 9.5% (8/84) for pulmonary TB and 2.4% (2/84) for extrapulmonary TB. While there were no HIV and hepatitis B or C co-infection among interviewed PLHIV.
Early presentation at the clinic for PLHIV who are still at stage one or two means better health outcomes. Most PLHIV had presented late at the clinic with clinical stages 3 and 4 (45.7% and 36.6%, respectively), while 7% had presented at clinical stage 1 and 10.5% at clinical stage 2.
There were 63 PLHIV out of 84 who had got married. Most couples went through HIV tests if one of them is HIV positive. 60.3% (41/63) of PLHIV partners knew the HIV status of their couple. Out of those who tested for HIV, 57.1% (36/63) were HIV positive, and 60.3% (38/84) of them knew their own HIV status.
Not all married, divorced, and widow PLHIV have children, only 48 PLHIV out of 63 (76.2%) had children, and not all PLHIV did HIV test for their children. Only 81.3% (39/48) of their children were tested for HIV, and 15.4% (6/39) were HIV positive and received ART. While 41.3% (26/63) of PLHIV children died either at birth or after birth for unknown reasons.
98.6% (70/71) of PLHIV presented for the first time at the clinic with clinical signs and symptoms improved during the 6 months after ART initiation, while 1.4% (1/71) did not improve. Though, 21.8% (15/71) of PLHIV had got recurrent signs and symptoms after 6 months of ART initiation, while 78.2% (56/71) had no recurrent signs and symptoms.
HIV treatment and care clinics of Aden and Mukalla cover most neighbouring governorates that have PLHIV under ART. Not all PLHIV could access services based on their clinic appointment. 56% (47/84) of PLHIV could access HIV treatment and care services once during the armed conflict, 22.6% (19/84) twice, 10.7% (9/84) three times, and 10.7% (9/84) more than 3 times.
The frequency of access to the Mukalla HIV treatment and care clinic from Mukalla city, Ghail, Bawazeer, and Sayoun districts of Hadramout governorate was three times more during the armed conflict compared to the frequency of access to HIV treatment services by PLHIV from neighbouring governorates such as Shabwa. Moreover, there was low access to the Aden HIV treatment and care clinic in Aden itself and neighbouring governorates or districts such as Lahj, Yafe’e, and Al-Dhale’e where the frequency of access was less than three times. The Pearson Chi-Square test showed a significant level of P-value (p=0.000).
The Multivariate Test is the actual result of the one-way MANOVA which tested residence as an independent variable with four dependent variables related to the frequency of access to HIV treatment and care services during the internal country conflict as follows: 1) access to services once, 2) access to services twice, 3) access to services three times and 4) access to services more than three times. The effect labelled “Residence” and the Wilks' Lambda row showed a “significant value of (0.000)”, which means p < 0.0005. Therefore, the frequency of access to HIV treatment and care services during the conflict significantly depends on the residence of PLHIV.
Residence of respondents has a statistically significant effect on access to HIV treatment and care services during conflict (p < 0.0005) and (95% confidence interval (CI): 2.48 to 1.22) for Aden and Mukalla, (95% CI: 0.84 to 3.09) for Aden and Lahj and Abyan, and (95% CI: 0.69 to 3.14) for Aden and Yafe’e. It is also statistically significant with (p ≤ 0.002) and (95% CI: 0.45 to 3.22) for Aden, Dhale’e, and Shabwa.
Multivariate Test shows the effect of the availability of the clinic as an independent variable with four frequencies of access to services as dependent variables (once, twice, three times, and more than three times). The Wilks' Lambda row showed a “significant value of (0.000)”, which means p < 0.0005. Therefore, the frequency of access to HIV treatment and care services during the internal country conflict was significantly dependent on the availability of the clinic (p < 0.0005) and with (95% CI: 1.007 to 1.953).
There were 41.7% (35/84) of PLHIV who had been interviewed had LTFU since the start of ART, 51.4% (18/35) of them had lost once, 28.6% (10/35) twice, and 20% (7/35) three times. The drop-out rate was 11.4% (4/35) of those who LTFU for three consecutive months (90 days) during the follow-up period.
There were 40% (14/35) of the interviewed PLHIV LTFU in the same year of ART start, 37.1% (13/35) of them had lost after three years of ART start, and 22.9% (8/35) of them within the first three years. There were 71.4% (25/35) of interviewed PLHIV with LTFU had received a phone call from health care providers at HIV treatment and care clinic as part of the tracking system. While 28.6% (10/35) did not receive any phone call from health care providers who are working at the treatment clinic. 60.0% (15/25) of them had received a phone call from their doctor and 40.0% (10/25) from nurses. There were 68.0% (16/25) of the respondents had received a phone call just once since the start of ART, 28.0% (7/25) of them had received phone calls twice and 12.0% (3/25) of them had received phone calls three times.
The main reasons for LTFU that have been given by 35 respondents were internal country conflicts (25.7%), stigma and discrimination at home (17.1%), the location of health facilities far from PLHIV residency either in a different governorate (17.1%) or in a different district (14.3%), stigma and discrimination at health setting (11.4%), no money for transportation (11.4%) and the closure of HIV treatment and care clinics (2.8%) as shown in Fig. (6).
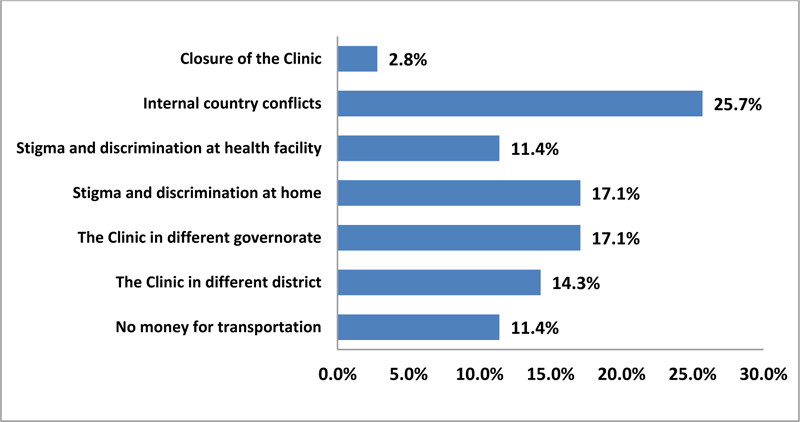
Table 5 provides the mean and standard deviation for the duration of LTFU, which has been split by occupation. In addition, the table provides “Total” rows, which allows means and standard deviations for groups split by the experience of LTFU to be known.
| Dependent Variable | Independent Variable (Occupation) | Mean duration | Std. Deviation | n | |
|---|---|---|---|---|---|
| Have you experienced loss to follow-up? | Work - Government | 1.74 | 0.452 | 19 | |
| Work - Private | 1.28 | 0.461 | 18 | ||
| Not work - Unemployed | 1.64 | 0.486 | 47 | ||
| Total | 1.58 | 0.496 | 84 | ||
The occupation of respondents has a statistically significant effect on LTFU (p = 0.011) and (95% confidence interval (CI): 0.09 to 0.83) for work with the Government and for work in the private sector as shown in Table 6.
| Dependent Variable | Independent Variable (Occupation) | Mean Difference (I-J) | Std. Error | Sig. | 95% Confidence Interval | ||
|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||
| Have you experienced loss to follow-up? | Work - Government | Work - Private | 0.46* | 0.156 | 0.011 | 0.09 | 0.83 |
The Multivariate Test is where the actual result of the one-way MANOVA. The second effect labelled “Occupation” as an independent variable and its relation with the frequencies of LTFU either once, twice, or three times as dependent variables. The Wilks' Lambda row showed a “significant value of (0.033), which means p < 0.05. Therefore, LTFU was significantly dependent on the occupation of PLHIV.
During the conflict, 66.6% (56/84) of PLHIV who were interviewed experienced a change in ART regimen per lifetime. There were 55.3% (31/56) of them had experienced ART change once, 28.6% (16/56) twice, and 16.1% (9/56) three times. Moreover, 50% (3/6) of the respondents whose children are under ART had experienced a change in ART regimen for their children.
96.4% (54/56) of interviewed PLHIV who are experiencing a change in ART regimen know the reasons behind this change. There were 81.5% (44/54) of them gave ARV stockout as the main reason for the change in ART regimen, while 27.8% (15/54) and 5.6% (3/54) of them gave the reasons for drug side effects and drug resistance, respectively. In addition, 33.3% (2/6) have mentioned the main reason for the change in ART regimen for their children was also stockout of ARVs during the conflict.
During the interview with PLHIV, 47.6% (40/84) of PLHIV experienced the closure of the HIV treatment and care clinic in Aden governorate during the armed conflict in 2015. There were 67.5% (27/40) of them had faced the closure of the site once, 20.0% (8/40) twice, 7.5% (3/40) three times, and 5.0% (2/40) more than three. All PLHIV who faced the closure of the HIV treatment and care site had given the insecurity situation as the main reason for the closure.
3.3. Phase III: Qualitative Results
The response obtained from in-depth interviews was analysed under main two themes which were the performance of HIV treatment and care services and HIV treatment and care policies and strategies.
3.3.1. Performance of HIV Treatment and Care Services
The analysis of this theme was obtained from in-depth interviews with 20 PLHIV who explained that before the armed conflict, the frequency of access to HIV treatment and care services was monthly at the beginning of ART initiation and every 3 to 4 months. Almost all interviewed PLHIV spent between YER 500 - 1000 (MR 8.12-16.24) per visit to access HIV treatment and care services. Eleven PLHIV were not comfortable with this cost. Also, all interviewed PLHIV agreed that, there was no extra cost to access services. However, some of them heard about the blackmail of some patients by some staff. Nineteen PLHIV are getting HIV treatment and care services for free except for lab tests such as liver function tests (LFT) and renal function test (RFT), which they have to do it in private health facilities. Eleven PLHIV were not convinced with the HIV treatment and care services provided before the conflict, they agreed upon the absence of clinical examination at HIV treatment and care clinic, lack of important tests such as CD4+ cell count/mm3, Complete Blood Count (CBC), LFT and RFT. Eight PLHIV had experienced a long waiting time at the clinic and eleven PLHIV expressed a good doctor-patient relationship, but one of them (PLHIV 2) said; “it is acceptable, but if I don't go to the clinic, no one is looking after me”.
Three PLHIV experienced ARVs disruption before the conflict because of shortages in some ARVs, and they mentioned the same phrase; “The cause of treatment disruption was due to lack of ARVs, the doctor changed the treatment regimen”.
Most PLHIV get ART for 3 months, while others get it either on a monthly basis, especially for those living near the clinic, or every 6 months for those living away. Seventeen PLHIV go to the clinic regularly on the schedule, while the remaining have missed their appointments. One of them (PLHIV 15) said; “I stopped going to the clinic for the last 3 years, but I am adherent to ART”.
The delay in ARVs supply led to complaints of nine PLHIV who experienced a three times changes in ART regimens. Eleven PLHIV had had blood tests for CD4+ count/mm3, CBC, LFT, and RFT regularly at the beginning of ART initiation and before the conflict. Five PLHIV have done blood tests at once, while four of the PLHIV have never done or even no one requests for them any blood tests.
There is no psychological support provided to PLHIV at the clinic. Seven PLHIV faced psychological problems, stigma, and discrimination. One of them (PLHIV 11) said; “I and my family were shocked when I knew my HIV status, my life has been destroyed and I failed to organize my life and my children's life, especially after the death of my husband due to AIDS”.
Seventeen PLHIV said that the government is not ready to accommodate the needs of PLHIV. All of them stated that although there is a specific law for PLHIV, the government is not ready to provide support. Fourteen PLHIV are requesting the Government to expand HIV treatment and care services to all districts/governorates' health facilities to make ART more easily accessible. One of them (PLHIV 8) said; “The Government should procure treatment from a domestic fund for sustainability because the donors might stop supporting us at any time”.
Since the start of the conflict, nineteen PLHIV have had difficult living conditions. They complain of low economic status and unstable security situations that can hinder their access to treatment. They also fear a lack of treatment, food insecurity, and lack of electricity and water. There were three PLHIV who indicated that their homes had been destroyed during the war. Eight PLHIV had been displaced once since the time of the conflict, three PLHIV had been displaced twice, and another three displaced more than twice. While some of them did not move out of their homes. There was a problem that hindered PLHIV from accessing HIV treatment and care services during conflict. Twelve of them said the same phrase; “The main problem we faced during the armed conflict was access to treatment due to insecurity, far distance to HIV treatment clinic, and displacement”.
Eight PLHIV complained of lack of financial support, six of them had difficult access to nutrition, and two PLHIV complained of stigma. Nineteen PLHIV have never been treated differently during the conflict by health care providers, but the clinic was closed for 6 months during the armed conflict, and they received the ART from the doctor’s house.
Eighteen of them had experienced out-of-pocket money to get access to services during the armed conflict because all public transportation stopped working and they paid for private transportation around YER 10000 (MR 162.35). Thirteen PLHIV were uncomfortable with the quality of services provided during the conflict because of difficulties to access services. Seventeen PLHIV did not experience ART disruption during the conflict, while three of them have had treatment disruption for 3 days. One of them said; “The pharmacist gave me half of the amount that supposed to receive due to the stock out of medicines”. (PLHIV 13).
Eighteen PLHIV did not experience a change in ART regimen during the conflict, while two of them had been exposed to changes in ART regimen twice due to the stockout of medicine. Seventeen PLHIV said that they had never taken blood tests during the conflict, while three PLHIV had taken CBC, RFT, and LFT. Six PLHIV also indicated that they knew a person living with HIV who died during the conflict because of their displacement and inability to access ART. And six PLHIV also indicated that they knew a person living with HIV who died during the conflict because of their displacement and inability to access ART. And one of them (PLHIV 6) said that a Somali refugee woman was pregnant and had been badly treated by hospital healthcare providers and eventually died.
All interviewed PLHIV are requesting the government to continue supporting the provision of ARVs, other medicines, and lab tests, including CD4+ cell count/mm3 and Polymerase Chain Reaction (PCR) for free. They are also looking for job opportunities, financial support, or migration to be able to live and cover school expenses for their children. They are also looking to continue raising awareness, training for the PLHIV support group and supporting their existence at the HIV treatment and care clinic to be able to provide peer support that can help to improve adherence to ART.
3.3.2. HIV Treatment and Care Policies and Strategies
The analysis of this theme was obtained from in-depth interviews with 15 HCPs. All respondents indicated that the HIV treatment and care program in Yemen is supported by the Global Fund to Fight AIDS, TB, and Malaria. They added the same phrase; “The technical support is provided by the WHO and NAP-MOPHP”. Twelve HCPs gave the benefit of joining the HIV treatment program to provide services and support to PLHIV, while three of them have indicated that they joined the HIV treatment program to improve their income due to the incentives that they receive.
Thirteen HCPs explained that NAP, Global Funds, UN Organizations, MSF and hospitals where HIV treatment clinics exist are providing support for service provision. Some of them (HCP 4) said; “The Global Fund is responsible for ARVs supply to all targeted health facilities since 2007”.
All HCPs said that they have no written action plans for HIV treatment and care program at their health facility. Twelve HCPs have confirmed that there were activities supporting the HIV treatment program before the conflict. They said the same phrase; “Most of the HCPs participated in capacity building and awareness-raising of other HCPs at the governorate level and neighbouring governorates, the printing of educational materials such as brochures and posters, home visits to provide counselling some PLHIV in a confidential way, participation in ART committee meetings”.
ARVs are supplied through the NAP, and the drugs are distributed through public transportation. All HCPs said the same phrase; “They obtained pre-conflict ARV supplies through the NAP Supply Management Unit. Medicines are sent via public transportation (bus or taxi) or sometimes through NAP teams during their supervision visits to all HIV treatment sites”.
Eight HCPs have reached patients before conflict by referral from governmental and private hospitals or clinics, other HIV treatment and care sites, Voluntary Counselling and Testing (VCT) sites, and prevention of mother-to-child transmission (PMTCT) sites. While three HCPs indicated that some PLHIV comes by themselves. Most of the challenges faced by the seven HCPs prior to the conflict were delays in the release of the operational budget and staff incentives. One of them (HCP 3) said; “Discontinuation of monthly meetings, lack of regular provision of stationery and cleaning materials, and delayed monthly incentives were considered the main challenges in the period preceding the conflict”. HCP-5 said; “Stigma, discrimination, and distance from HIV treatment sites was considered the main challenges before the conflict “.
The main problems and challenges that faced eight HCPs during the armed conflict in Aden were an inability to access HIV treatment and care clinics. The clinic was closed and had been exposed to a robbery of most of the electronic and electrical equipment. It became a residential place for the IDPs. Some of the HCP said; “There is an increased number of LTFU during the armed conflict, and there is incomplete data in the patient’s files which has influenced our daily job of writing monthly reports”.
Insecurity situation prevented HCPs in Aden from accessing the clinic during the conflict. All HCPs in Aden said the same phrase; “A shortage of stocks of ARVs, high transportation costs due to increased fuel costs, and a lack of an operating budget remained the main problems during the conflict”. In addition, two HCPs indicated that the incentive that they receive from the NAP is low compared with the risk, there is no hazard pay and no training courses that can help to improve the knowledge and skills of HCPs”. One of HCPs (HCPs 11) said; “Some HCPs refuse to deal with PLHIV, especially surgical doctors in government and private health facilities, and there is a lack of government support to procure HIV treatment”. Another one (HCP 3) said; “There is no oversight, monitoring and evaluation by the hospital management to improve staff performance”.
All HCPs had agreed to make PLHIV and their problems more understandable to the Government by requesting a meeting with the government to discuss the problems that PLHIV has complained about. Some of the HCPs indicated that; “The MOPHP and NAP should advocate the Government to mobilize national resources to ensure the sustainability of ARVs, support, and expand HIV treatment and care sites to other governorates”.
Nine HCPs said that life has changed during the conflict where insecurity, rising prices, no salaries, scarcity of resources, scarcity of fuel, and increased transportation costs were the most prominent problems in the community. All interviewed HCPs said that the most powerful memory about working as a health care provider in the pre-conflict period is that there were no significant challenges that can prevent the provision of services. One of them (HCP 4) said; “During the conflict, I was afraid of treatment interruption, all activities collapsed, and there was low access to treatment and care services by PLHIV”.
There was no emergency plan at the level of HIV treatment and care clinic in Aden, while in Mukalla has developed an emergency plan for rationing of ARVs. ARVs were available at the level of HIV treatment and care clinics before the conflict. However, nine HCPs have experienced a shortage of ARVs before the conflict. There are no big problems regarding reaching PLHIV before and during the start of the conflict in February 2011 compared with 2015 as HCPs in Aden said. One HCPs (HCP 6) said; “I faced big challenges during the start of the armed conflict in 2015 in Aden, the PLHIV had been reached by phone calls or social media to inform them to take their ARVs to the doctor's house”. And HCP-10 said; “I received a big number of PLHIV in Mukalla who were referred from other HIV treatment sites due to internal displacement”.
All HCPs confirmed that there are no alternative clinics or warehouses for ARVs and other Opportunistic Infection drugs (OIs) during the conflict. The Coordinator of Aden HIV treatment and care site (HCP 1) said, “There are no alternative warehouses, but I used my house as an urgent solution to dispensing ARVs”.
The HCPs in Aden complained of the bad security situation during the armed conflict in Aden. All interviewed HCPs in Aden and Mukalla confirmed that the laboratory was not working for more than 3 years in Aden and had never worked in Mukalla. The lab technician in Aden (HCP 6) said, “There was a shortage of CD4+ reagents in Aden, and the CD4+ machine has stopped working”. While HCP-13 said, “The CD4+ machine has never worked in Mukalla since we received it in 2011 due to a technical problem”.
All HCPs indicated that the PCR machines have been received since 2014 but did not work due to technical reasons in installation. Furthermore, all HCPs said that there is a shortage in stationery due to stop disbursement of the operational budget since 2015.
All HCPs at HIV treatment and care clinics in Aden agreed that there was declining in the number of new PLHIV who accessed services during the conflict compared to pre-conflict period because no private clinics, hospitals, labs and staff worked during the armed conflict. Moreover, they said that there were no reagents for HIV diagnosis.
The culture in Yemen influences the access of women to health services. All HCPs in both HIV treatment and care clinics (Aden and Mukalla) said the same phrase, “Men have more access to services than women in the pre-and during conflict time”.
There has been loss to follow-up since the start of HIV treatment and care services, but it increased during the armed conflict in Aden in 2015. Some PLHIV who lost follow-up return to the clinic and restarted ART again after receiving counselling. All HCPs have experienced changes in the treatment regimen for PLHIV more than twice due either to the side effects of medicines, stock out of ARVs, or treatment failure, especially during the conflict period.
In Mukalla, all HCPs indicated that there was no destruction or theft of health facilities, but the air conditioner and computer were damaged during the period of the armed conflict, and we do not have an operating budget to fix them. While eight HCPs in Aden said that the treatment site was robbed. HCP-1 said that, “The health facility was not destroyed in 2015, but the HIV clinic has been stolen, where the fans, computers, air-conditioning, and printer were stolen. Moreover, the IDP stormed the clinic during armed conflict”.
4. DISCUSSION
AIDS is one of the biggest public health challenges because of socio-cultural barriers that prevent PLHIV from accessing services. These challenges include the need to expand HIV treatment and care services, especially in low-income countries with a concentrated HIV epidemic [27]. Thus, the public health approach focuses on combination prevention strategies with early initiation of ART and achieving long-term retention in care and viral suppression to end the HIV epidemic by 2030 [28]. The socio-demographic characteristic of PLHIV in this study is similar to that reported by some countries where they are male dominant, and the mean age is around 40.5 years. This may be because of socio-cultural factors that allow males and young adults to access HIV services more than women [29]. There is a relationship between higher education and the unemployment rate, although most highly educated people do not find opportunities in the current work market. However, those who have a low-educated level have less chance of having jobs [30]. The majority of PLHIV who accessed HIV treatment services, as shown in this study, have secondary education, similar to Kenya where 70% of PLHIV reported in a socio-demographic study [31]. Also, HIV-related stigma prevents HCPs from engaging in HIV treatment and care programs, especially for females, as shown in this study. This may influence women living with HIV to access HIV services and seek medical advice in a community such as Yemen [29].
This study showed a gap between HIV diagnosis and enrolment in HIV care in Yemen. This might be related to delays in launching HIV treatment and care programs, stigma, and limited HIV care services to only 5 main governorates out of 22. The PLHIV in New York City has reached suboptimal outcomes in the care continuum. Although 72%-80% of PLHIV have been promptly linked to care after their HIV diagnosis, only 45%-59% maintained care and 24%-43% of PLHIV attained got viral load suppression. The reasons behind this underutilization of HIV care services and suboptimal clinical outcomes are related to, for instance, young age, low income, lack of signs and symptoms, and stigma. Place of residence is also playing a role in the utilization of HIV services, where those who are living far from services have a low level of utilization of services and poor clinical outcomes [32, 33]. The long waiting time preceding the treatment period with a CD4+ cell count/mm3 decline affects subsequent ART adherence, HIV- related mortality, and immune response. Therefore, PLHIV may continue their risky behavioural pattern, which accelerates HIV disease progression [34]. It is also noticed in Tanzania that PLHIV who were linked to HIV care services within the first 6 months of testing HIV positive were those who had a facility-based HIV test compared with those who tested outside the health facility [35].
There are different factors influencing the health-seeking behaviour of PLHIV in Yemen. Most of them present late with clinical signs and symptoms of stages 3 and 4. Late presentation at the first clinic visit was explained in different studies where it remains a problem in high-income countries such as the United States of America and Europe. That means PLHIV either comes with a very low CD4+ cell count (< 100 cells/mm3) or with a clinical stage 4, irrespective of CD4+ counts. This has a negative impact on the health system where the costs are increased, and HIV transmission and mortality are also increased. Furthermore, there are many PLHIV who are referred from a VCT to an HIV treatment and care site; those seem to enrol in HIV care earlier, while elderly patients have a later presentation, as explained in the study conducted in Cambodia [36]. Most PLHIV in Sub-Saharan Africa present at the clinic at late stages which results in early mortality even after ART initiation, and slow response of CD4+ cell count [37]. Similarly noticed in the Mozambique cohort study where clinical stages 3 and 4 represented the highest percentage [38]. There is a significant association between a CD4+ cell count/mm3 at baseline and an immune outcome; a late initiation of ART with low CD4+ cell count/mm3 at baseline leads to poor immune recovery [39].
TB and HIV comorbidity is considered one of the serious worldwide public health challenges, especially in the European region. HIV infection increases the risk of reactivation of latent TB, and TB has an adverse effect on PLHIV where the disease increases viral replication [40, 41]. South Africa has a high load of HIV/TB co-infection where 61% of TB cases in 2014 have HIV [42]. In Kenya, TB/HIV represented (3.4%) of cases [43], and most European countries reported (7.9%) of TB/HIV co-infection [41]. Although the estimated number of TB cases per year in Yemen is 14,000, the study among TB patients that was conducted in 2009 showed the prevalence of HIV among TB patients (1.75%) [44]. However, this analysis pointed out that TB-HIV co-infection was shown at the first clinic visit in Yemen where TB treatment started for only (5%) of PLHIV with a proven TB diagnosis.
This study indicates that most HIV couples who participated in this study went through HIV testing, and most of them know the HIV status of their partner, but not all partners know their HIV status, which may delay linkage to HIV care and ART initiation. Moreover, not all PLHIV have linked their children to care, although most of them who have children did an HIV test for them. Sweden has achieved a 73% level of undetectable viral load, although some PLHIV is still not aware of their HIV status in some European countries, which may delay receiving care and treatment and might not achieve viral suppression [45].
The frequency of clinic visits has pros and cons on the cost and efficiency of the HIV treatment and care clinic. Increasing the frequency of visits can lead to an increase in the burden on the patient to pay extra costs for transportation, have a long waiting time at the clinic due to the increasing burden of patients and reduce the time given for the patient to receive proper care and counselling. On the other hand, the patient will get proper follow-up and on time and early discovery of treatment failure. While decreasing the frequency of clinic visits can decrease the burden on patients, and the patient can receive more attention from the HCPs but could miss some early warning indicators for treatment failure. Therefore, some countries have taken this into consideration and implemented a task-shifting to the community in providing HIV care and reducing clinic visits such Kenya [46]. Prior to the conflict, there were different factors influencing access to the HIV clinic in Yemen such as stigma and discrimination in health settings [18]. This study has explored regular access to HIV treatment and care services by PLHIV in Yemen in the period with precedent conflict either on a monthly basis or every 3-6 months for stable cases. This frequent visit to the HIV clinic does not depend on health-seeking behaviour, rather it depends on clinical actions and national policies and guidelines. Therefore, most PLHIV have spent out-of-pocket money to pay the transportation cost. Similarly, in Uganda, 90% of PLHIV who have a stable condition have to visit the clinic every 3 months [46]. However, there were different factors influencing access to HIV treatment and care services in Yemen, such as stigma and discrimination in health settings prior to the conflict and limited number of HIV treatment and care clinics [18]. Low access to HIV treatment has worsened during the armed conflict in Yemen, as indicated in this study. This is also seen during the conflict in northern Uganda for PLHIV who are from remote and rural areas. Conflict has also influenced the availability of ART [47]. 71% of PLHIV had treatment interruption during the conflict in Kenya [18]. Furthermore, the availability of the clinic plays a role in access to services. During the armed conflict in Yemen, the HIV treatment and care clinic in Aden was closed and most of the PLHIV could not access services and received treatment at the doctor’s house. Similarly, the closure of the clinic during the armed conflict in Burundi and Uganda influenced mothers' access to health services and resulted in increased maternal death [48].
There is a relationship between conflict and shortage of funds. The political instability in Guinea-Bissau influenced AIDS response, where all HIV services collapsed because of cuts in funds [49]. Also, the conflicts in the Central African Republic, which depends mainly on donors’ support for AIDS response, led to shortages in ARVs, high rates of LTFU, and poor treatment outcomes. On the other hand, most of the conflict-affected countries that have concentrated HIV epidemic among FSWs and MSM had complained of increasing morbidity and mortality related to HIV and AIDS although of increased spending on HIV [50]. Similarly, this study explained fund shortages during internal country conflict compared to the period preceding conflict. Most HIV treatment program support activities such as capacity building of HCPs, the printing of educational materials, raising awareness activities, regular supervision visits, and staff meetings were stopped during the conflict. Moreover, the scaling-up plans of HIV treatment and care clinics were frozen because no funds supported their implementation. Furthermore, the study showed shortages in HIV-specific tests such as CD4+ cell count/mm3 and VL.
Each year there are hundreds of millions of people affected by humanitarian emergencies where most of the people are displaced and lack access to essential health services including HIV services. In 2013, there were 1.6 million PLHIV affected by humanitarian emergencies worldwide, and 81% of them lived in sub-Saharan Africa [51]. There is a negative effect of emergencies on health services, including HIV treatment and care. For instance, there was an 88% drop in the number of HCPs due to armed conflict that led to a million displacements in Coˆte d’Ivoire. The violence in Kenya during the post-election period led to ART disruption for more than two days in one hospital in Nairobi. The effect of floods in Mozambique caused the closure of the clinics and treatment interruption [52]. Furthermore, in conflict-affected countries, health services are exposed to danger and the quality of services becomes low due to the fragile health system and the absence of national health policies [53]. The blockade that occurs as a result of conflict has influenced the shipping of medicines and transportation to HIV treatment sites so that it can affect the quality of services provided [54].
This study has shown significant levels of LTFU in the pre-ART and ART periods because of the statistically significant between LTFU and work either in the government or private sector. However, most of the LTFU was in 2011 and 2012; this might be due to insecurity and unstable political and economic situations in the country where Yemen was among the countries involved in the Arab Spring revolutions [55]. The study also reported that married and unmarried young males have a higher number of LTFU. Similarly, the civil war in South Sudan affected HIV care services and led to an increased number of LTFU among PLHIV [56]. It is also noticed that LTFU frequently occurred among PLHIV who had a shorter history of HIV infection, and this might be due to improper counselling being given to the PLHIV at the start of ART and during each visit [57].
Using a combination ART regimen can lead to a dramatic response in controlling the burden of HIV. However, there are many reasons that force PLHIV to undergo treatment substitution within the first line or switching to second-line regimens, such as intolerance to a specific drug, drug side effects, drug interaction, or treatment failure [58]. In Cameron, 73.8% of PLHIV have experienced changing ART regimens, and 90% of them were given the cause of a shortage in ART stock [59]. Among the 3028 PLHIV who switched to second-line ART regimens in South Africa, 11.7% and 8.6% of them were because of treatment substitution and treatment interruption, respectively [60]. Similarly, in Yemen, PLHIV were exposed to multiple ART changes before and during conflict due to healthcare supply factors and patient factors such as lack of a national supply policy on ARVs and drug toxicity, respectively.
Nutrition is a critical component of HIV treatment, care, and support although the availability of ART. The immune system of PLHIV may further weaken due to malnutrition and can expose them to opportunistic infections. The evidence confirms that most undernourished PLHIV are likely to die 2-6 times when starting ART compared with those who have a normal body mass index [61]. There is no clear policy or strategy to include PLHIV support within the existing humanitarian plan. Most PLHIV in Yemen is not targeted for food support, although they are most in need. They are chronically ill, have no productive assets or reliable means of income, and are marginalized in the community due to stigma and discrimination. Furthermore, the conflict forced people to move from their hometown to the safest places [62]. This study showed that 70% of PLHIV had been displaced internally during 2015, and it is expected more displacement due to continued armed conflict. Therefore, PLHIV are at high risk of getting acute watery diarrhoea, meanwhile, they do not have enough food, which can worsen their medical condition.
CONCLUSION
This study assessed the implications of internal country conflict on HIV treatment and care services in Yemen through a mixed method of quantitative and qualitative studies besides the analysis of secondary data. Most of the respondents were PLHIV among the young age group, males, married, and jobless because of having low education levels. This influenced the access of PLHIV to HIV treatment and care clinics, especially for those who are outside the governorate where the clinic exists because of the inability to afford the transportation cost, especially during the internal country conflict. This study also reveals that the HIV treatment and care sites in Yemen are limited to only 5 governorates out of 22, which makes access to HIV treatment and care services very difficult, especially for PLHIV who are living in remote areas despite a stable security situation during 2007-2010. Therefore, there was a gap between HIV diagnosis and initiation of ART, and most PLHIV have access to HIV treatment and care services at late clinical stages. Moreover, this resulted in increasing LTFU, reduced retention rate in HIV treatment and care, and increased morbidity and mortality rates. There was no government support to procure HIV treatment and ensure the sustainability of ARVs. The procurement of ARVs depended only on the donor’s support, so this threatened the life of PLHIV and adherence to ART. Moreover, all laboratory tests that can assess the progress of the disease, such as VL and CD4+ cell count/mm3 have stopped because of the lack of funds that can ensure the availability of reagents and maintenance of machines. The financial resources of donors for AIDS response during internal country conflicts have been reduced and are limited to only covering the availability of ARVs, although mobilization of resources for the humanitarian crisis has increased but was prioritized to cover other humanitarian acts rather than AIDS response.
There is a lack of policies or strategies that can ensure the regular and safe transportation of medicines to governorates where HIV treatment and care clinics exist, contributing to an irregular availability of enough stock of ARVs and their effectiveness and leading to poor treatment outcomes. Moreover, PLHIV have faced difficulties to access HIV treatment and care services during armed conflict especially when they are displaced far from their hometown and during the closure of HIV treatment and care sites. There were no contingency plans developed by MOPHP, NAP, and or governorate health offices to face an emergency. Therefore, HIV treatment and care services stopped operating at hospitals where HIV clinics exist and the doctor, who is the head of the HIV clinic, would dispense ARVs from home. Therefore, it is recommended to include scaling up of services, mainstreaming of HIV and AIDS in different sectors, mobilization of national resources, and formulation of better policies that meet the needs of PLHIV. In addition, the recommendations included the integration of HIV services within the existing health system, improving the tracking systems to avoid LTFU, developing a contingency plan, implementing in-depth studies on HIV treatment outcomes, food support, and income-generating activities.
LIST OF ABBREVIATIONS
| AIDS | = Acquired Immune Deficiency Syndrome |
| ART | = Antiretroviral therapy |
| ARVs | = Antiretroviral drugs |
| CD4+ | = Cluster of differentiation 4 |
| HCP | = Health care providers |
| HIV | = Human Immunodeficiency Virus |
| IDP | = Internally displaced population |
| LTFU | = Loss to follow up |
| MOPHP | = Ministry of Public Health and Population |
| MSM | = Men who have sex with men |
| NAP | = National AIDS Control Program |
| PCR | = Polymerase Chain Reaction |
| PLHIV | = People living with HIV |
| UNAIDS | = Joint United Nations Program on HIV and AIDS |
| VL | = Viral Load |
| WHO | = World Health Organization |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was a doctoral dissertation that was submitted to the Research Ethics Committee, National University of Malaysia, with reference number UKM PPI/111/8/JEP-2016–614.
HUMAN AND ANIMAL RIGHTS
No animals were used for studies that are the basis of this research. This research was conducted on humans were in accordance with the Helsinki Declaration of 1975, as revised in 2013 (http://ethics.iit.edu/ecodes/node/3931).
CONSENT FOR PUBLICATION
All interviewees participated on a voluntary basis after signing informed consent. The right to refuse to participate or to withdraw from the study, anonymity and confidentiality as well as data protection were guaranteed.
STANDARDS FOR REPORTING
STROBE guidelines and methodology were followed.
AVAILABILITY OF DATA AND MATERIALS
The authors confirm that the data supporting the findings of this study are available within the article.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
I would like to express my sincere gratitude and indebtedness to Professor Dr. Sharifa Ezat Wan Puteh for her expert guidance and constant supervision, ever-abiding encouragement, and timely help. I am also grateful to Associate Prof. Dr. Amrizal Muhammad Nur for his guidance and valuable feedback. I am also very grateful to Professor Dr. Zaleha Abdullah Mahdy, Dean of the Faculty of Medicine, who facilitated my PhD journey through the great support I received from her side. Special thanks to the spirit of my father, my brother Ammar and my husband Altegani (may their souls rest in eternal peace), who were with me on this study journey.

